Article Text

Abstract
Background: Measurement of pH in exhaled breath condensate (EBC) is robust and simple. Acidic source fluid (airway lining fluid) traps bases while volatilising acids, leading to EBC acidification in many lung diseases. Lower airway ammonia is one determinant of airway lining fluid pH, raising the concern that addition of the base ammonia by contamination from the mouth might confound EBC pH assays.
Methods: Three discrete methods were used to limit oral ammonia contamination of EBC collections: endotracheal intubation, oral rinsing, and −40°C condenser temperatures. Separately, ammonia was removed from collected EBC samples by lyophilisation and resuspension. Intraweek and intraday variability of ammonia concentration was determined in 76 subjects, and ammonia and pH from a further 235 samples were graphically compared. Ammonia was assayed spectrophotometrically and pH was assessed after deaeration.
Results: Data from 1091 samples are presented. Ammonia was reduced in EBC by all methods. Endotracheal intubation decreased EBC ammonia from a mean (SD) of 619 (124) μM to 80 (24) μM (p<0.001, n = 32). Oral rinsing before collection also led to a decline in EBC ammonia from 573 (307) μM to 224 (80) μM (p = 0.016, n = 7). The colder the condensation temperature used, the less ammonia was trapped in the EBC. Lyophilisation removed 99.4 (1.9)% of ammonia. Most importantly, the pH of EBC never decreased after removal of ammonia by any of these methods. Intraweek and intraday coefficients of variation for ammonia were 64 (27)% and 60 (32)%, which is substantially more variable than EBC pH assays.
Conclusions: Although ammonia and pH appear to correlate in EBC, the oral ammonia concentration is not an important determinant of EBC pH. No precautions need to be taken to exclude oral ammonia when EBC pH is of interest. The low pH and low ammonia found in EBC from patients with lung diseases appear to be independent effects of volatile compounds arising from the airway.
- ammonia
- exhaled breath condensate
- pH
Statistics from Altmetric.com
Exhaled breath condensate (EBC) becomes acidic during airway and lung diseases including asthma,1 cystic fibrosis,2 chronic obstructive pulmonary disease (COPD),3 bronchiectasis,3 acute respiratory distress syndrome,4 the common cold,5 and after partial pulmonary resection.6 Ammonia in EBC is also known to be low in acute asthma.7 It has been shown that low ammonia in EBC is necessary—but not sufficient—for EBC to be acidic.7
The pH of EBC is simple to ascertain and is remarkably robust and reproducible.8 Because ammonia production in the lungs may have an important role in modulating airway pH,7 there has been theoretical, but not data driven, concern that orally derived ammonia might interfere with assessment of pH in EBC.9,10 The work presented in this paper systematically examines the potential of oral ammonia to cause artifact in EBC pH assays.
Oral ammonia was excluded from EBC by three different techniques: (1) bypassing the oropharynx with a cuffed endotracheal tube; (2) rinsing the mouth before sample collection; or (3) condensing exhaled breath as a solid to minimise volatile gas trapping in liquid EBC. In addition, ammonia was removed from EBC by lyophilisation and resuspension of the lyophilate in deionised water. These techniques all substantially reduced EBC ammonia without affecting the measured pH.
METHODS
Subjects
Exhaled breath condensate samples were collected from 32 subjects undergoing elective surgery, from 76 healthy subjects enrolled in a longitudinal study of exhaled biomarkers, and from 10 healthy non-smoking subjects who work within the University of Virginia Health Sciences system (table 1). Samples from the first two subject groups were incorporated into a separate study determining reproducibility of EBC pH and these data have been reported elsewhere.8 An additional 235 EBC samples for which we had obtained both pH and ammonia concentrations were analysed purely for correlation without regard for the underlying disease. Informed consent was given by all subjects, and the protocols were approved by the Human Investigation Committee at the University of Virginia.
Characteristics of study subjects
Sample collection
A total of 1091 EBC samples were assayed. Exhaled breath condensate was collected during oral tidal breathing using the RTube™ EBC collection system (Respiratory Research Inc, Charlottesville, VA, USA) at temperatures as specified for each experiment below. All collections were performed for 10 minutes except the lyophilisation experiment collections which were 20 minutes in order to increase sample volume. Nose clips were not worn. For studies of reproducibility, subjects performed all collections unsupervised in their homes. For comparison between oral and endotracheal collections, subjects provided EBC orally immediately before induction of general anaesthesia and, subsequently, immediately after intubation, confirmation of endotracheal placement, and cuff inflation. For intubated collections the RTube condenser was attached early in the exhalation circuit at the top of the endotracheal tube. Samples were stored at −80°C until assay, except for collections taken at home which were stored initially in home freezers for up to 1 week at approximately −10°C. Assays were performed within 2 months of collection except where noted.
Measurement of pH
pH was assayed with a glass microelectrode (Orion, Beverly, MA, USA) after bubbling 200 μl of the sample with argon at 350 ml/min until the pH reading was stable, as previously described.1
Ammonia assay
Within 2 months of collection, ammonia concentrations in EBC were determined spectrophotometrically using a diagnostic ammonia assay kit (Diagnostic Chemicals Ltd, PEI, Canada). Our standard curves (ammonium chloride in water) were linear down to 20 μM.
Lyophilisation and resuspension of EBC
To remove ammonia from EBC, 1.5 ml aliquots of EBC were lyophilised in 5 ml polypropylene test tubes in a Savant SpeedVac Concentrator (Farmingdale, NY, USA) for 12 hours at +43°C. Immediately thereafter the lyophilates were resuspended to a volume of 1.5 ml with deaerated ultrapure deionised water (>18 megaOhms resistivity) adjusted to pH 7.
Oral rinse
Samples were collected from seven subjects immediately before and after thorough rinsing of the mouth with three 20 ml aliquots of water. EBC collections were performed at an initial condenser temperature of −17°C for 10 minutes each. Salivary pH was not measured.
Altering temperature of EBC collection
Ten subjects provided consecutive 10 minute EBC collections at the following mean temperatures: −44°C, −16°C, −6°C, and +13° C. The temperature of the condenser was kept relatively stable using a modified cooling sleeve for the RTube that contained a chamber into which chemicals with desired temperatures of phase changes were inserted. The phase change from solid to liquid allowed energy to be absorbed from the condensing breath with minimal change in condenser temperature.
Study of reproducibility
Seventy six subjects performed 10 minute EBC collections in their homes before breakfast each morning for seven consecutive days and an additional three collections on the seventh day (before lunch, dinner and bedtime). Initial temperatures of the condenser were between −4°C and −17°C (standard temperatures of home freezers). Ammonia and pH were assayed in all samples in batches.
Statistical analysis
Matched samples of EBC for each study were compared with paired t tests. Multiple comparisons were analysed by one way ANOVA using the Tukey post hoc test. For the study of reproducibility, intraday and intraweek coefficients of variation were calculated for each subject and the means of these results presented. Results are generally presented as mean (SD). Median and range are given where appropriate, and full range is given in addition to mean (SD) when adding that information more clearly communicates the data. Correlations of pH to ammonia concentration and to logarithmically transformed ammonia concentration were performed using Pearson’s product moment. Linear regression was used to compare ammonia assays before and after storage. p values of <0.05 were considered statistically significant.
RESULTS
Reproducibility of ammonia levels in EBC
A total of 760 samples were collected and assayed from 76 subjects. These samples were collected in their own homes unsupervised. The mean intraweek coefficient of variation for EBC ammonia was 64.3 (27.4)% with a full range of intrasubject CVs from 9.6% to 184.5%, and the mean intraday coefficient of variation was 60.4 (32.7)% (full range 1–140.5%). The values of the standard deviations were proportional to the means, and the CVs were therefore similar regardless of the mean measurement. In a subgroup comparison there was no difference in the mean (SD) concentration of ammonia in EBC samples collected unsupervised by healthy subjects in their own homes (481 (281) μM, n = 86) and samples collected from healthy controls in the more controlled circumstances of the laboratory (532 (307) μM, n = 48, p = 0.48). Storage of samples at −80°C had no effect on the ammonia concentration in 10 samples assayed twice 2 months apart, nor in five samples assayed 2 years apart (fig 1).

Ammonia concentration in exhaled breath condensate (EBC) during storage. A total of 15 EBC samples were assayed before and after storage at −80°C (10 samples were frozen for 2 months (closed circles) and five samples for 2 years (open circles)). The plot shows the initial assay and the after storage assay. No differences were identified (r2 = 0.96, p<0.001).
Effect of elimination of oral ammonia by endotracheal intubation on pH of EBC
The mean ammonia concentration in EBC collected orally before intubation was 619 (124) μM which was significantly greater than when the mouth was bypassed by the endotracheal tube (80.2 (24) μM; p<0.001, n = 32). The mean (SD) pH of the EBC in oral collections was 7.9 (0.23) and in the subsequent intubated samples was 7.8 (0.28), (p = NS, fig 2).8

Contribution by the upper and lower airway to EBC ammonia concentrations. Subjects performed oral EBC collections immediately before endotracheal intubation, followed by EBC collection while intubated. EBC collected while intubated had approximately 13% of the ammonia concentration of the matched oral sample (80 (24) μM v 619 (124) μM; *p<0.001, n = 32). There was no difference in EBC pH.
Effect of oral rinsing on EBC ammonia and pH
The mean (SD) ammonia concentration in EBC collected from seven subjects before oral rinsing was 573 (307) μM and the pH was 8.0 (0.2). Immediately after oral rinsing the ammonia concentration declined to 224 (80) μM (p = 0.016; n = 7). Despite the reduction in ammonia, the pH of the EBC remained unchanged at 8.0 (0.1), p = NS (fig 3).
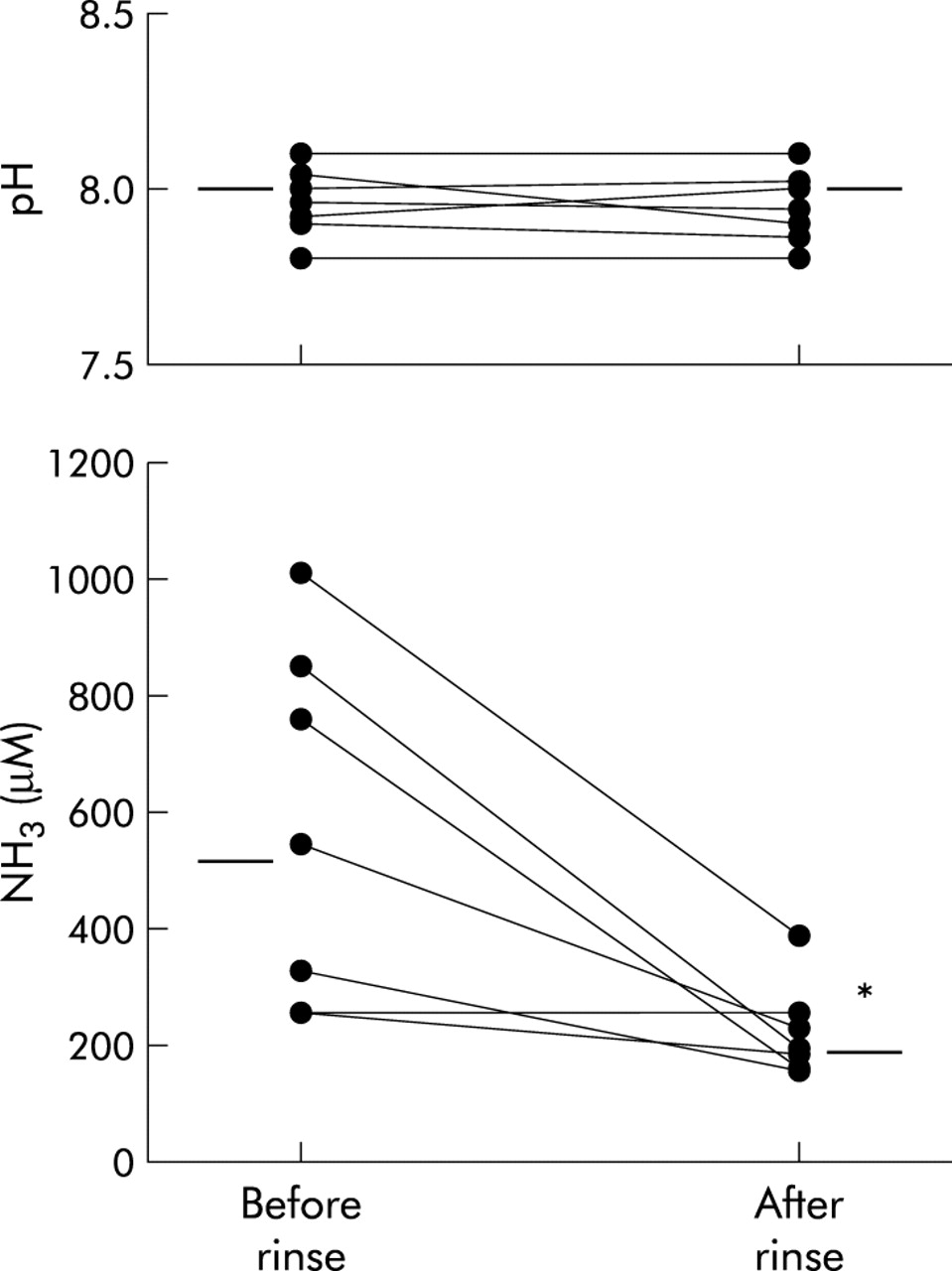
Oral rinsing before EBC collection decreased ammonia without affecting EBC pH. Subjects provided EBC samples immediately before and then after rinsing their mouth thoroughly with water (pH <7). The concentration of ammonia fell from 573 (307) μM to 224 (80) μM after oral rinsing (*p = 0.016, n = 7). The pH of the EBC remained unchanged at 8.0 (0.1), p = NS.
Effect of very low temperatures on EBC ammonia and pH
Ten subjects provided back to back 10 minute EBC collections at the following temperatures: +13°C, −6°C, −16°C, and −44°C in no set order. The mean ammonia concentration in the EBC depended on collection temperature (697 (442) μM at +13°C, 534 (473) μM at −6°C, 451 (218) μM at −16°C, and 140.2 (99.4) μM at −44°C; fig 4). By ANOVA, these ammonia concentrations were significantly different (p = 0.002) between collections at +13°C and −44°C and between −6°C and −44°C. Despite the decreased concentration of ammonia at the lowest temperatures, the pH of the EBC remained identical irregardless of the temperature of collections (pH = 7.9 (0.2), 7.9 (0.3), 7.9 (0.3), 7.8 (0.3) respectively; p = NS), as previously reported.8

Effect of temperature on ammonia concentrations in EBC. Subjects provided consecutive EBC collections at four different condenser temperatures. Ammonia levels in EBC progressively declined at the lower collection temperatures (*p = 0.002, n = 10). The pH of the EBC was unaffected by removal of ammonia.
Effect of lyophilisation and resuspension on EBC ammonia
The median ammonia concentration before lyophilisation of the sample was 628 μM (range 100–1760 μM, n = 10) and the pH = 7.9. Lyophilisation was very successful at purging ammonia from the EBC. When the lyophilate was resuspended in deionised water, ammonia was undetectable (<20 μM) in 9/10 samples. Resuspension of lyophilate in pH 7 adjusted deaerated deionised water was performed before repeated pH measurement. The pH of this reconstituted EBC was 8.1 (p = 0.023, n = 10), higher than the original sample despite complete removal of ammonia (fig 5).

Effect of removal of all ammonia from EBC by lyophilisation on pH of the sample. EBC samples underwent lyophilisation and resuspension in deionised water (pH = 7). Ammonia was essentially completely removed by this process (n = 10). The pH rose slightly in the reconstituted samples despite removal of the base (*p⩽0.023).
Correlation of ammonia and pH in EBC samples
Data from an additional 235 samples collected during the course of various investigations into EBC were used to compare ammonia and pH in EBC without regard for any underlying disease. Figure 6 shows that the ammonia concentrations in EBC were low when the pH was low. There was a weak but significant correlation between log transformed ammonia and pH (correlation coefficient = 0.52, p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Low levels of ammonia in EBC are necessary but not sufficient for low EBC pH to be present. Low ammonia levels occur both in low and high pH samples.
DISCUSSION
Exhaled breath sampling for assessment of airway disease is increasing in utility and application. The biochemistry of the airway now can be repeatedly assessed during illnesses with methodology that can measure trace concentrations of volatile and non-volatile substances that egress from the human lung.11 Interpretation of the multiple markers of disease in EBC, as is true for exhaled nitric oxide, needs to be wise and circumspect. With the field of non-invasive lung biochemistry measurement still in its infancy, it is expected that there will be debates as well as occasional erroneous interpretations and mistaken theories. Indeed, it seemed likely that contamination of EBC with oral ammonia would have an important alkalinising effect in EBC. Figure 6 could be interpreted to show that pH depends on the ammonia concentration; however, our empirical data dispel that incorrect notion. In fact, no acidification of EBC could be accomplished despite complete removal of oral ammonia by endotracheal intubation, partial removal of oral ammonia by oral rinsing, and partial and complete removal of total respiratory ammonia by low temperature condensation or post-collection lyophilisation. Absence of a base does not an acid make.
Oral ammonia appears to have no relevant effect on the pH of EBC. Nonetheless, respiratory ammonia may be important for airway pH and lung disease. Firstly, airway ammonia can neutralise inhaled environmental acids, protecting the airway from injury.12 Secondly, the glutaminase pathway of epithelial ammonia and bicarbonate production is the only currently identified (although assuredly not the only existent) airway pH homeostatic process7—that is, glutaminase increases production of base equivalents when airway lining fluid pH falls. If the glutaminase system and other pH homeostatic mechanisms fail, or if acidifying mechanisms are activated, airway lining fluid pH will fall. Ammonia (including that inhaled from the mouth) will then be trapped as non-volatile ammonium (NH4+) and will not egress from the airway for subsequent capture in EBC. In this manner, the absence of ammonia in EBC appears to serve as a highly (indeed, overly) sensitive signal of low airway pH. Thus, if EBC ammonia is low, this can mean either that it is being formed in smaller quantities or that it is being trapped by the acidic fluid. Similarly, low EBC pH indicates that more acids are being exhaled, either because there are more acids being formed in the airway or because the airway is acidic, allowing acids to be more volatile. Although low ammonia production in the airway (by glutaminase, for example) may lead to a low airway lining fluid pH, it is clear that a low NH3 concentration in the EBC is not the cause of a low EBC pH. Instead, our data support the notion that both of these characteristics of EBC may be independently controlled by airway lining fluid pH—which, in turn, is controlled by many factors including glutaminase.
The correlations we found between EBC ammonia and EBC pH reflect not cause and effect but, rather, the independent effect of a low source fluid pH on enhancing volatility of acids (then trapped in EBC and lowering its pH), while minimising the volatility of ammonia (which is then not exhaled and therefore not trapped in EBC). Molecular pathways and effects of airway acidification have been reviewed recently.13
That ammonia is not the relevant controller of EBC pH is additionally supported by the slight but significant increase in pH in lyophilised and reconstituted EBC samples. Lyophilisation successfully removed the ammonia but, given the increase in pH despite removal of this base, it seems likely that one or more volatile acids were also removed by lyophilisation. These acids are the real controllers of EBC pH and are likely to be the relevant acids when EBC pH is very low, as occurs during lung diseases.
Although EBC ammonia is stable over time in storage and the assays are simple, inexpensive, and sufficiently sensitive, the poor same subject reproducibility of EBC ammonia can be problematic. Although the lower airways make a substantial contribution to EBC ammonia, most arises from the upper airways. (This is also true for exhaled nitric oxide but is often overlooked.14) The oral contribution to ammonia can be affected by eating and drinking before collection, which is also similar to exhaled nitric oxide.15 In addition, technical issues such as the temperature of the device condenser affect EBC ammonia levels. These technical issues are not a concern for EBC pH assays.8 As a result, the reproducibility of EBC ammonia measurements compares poorly with the excellent reproducibility of EBC pH, which is less than 5% for intraday and intraweek sampling and 0.5% for back to back collections.
Based on our data, we expect that neither delay in performing the ammonia assay nor collecting the sample at home instead of in the laboratory would adversely influence the reproducibility of the ammonia concentrations. Our extensive data reveal that oral ammonia is not an important determinant of EBC pH. As a corollary, oral ammonia does not adversely affect or seem to interfere with EBC pH assays. No special efforts are necessary to exclude oral ammonia when the pH of EBC is of interest. The pH of EBC has become an important characteristic that is enhancing our understanding of airway biochemistry during disease states. Because of their simplicity, ammonia assays may cautiously be used to complement pH assays in large studies, especially when subjects are intubated. The search for the specific acids that are released from the airway and lung during various diseases continues. Although the identification of the acids that cause EBC acidification may lead to recognition of previously unconsidered pathways of airway and lung disease development, the simple notion that the airway pH deviates in diseases in itself has substantial implications for airway pathophysiology.
REFERENCES
Footnotes
-
This work was supported by the United States National Institutes of Health R01 HL72429-01 and the American Academy of Allergy, Asthma and Immunology Education and Research Trust.
-
Conflict of interest: JV and JH are minority shareholders of Respiratory Research Inc, the company that manufactures the exhaled breath condensate collection equipment used in this study.