Article Text

Abstract
Background: It has been proposed that the pH of airway lining fluid may regulate the fractional exhaled concentration of nitric oxide (FeNO) in respiratory disease.
Methods: FeNO, exhaled breath condensate (EBC) pH, and EBC concentrations of nitrite plus nitrate (NO2/NO3) were compared in 12 subjects with stable asthma, 18 with stable cystic fibrosis (CF), and 15 healthy control subjects. Eight of the CF patients were studied on a separate occasion at the start of a pulmonary exacerbation.
Results: FeNO was significantly greater in asthmatic subjects than in control subjects (mean 35 v 9 ppb, p<0.001). EBC pH, however, was similar in the asthmatic and control groups (median 5.82 v 6.08, p = 0.23). Levels of NO2/NO3 were on average higher in EBC samples from asthmatic subjects, but the difference was not significant. In patients with stable CF both the FeNO (mean 4 ppb, p<0.001) and EBC pH (median 5.77, p = 0.003) were lower than in the control group. Levels of EBC NO2/NO3 (median 29.9 μM; p = 0.002) in patients with stable CF, in contrast, were significantly higher than in control subjects. During CF exacerbations, EBC pH was further reduced (median 5.30, p = 0.017) but FeNO and NO2/NO3 were unchanged.
Conclusions: These findings demonstrate a dissociation between EBC pH and FeNO in inflammatory airways disease.
- CF, cystic fibrosis
- EBC, exhaled breath condensate
- FeNO, fractional exhaled concentration of nitric oxide
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- NO, nitric oxide
- PD20, provocative dose of methacholine required to produce a 20% fall in FEV1
- asthma
- cystic fibrosis
- exhaled breath condensate
- nitric oxide
Statistics from Altmetric.com
- CF, cystic fibrosis
- EBC, exhaled breath condensate
- FeNO, fractional exhaled concentration of nitric oxide
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- NO, nitric oxide
- PD20, provocative dose of methacholine required to produce a 20% fall in FEV1
Since the initial report that nitric oxide (NO) can be detected by chemiluminescence in exhaled air of humans,1 a large body of literature has accumulated describing the expression of NO in the respiratory tract in health and disease. In the absence of corticosteroid treatment, the fractional exhaled concentration of NO (FeNO) is raised in adults2–4 and children5 with allergic asthma. The FeNO in asthma is further increased during acute exacerbations and falls with response to treatment.6 In cystic fibrosis (CF), on the other hand, the FeNO has been reported to be either lower than,5,7 or similar to,8,9,10 that in healthy control subjects and not to change during pulmonary exacerbations.10,11
Endogenous NO may be synthesised during conversion of the amino acid l-arginine to l-citrulline by enzymes of the nitric oxide synthase (NOS) family.12 Three distinct isoforms of NOS, encoded by separate genes, have been cloned and characterised. Neuronal NOS (nNOS) or NOS1 and endothelial NOS (eNOS) or NOS3 generate relatively small (picomolar) amounts of NO that are believed to play a homeostatic role in many physiological processes. Inducible NOS (iNOS) or NOS2, in contrast, produces much higher (nanomolar) levels of NO at sites of inflammation. Although transcriptionally regulated by proinflammatory stimuli, iNOS is constitutively expressed in normal human airway epithelium.13 Consistent with the changes in FeNO, epithelial expression of iNOS mRNA and protein is increased in allergic asthma14–16 whereas iNOS immunostaining is reduced in the airway epithelium in CF.17,18
Recent controversy has centred on the potential ability of airway lining fluid pH to regulate FeNO independently of NOS activity. Hunt et al19 collected exhaled breath condensate (EBC) from patients hospitalised with acute asthma and found that the pH was over two log orders lower than that of non-asthmatic control subjects. The degree of acidification was shown to be sufficient to generate NO non-organically from nitrite (NO2) in vitro. These authors therefore proposed that pH might be an important determinant of FeNO. In subsequent work, low EBC pH has also been described in CF, chronic obstructive pulmonary disease (COPD), and bronchiectasis.20,21 However, direct comparisons of EBC pH and FeNO have not been made in any of these studies.
We have therefore further examined the relationship between exhaled NO and airway acidification in inflammatory airway disease. Our aim was to establish whether alterations in EBC pH and FeNO were necessarily associated or could occur independently of each other. To address this, we compared FeNO, EBC pH, and EBC NO2 and nitrate (NO3)—stable end products of NO metabolism—in subjects with asthma, in subjects with CF, and in healthy control subjects.
METHODS
Subjects
The study population comprised 12 subjects with atopic asthma, 18 patients with stable CF, and 15 healthy control subjects. Asthma was defined according to American Thoracic Society criteria.22 Subjects in this group had mildly symptomatic and clinically stable disease. None was a cigarette smoker. They were receiving treatment with inhaled β2 agonists as required but none had taken inhaled or oral corticosteroids or any other form of preventative anti-asthma medication within at least 6 weeks of the study. Patients with CF had the diagnosis confirmed by genotype analysis, with the homozygous ΔF508 mutation identified in 12 cases. They were all taking vitamin supplements, pancreatic enzyme supplements, and inhaled or nebulised β2 agonists as necessary. In addition, 12 CF patients were receiving treatment with nebulised antibiotics (colistin or gentamicin), three with nebulised DNase, and nine with an inhaled corticosteroid (budesonide or fluticasone propionate). One subject in the CF group was a cigarette smoker. Eight of the 18 CF patients were studied on a separate occasion within 3 days of the start of a pulmonary exacerbation. For the purpose of the study, a pulmonary exacerbation was defined empirically on the basis of clinical characteristics (increase in cough, breathlessness, sputum volume, or sputum purulence) in combination with a requirement for intravenous antibiotics, as judged by the supervising clinician. The control group consisted of healthy non-smoking non-atopic volunteers with no respiratory symptoms and no history of lung disease. All control subjects had normal spirometry and normal airway responsiveness.
The study was approved by the local research ethics committee and all subjects provided written informed consent.
Skin prick testing
Skin prick testing was performed with the following allergens: Dermatophagoides pteronyssinus, Dermatophagoides farinae, mixed grasses, cat allergen, and dog allergen (Allergopharma, Reinbek, Germany). Atopy was defined as a positive response (weal diameter 3 mm or more greater than the saline control at 15 minutes) to at least one of these.
Pulmonary function
Spirometric tests were performed with a Vitalograph compact spirometer (Vitalograph Ltd, Buckingham, UK). Subjects receiving inhaled bronchodilators were asked to withhold these for at least 6 hours. Airway responsiveness was measured in accordance with European Respiratory Society (ERS) guidelines23 using a flow controlled nebuliser and dosimeter system (Jaeger Toennies GmbH, Hochberg, Germany). Subjects inhaled increasing doses of methacholine from 0.0256 to 1.44 mg. The provocative dose of methacholine required to produce a 20% fall in forced expiratory volume in 1 second (FEV1PD20) was calculated by linear interpolation from the logarithmic dose-response plot.
Measurement of FeNO
FeNO was measured using a chemiluminescence analyser (LR2500 series; Logan Research Ltd, Rochester, UK). Nose clips were applied immediately before the manoeuvre to prevent nasal exhalation. Subjects exhaled at a constant flow rate of 250 ml/s in accordance with ERS recommendations.24 Measurements of FeNO were taken from the plateau at the end of exhalation, as determined by simultaneous monitoring of CO2. The procedure was repeated three times and the mean value taken. The machine was calibrated before each use with standard calibration gases.
Collection and analysis of EBC
EBC was collected using a device which consisted of a mouthpiece and a two-way non-rebreathing valve connected by polypropylene tubing to a glass Dreschel flask immersed in crushed ice, acting as a condensing chamber. Subjects breathed at a normal frequency and tidal volume for 15 minutes while wearing nose clips, allowing collection of 1.5–2.5 ml of condensate. The pH was measured immediately with a benchtop pH meter (Fisher Scientific Instruments, Loughborough, UK). Vaughan et al25 have recently shown that, at least in the case of deaerated specimens, EBC pH measurements are highly reproducible and independent of condenser temperature, ventilatory pattern, duration of collection, and degree of airway narrowing. In the present study, EBC samples were not deaerated but in preliminary experiments the pH was shown to remain stable for at least 5 minutes after collection. For subsequent assay of NO2 and total NO2 plus NO3 (NO2/NO3), EBC was frozen in 250 μl aliquots at −80°C. After thawing, 500 μl samples were spun at 13000 rpm for 30 minutes in a centrifugal filter device with a 10 kDa molecular weight cut off (Microcon YM-10; Millipore Corporation, Bedford, MA, USA). Concentrations of NO2 and of NO2/NO3 in filtrates were determined in duplicate using a commercially available colorimetric assay kit according to the manufacturer’s instructions (Cayman Chemical Company, Ann Arbor, MI, USA). The detection limit was approximately 1 μM. All samples underwent a single freeze-thaw cycle.
Statistical analysis
Subjects’ ages, spirometric measurements, and FeNO data were expressed as mean (SD). Data for EBC pH and for NO2 and NO2/NO3 concentrations were expressed as median (range). Comparisons between asthmatic and control groups and between stable CF and control groups were undertaken using an unpaired t test or Mann-Whitney U test, as appropriate. Comparisons of paired data for CF patients in stable disease and in exacerbation were performed with a paired t test or Wilcoxon test, as appropriate. In the case of NO2, some values were below the detection limits of the assays and were therefore assigned an arbitrary value of 0 for the purpose of analysis. Correlations were sought using Pearson’s test or Spearman’s test for normally and non-normally distributed data, respectively. Statistical analysis was performed using StatView 5.01 for Macintosh (Abacus Concepts, Berkeley, CA, USA) and CIA version 2.1.1 software (University of Southampton, Southampton, UK).
RESULTS
The clinical and physiological details of the subjects studied are summarised in table 1. Spirometric values in patients with CF were lower on average during acute exacerbations than in stable disease, but the differences were not statistically significant. Asthmatic subjects exhibited varying degrees of airway hyperresponsiveness whereas control subjects all had airway responsiveness in the non-asthmatic range. Methacholine bronchoprovocation was not performed in patients with CF.
Clinical and physiological characteristics of study subjects
The FeNO was significantly greater in subjects with asthma than in healthy control subjects (35 (19) v 9 (4) ppb, difference between means 26 ppb (95% CI 15 to 36); p<0.001, fig 1). The EBC pH, however, was similar in the asthmatic and control groups (5.82 (5.19–6.33) v 6.08 (5.58–6.64), median difference −0.18 (95% CI −0.43 to 0.11); p = 0.23, fig 2). Concentrations of NO2 in these EBC samples were below the measurable range (<1 μM) except in five cases (two asthmatic and three non-asthmatic) where it was present at low levels (fig 3). Levels of NO2/NO3 were on average higher in EBC samples from asthmatic subjects, but the difference did not reach statistical significance (21.1 (<1–63.3) μM v 11.4 (<1–67.3) μM, median difference 12.3 (95% CI −3.8 to 28.1) μM; p = 0.17). There were no significant correlations between FeNO, EBC pH, EBC NO2/NO3 levels, and physiological indices in either the asthmatic or the control group.

Measurements of FENO in control subjects (n = 15), subjects with mild stable atopic asthma (n = 12), subjects with stable CF (n = 14), and subjects with CF during exacerbation (n = 7). Horizontal bars represent mean values. For technical reasons, data were unavailable for four of 18 CF subjects during stable disease and for one of eight CF subjects during exacerbation. Comparisons were performed using paired and unpaired t tests, as appropriate.

Measurements of EBC pH in control subjects (n = 15), subjects with mild stable atopic asthma (n = 12), subjects with stable CF (n = 18), and subjects with CF during exacerbation (n = 8). Horizontal bars represent median values. Paired and unpaired data were compared using the Mann-Whitney and Wilcoxon tests, respectively.
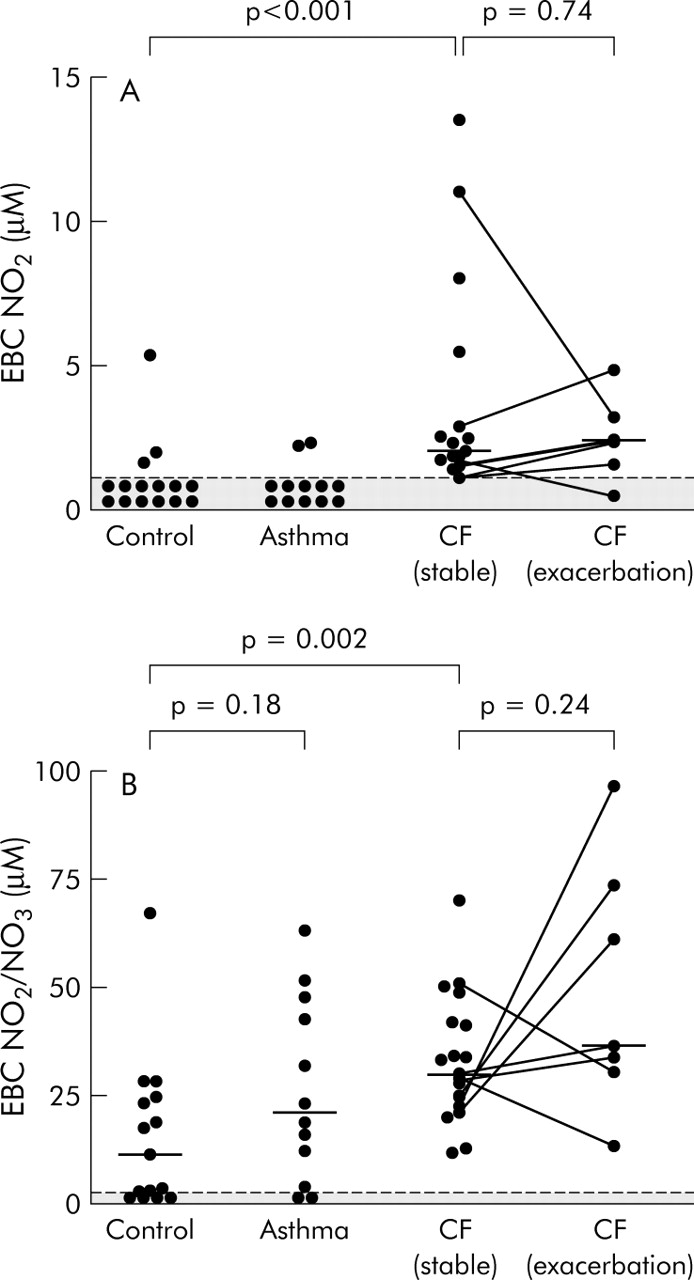
Measurements of (A) EBC NO2 and (B) NO2/NO3 in control subjects (n = 15), subjects with mild stable atopic asthma (n = 12), subjects with stable CF (n = 17), and subjects with CF during exacerbation (n = 7). For technical reasons, data were unavailable for one of 18 CF subjects during stable disease and for one of eight CF subjects during exacerbation. Horizontal bars represent median values. Paired and unpaired data were compared using the Mann-Whitney and Wilcoxon tests, respectively.
In stable CF the FeNO was significantly lower than in the control group (4 (3) v 9 (4) ppb, difference between means −6 ppb (95% CI −3 to −8); p<0.001, fig 1), as was the EBC pH (5.77 (4.81–6.99) v 6.08 (5.58–6.64), median difference −0.34 (95% CI −0.61 to −0.12); p = 0.003, fig 2). In contrast, levels of EBC NO2 in stable CF were significantly higher than in control subjects (2.0 (1.1–13.5) μM v <1 (<1–5.4) μM, median difference 1.9 (95% CI 1.4 to 2.5) μM; p<0.001), as were levels of NO2/NO3 (29.9 (11.9–51.0) μM v 11.4 (<1–67.3) μM, median difference 19.7 (95% CI 8.7 to 28.2) μM; p = 0.002, fig 3). There were direct correlations between FeNO and both FEV1 % predicted (r = 0.64, p = 0.012) and FVC % predicted (r = 0.53, p = 0.049; fig 4), but no significant correlations between EBC pH, NO2, or NO2/NO3 and these physiological parameters. There was a further fall in EBC pH during CF exacerbations compared with stable disease (5.30 (4.99–5.86) v 5.77 (4.81–6.99), median difference −0.53 (95% CI −1.16 to −0.11); p = 0.017), but no significant change in FeNO (3 (2) v 4 (3) ppb, difference between means 0 ppb (95% CI −2 to 2); p = 0.91). Levels of EBC NO2 (2.4 (<1–4.8) μM) and NO2/NO3 (36.6 (13.5–96.5) μM) during CF exacerbations were higher than in stable disease, but not significantly so.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlations between FENO and (A) FEV1 % predicted and (B) FVC % predicted in subjects with stable CF (n = 14). Statistical analysis was performed using Pearson’s test.
DISCUSSION
Collection of EBC is attracting increasing interest as a novel method of sampling lower airway lining fluid. Compared with techniques such as bronchoalveolar lavage (BAL) and sputum induction, EBC offers the advantages that it is safe, inexpensive, non-invasive, may be repeated at frequent intervals, and can be performed by children and the elderly. Previous reports of disturbances of EBC pH in various forms of respiratory disease have led to speculation regarding the relationship between airway pH and exhaled NO. To our knowledge, however, this is the first study directly to compare EBC pH and FeNO in the same individuals.
In subjects with mild stable allergic asthma not receiving treatment with corticosteroids, we found that the FeNO was raised and that levels of EBC NO2/NO3 were also on average higher than those of control subjects. In contrast, the EBC pH was normal. The mechanism of the raised FeNO in these asthmatic subjects does not therefore appear to be acidification of endogenous NO2. A more likely explanation is the increased expression of iNOS that has previously been reported in asthmatic airways.14–16 Further support for an enzymatic source of exhaled NO derives from the observation that non-selective NOS inhibitors such as NG-nitro-l-arginine methyl ester (l-NAME) and NG-monomethyl-l-arginine (l-NMMA) produce a marked reduction in FeNO in asthmatic (and also non-asthmatic) subjects.26
The increased FeNO in subjects with mild asthma is consistent with a number of earlier studies,2–4 and the values that we have measured are in agreement with those previously reported. Some studies have also described significant increases in NO2 and/or NO2/NO3 concentrations in EBC19,27,28 and induced sputum29 in asthma. In the present study, NO2 was below the limit of detection in most samples and NO2/NO3 measurements were variable, with the difference between groups not statistically significant. These findings are consistent with our previous observations in BAL fluid where levels of NO2 and of NO3 were similar in healthy control subjects, mild non-steroid treated asthmatics, and the same asthmatic subjects following treatment with fluticasone propionate (NO2: medians 0.74, 0.97, and 0.45 μM; NO3: 15.1, 16.5, and 15.4 μM; A E Redington, unpublished data). The normal EBC pH in asthma in the present study is consistent with the data of Kostikas et al20 who reported that EBC pH was decreased in moderate, but not mild, asthma. Similarly, Hunt et al19 found that the low EBC pH in acute asthma rapidly normalised with anti-inflammatory treatment. A reduction in EBC pH—and perhaps, by inference, a contribution of airway acidification to FeNO—appears therefore to be a feature only of more severe disease, not of mild asthma.
In contrast to the situation in asthma, we found that stable CF was associated with acidification of EBC and that a further reduction in EBC pH occurred during acute pulmonary exacerbations. Despite the presence of NO2 and NO3 reserves in quantities that were higher than in control subjects, the reduced pH did not lead to an increase in FeNO. On the contrary, FeNO levels in CF were significantly reduced, both in stable disease and during acute pulmonary exacerbations, consistent with previous reports.5,7,9–11 These findings indicate that airway acidification, as assessed by EBC pH, does not necessarily increase NO generation, even in the presence of plentiful NO2 reserves. They confirm and extend the findings of Tate et al21 who also demonstrated acidification of EBC in CF but did not measure FeNO. Furthermore, the observation that FeNO was reduced in CF whereas levels of NO2 and NO2/NO3 were increased argues against the possibility that these latter constituents are generated by oxidation of NO ex vivo.
Several mechanisms may be considered to explain the reduced EBC pH in CF. Although its role is still not well defined, cystic fibrosis transmembrane conductance regulator (CFTR) facilitates HCO3− secretion in the pancreas and there is also evidence of apical HCO3− conductance by CFTR in cultured human airway epithelial cells.30,31 Defective epithelial HCO3− transport in CF could therefore lead to lumenal acidification. However, individual EBC pH data points for one patient with the heterozygous mutation R117H/ΔF508, a genotype associated with significant retention of HCO3− conductance,32 did not represent outliers. Furthermore, a low EBC pH is not specific for CF but appears rather to be a more general feature of inflammatory airways disease, suggesting a role for leucocyte infiltration and activation. Stable CF is associated with predominantly neutrophilic airway inflammation and the degree of sputum neutrophilia is more pronounced during pulmonary exacerbations.33 Neutrophil activation has been linked to pH reduction in animal models of pleural sepsis,34 and the EBC pH in COPD is inversely correlated with induced sputum neutrophil counts.20 Finally, buffering of airway lining fluid in CF might be impaired by an inflammation dependent reduction in epithelial glutaminase expression and NH3 generation, as has been described in acute asthma.35
The mechanism underlying the low FeNO in CF, despite the presence of chronic airways infection and inflammation, is uncertain. Firstly, inhaled corticosteroid treatment (which was being taken by nine of the 18 CF patients in contrast to none of the asthmatic or control subjects) must be considered as a possible confounding factor. FeNO measurements did not differ significantly between those CF patients who were receiving inhaled corticosteroids and those who were not (mean 5 v 3 ppb), although the possibility of a type II error cannot be excluded. Previous studies of the effect of corticosteroids on FeNO in CF have produced conflicting findings.8,36 Secondly, the excess secretions and mucus in CF airways may inhibit the diffusion of gaseous NO into the airway lumen. This would be consistent with the positive correlations that we have demonstrated between FeNO and spirometric measurements in stable CF, as more advanced lung disease is presumably associated with increased retention of mucus. It is also in keeping with the increased EBC levels of NO2 and NO2/NO3 in CF demonstrated here and in other studies of NO metabolites in EBC21,37 or sputum.11,38 Finally, there may be a primary defect in NO production in CF. Expression of iNOS is decreased in CF airway epithelium,17,18 and the presence of a low FeNO in infants with newly diagnosed disease39 suggests that this is not simply a consequence of inflammation. Moreover, experiments in human tracheal epithelial cells in vitro and in CFTR deficient mice have shown that loss of functional CFTR results in reduced epithelial iNOS expression and NO generation.40
Theoretical concerns have been raised about whether EBC measurements are truly reflective of the lower airways in terms of pH and concentrations of non-volatile solutes. Firstly, fluid formation involves the dilution of aerosolised droplets by condensed exhaled water vapour and the degree of dilution, as estimated from condensate electrolyte concentrations, can be both substantial and highly variable.41 Currently, there is no readily available dilutional marker that can be used to calculate absolute concentrations of non-volatile solutes in lower respiratory tract lining fluid. Despite this, their relative concentrations in EBC may serve to provide information about the presence and activity of disease processes. This would be consistent with recommendations for interpreting solute concentrations in BAL fluid,42 where a reliable dilution marker is also lacking. A second concern has been that exhaled ammonia, derived mainly from the mouth, might influence condensate pH independently of processes in the lower airways.41 Against this, the pH of undiluted tracheal secretions obtained during bronchoscopy is almost identical to same-subject EBC collections19 and, at least in the absence of respiratory disease, similar observations have been made in EBC collected from isolated lower airways.25
In conclusion, we have shown that mild stable atopic asthma is associated with a normal EBC pH and an increased FeNO in contrast to CF where the EBC pH is low, particularly during acute exacerbations, but FeNO is reduced. These findings demonstrate a dissociation between EBC pH and FeNO in inflammatory airways disease. They also draw attention to the complexity of NO metabolism, where multiple pathways of NO synthesis and clearance are likely to have variable relevance in different circumstances.
Acknowledgments
The authors thank the CF nurse specialists Tanya Moon and Julie Mould for help with data collection and Fiona Lampe for statistical advice.