Article Text

Abstract
Background: Inhalation of hypertonic or even isotonic saline during sputum induction may cause bronchospasm in susceptible patients with asthma, despite premedication with 400 µg inhaled salbutamol delivered by pressurised metered dose inhaler (pMDI). The bronchoprotection afforded by additional inhaled salbutamol administered through the ultrasonic nebuliser during sputum induction was investigated.
Methods: Twenty patients with moderate to severe asthma underwent sputum induction by inhaling saline 4.5% (or 0.9% if post-bronchodilation forced expiratory volume in 1 second (FEV1) <65% predicted) for 10 minutes according to two protocols given 1 week apart in random order. At visit A the patients received 400 µg salbutamol administered through a pMDI + spacer 20 minutes before induction while at visit B the premedication was supplemented by 1500 µg nebulised salbutamol inhaled throughout the induction procedure. Both the investigator and the patients were blind to the nebulised solution used. FEV1 was recorded during sputum induction at 1, 3, 5, and 10 minutes. Sputum cell counts and histamine, tryptase and albumin levels in the supernatants were determined.
Results: The mean (SE) maximal reduction in FEV1 over the 10 minute period of sputum induction was 11.7 (2.8)% at visit A, which was significantly greater than at visit B (2.6 (1.2)%; mean difference 9% (95% CI 2.7 to 15.4), p<0.01). Total and differential sputum cell counts as well as albumin, tryptase, and histamine levels did not differ between the two visits.
Conclusion: The addition of inhaled salbutamol through an ultrasonic nebuliser markedly improves bronchoprotection against saline induced bronchoconstriction in patients with moderate to severe asthma undergoing sputum induction without affecting cell counts and inflammatory markers.
- asthma
- bronchoprotection
- salbutamol
- nebulisation
- sputum induction
Statistics from Altmetric.com
Since the first description of sputum induction by Pin et al in 1992,1 the technique has been widely used in asthma research. Although several studies have reported on the methodology of sputum induction,2 some outstanding issues with respect to the safety of the procedure remain. Inhalation of hypertonic saline carries the risk of severe bronchoconstriction in patients with bronchial hyperresponsiveness,3 and hypertonic saline challenge is a recognised indirect challenge to assess bronchial hyperresponsiveness in asthma.4 This has led to the recommendation of using inhaled salbutamol 200–400 μg before sputum induction in patients with asthma unless measurement of bronchial responsiveness to saline is an outcome of the study.5 In most studies inhaled salbutamol has been delivered by pressurised metered dose inhaler (pMDI), some authors combining the pMDI with a spacer to improve lung deposition. Despite this type of premedication, some asthmatic patients still experience breakthrough bronchoconstriction. One way to reduce the risk of bronchoconstriction is to induce sputum by inhalation of isotonic rather than hypertonic saline, as advocated by Pizzichini et al for severe asthmatic exacerbations.6 However, even isotonic saline may be sufficiently irritating to the airways to trigger bronchospasm in asthmatic patients with very reactive airways. The dose of salbutamol and the optimal way to deliver it remains an issue for the safety of sputum induction.5
We hypothesised that delivering salbutamol via ultrasonic nebuliser together with isotonic or hypertonic saline may provide better bronchoprotection than inhaled salbutamol pMDI 400 µg alone administered through a Volumatic chamber. We have assessed 20 patients with moderate to severe asthma and compared the falls in forced expiratory volume in 1 second (FEV1) that occurred during sputum induction when subjects were premedicated with either salbutamol pMDI (400 µg) or salbutamol pMDI (400 µg) + nebulised salbutamol delivered throughout the induction procedure. To ensure that nebulised salbutamol does not affect the key indicators in the sputum we compared the two induction procedures with respect to sputum cell counts and several biochemical markers—albumin as an indicator of plasma exudation and tryptase and histamine as markers of mast cell activation—two activities that may theoretically be influenced by β2 agonists.7
METHODS
Subjects
Twenty patients with moderate to severe asthma diagnosed according to ATS criteria8 were recruited from outpatient clinics. Three had been admitted to hospital and five others had received a course of systemic corticosteroids for a severe asthma exacerbation during the previous year. The demographic and functional characteristics of the subjects are shown in table 1.
Demographic and functional characteristics of study subjects
Sixteen subjects received regular treatment with inhaled corticosteroids, 11 of whom were also receiving inhaled long acting β2 agonists. Two subjects were also on oral corticosteroids with a daily dose of 16 and 32 mg methylprednisolone, respectively. Maintenance treatment was kept constant over the 4 weeks preceding the study (table 2). The protocol was approved by the local ethical committee and volunteers gave their written informed consent.
Treatment characteristics of study subjects
Study design
This was a randomised crossover study. There was a run in period during which subjects recorded their daily consumption of relief bronchodilators into diary cards. Subjects were randomised to receive either inhaled salbutamol 400 µg administered through pMDI and Volumatic (Glaxo Smith Kline, UK) 20 minutes before sputum induction (visit A) or the same regimen + additional nebulised salbutamol 1571 µg during the sputum induction procedure (visit B). Both the asthmatic subjects and the laboratory function technician who performed sputum induction and spirometric tests were blind to the inhaled solution used. The two sputum inductions were separated by a period of 1 week and were performed at the same time of the day (±2 hours). There was no change in the maintenance treatment between inductions and subjects were allowed to take their usual maintenance drugs (including long acting β2 agonists) on the morning of the induction. Importantly, the mean consumption of short acting bronchodilator during the preceding week and the baseline lung function values before sputum induction were similar between visits A and B (table 2).
FEV1 was measured as the best of three flow-volume curves using an electronic spirometer (Spirobank, MIR, Rome, Italy) before and 15 minutes after 400 µg inhaled salbutamol, the latter value being considered as the baseline value.
Sputum induction was started with either hypertonic or isotonic saline according to post-bronchodilator FEV1. Patients with an FEV1 ⩾65% predicted inhaled 4.5% saline while those with FEV1 <65% predicted were given 0.9% saline instead. Two patients had a post- bronchodilator FEV1 slightly less than 65% predicted at visit A (62% and 64% predicted, respectively) but more than 65% at visit B (66% and 67% predicted, respectively). As visit A was the first visit for these two patients, they also inhaled isotonic saline at their second visit (visit B) for consistency.
Sputum induction
Saline was inhaled through an ultrasonic nebuliser (Devilbiss 2000), the mean output of which was calculated to be 0.93 ml/min. The cup of the nebuliser was filled with 50 ml hypertonic/isotonic saline to which was added 1.75 ml salbutamol solution at 5 mg/ml. The dose of nebulised salbutamol was dependent on the duration of sputum induction and was calculated by multiplying the concentration of salbutamol in the cup of the nebuliser (169 µg/ml) by the output of the nebuliser (0.93 ml/min) and the duration of the induction. FEV1 was measured at 1, 3, 5, and 10 minutes after starting inhalation. Inhalation of saline was stopped after 10 minutes or when a fall in FEV1 of >20% from baseline had occurred. After performing spirometric measurements at 5 and 10 minutes the subjects were asked to rinse their mouth with tap water and to cough up sputum into a plastic container. For safety reasons, FEV1 was measured 10 and 20 minutes after the end of the induction in every patient. Two subjects who still had a fall in FEV1 of >20% at this time received additional nebulised salbutamol and ipratropium bromide and were kept under observation until their FEV1 value had returned to within 5% of baseline.
Sputum processing
Samples were poured into a 50 ml polypropylene tube, weighed, and diluted with a threefold weight of a phosphate buffered saline (PBS) solution for homogenisation. The samples were then rocked at room temperature for 20 minutes and centrifuged at 400 g for 10 minutes at 4°C. The supernatant was stored at –80°C until biochemical analyses for albumin and histamine. The cellular phase was dispersed in 1 ml PBS without Ca2+ and Mg2+ solution for total cell counts using a manual haemocytometer. The differential cell count was performed on cytospins stained with Diff-Quick by counting 500 cells under a light microscope.
Biochemical assays
Albumin was measured by rocket electrophoresis as previously described.9 Histamine was measured by RIA (Immunotech, Marseille, France) with a sensitivity of 0.02 ng/ml. Tryptase was measured by an immunoassay (UniCAP, Pharmacia, Uppsala, Sweden) with a sensitivity of 1 ng/ml.
Statistical analyses
Changes in FEV1 during sputum induction were expressed as mean (SE), and sputum cell counts and biochemical markers as median (range). Assessment of the significance of a bronchoconstriction during the sputum induction for each procedure was performed using a one sample Student’s t test. Comparisons of the maximal falls in FEV1 between the two procedures were performed by a paired Student’s t test. Comparisons of sputum cell counts and biochemical markers between the two procedures were performed by the Wilcoxon rank sum test, whereas reproducibility was assessed by calculating the intraclass coefficient of correlation as previously described.10 p values of <0.05 were considered statistically significant. Given the repeatability of the functional and biochemical parameters and setting a risk error α at 0.05, our sample size had a power of 98%, 96%, 82%, and 84% to detect a 50% inhibition in the fall in FEV1 and of the sputum levels of albumin, histamine and tryptase, respectively.
RESULTS
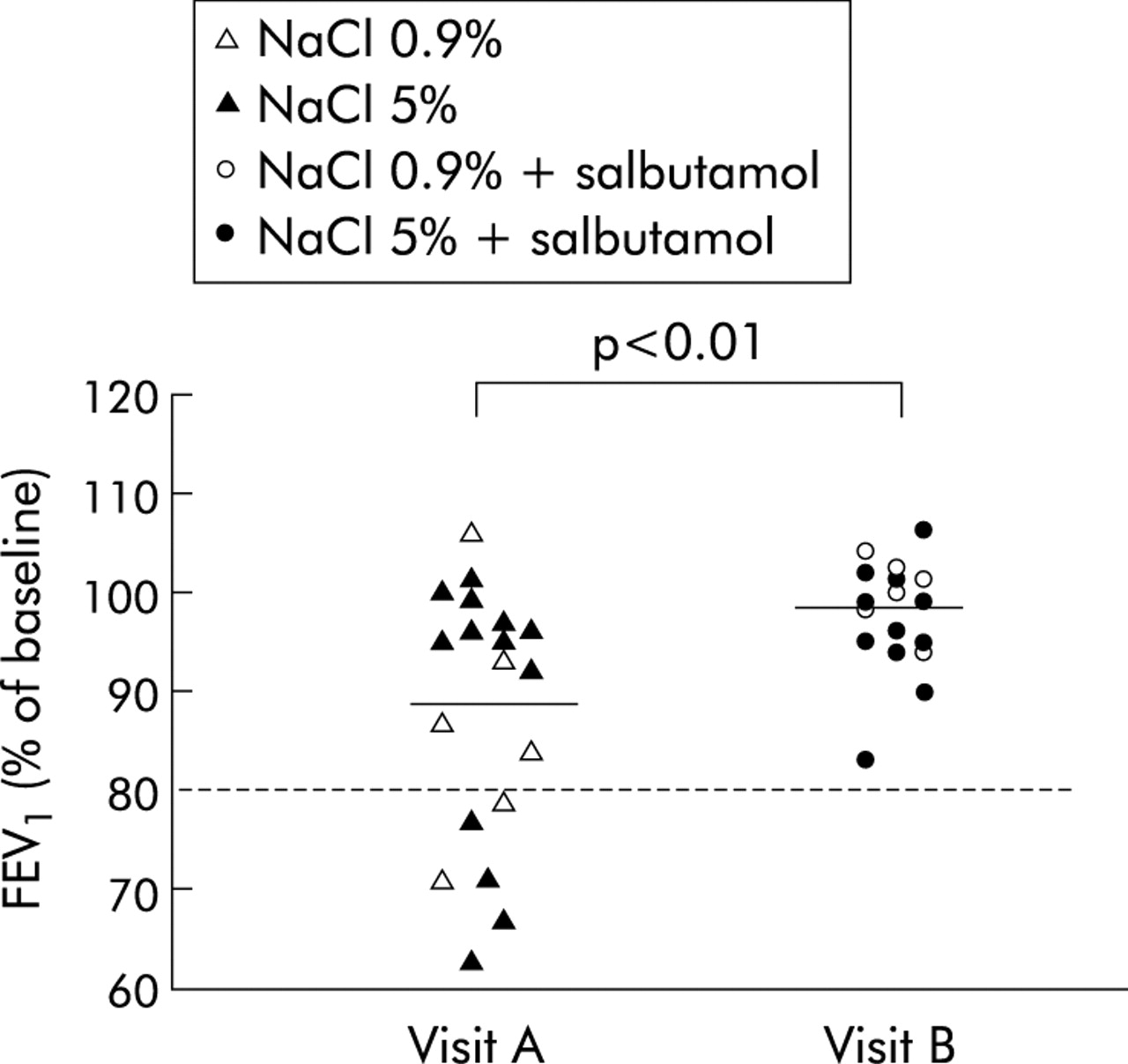
There was no significant difference between post-bronchodilator FEV1 values measured before starting sputum induction on visits A and B (table 1). All the subjects inhaled saline for 10 minutes on both occasions. Sputum induction caused significant bronchospasm that peaked at 10 minutes and reached 10.4 (3.2)% (p<0.01) when subjects were premedicated with 400 μg salbutamol inhaled through a pMDI and spacer (visit A). In contrast, inhalation of the same amount of saline did not produce any significant fall in FEV1 when the patients received nebulised salbutamol in addition to conventional premedication (visit B, fig 1). The maximal fall in FEV1 over the 10 minute period was 11.7 (2.8)% at visit A and 2.6 (1.2)% at visit B (fig 2). The mean (95% CI) difference for the maximal fall in FEV1 between visits A and B was 9% (2.7 to 15.4), p<0.01. Six of the 20 patients had a fall in FEV1 of >20% at 10 minutes when premedicated with the conventional procedure while none reached this threshold when receiving nebulised salbutamol.
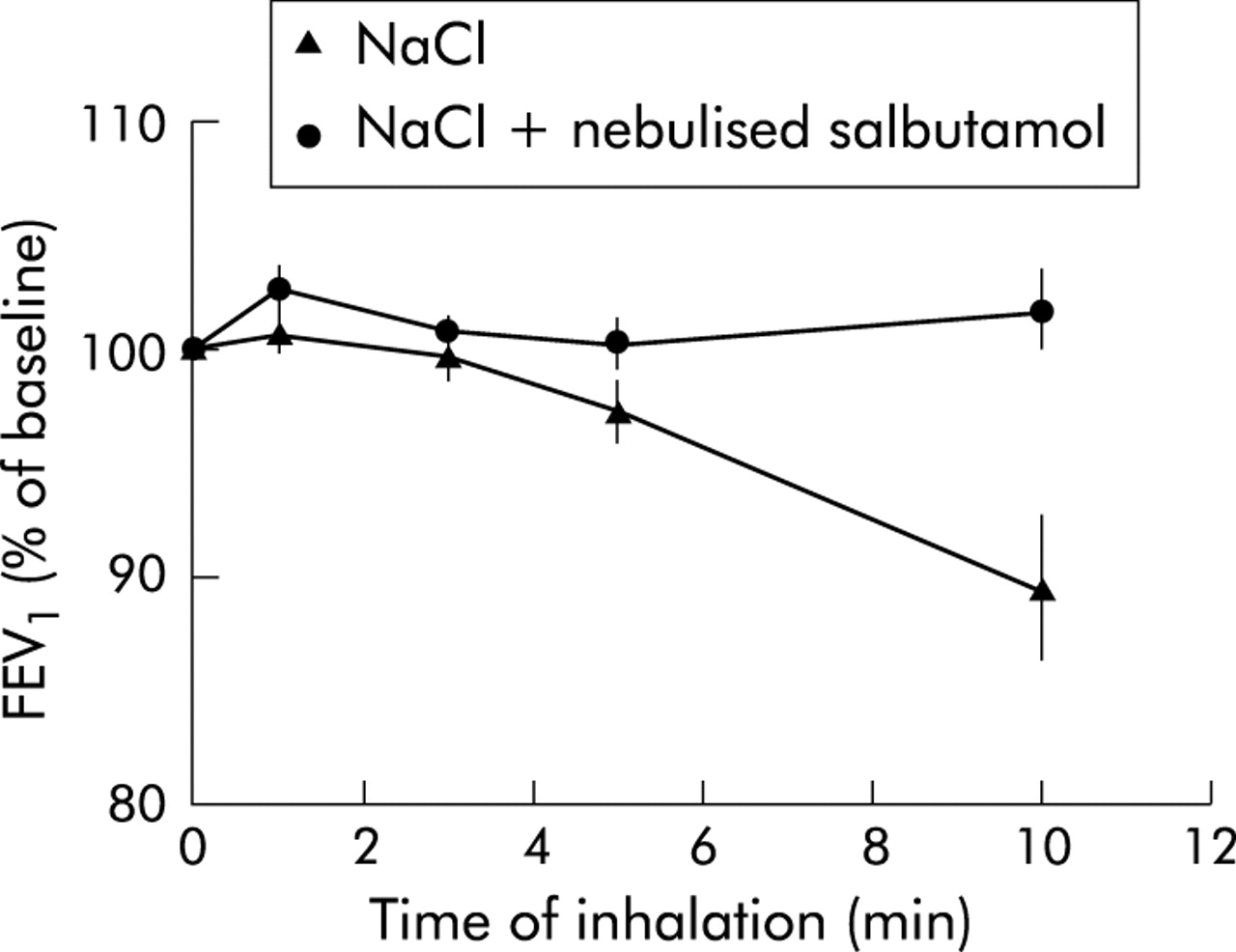
Time course of bronchoconstriction during sputum induction by inhalation of hypertonic or isotonic saline in 20 patients with moderate to severe asthma. Results expressed as mean (SE) values.

Distribution of the maximal falls in forced expiratory volume in 1 second (FEV1) at visit A (NaCl) and visit B (NaCl + nebulised salbutamol).
At visit A the mean maximal fall in FEV1 was 11.1 (3.6)% (p<0.05, one sample t test) in patients who inhaled hypertonic saline and 13.2 (4.9)% (p<0.05) in patients who inhaled isotonic saline (post-bronchodilator FEV1 <65% predicted). The magnitude of the falls in FEV1 with the conventional procedure was inversely related to baseline FEV1 (r = −0.46, p<0.05) and directly related to both the extent of bronchodilation after inhaled salbutamol 400 μg (r = 0.58, p<0.01) and the consumption of β2 agonist in the preceding week (r = 0.44, p = 0.05).
At visit A, patients who were regularly treated with long acting β2 agonists (n = 11) had a fall in FEV1 of 11.2 (3.8)% compared with 12.5 (4.5)% in those not treated with long acting β2 agonists (n = 9). When receiving nebulised salbutamol, the fall in FEV1 was 2.4 (1.7)% in patients on regular treatment with long acting β2 agonists and only 3 (1.6)% in patients not so treated (fig 3).

{kind=link}
{kind=link}
{kind=link}
Comparison of the maximal falls in FEV1 between patients treated and not treated with long acting β2 agonists (LABA).
Mean (SE) FEV1 values measured 10 and 20 minutes after the end of sputum induction at visit A were 7.1 (1.9)% and 4.3 (2.4)%, respectively. Two subjects still had a fall in FEV1 of more than 20% by this time which was quickly reversed to less than 5% of baseline by nebulised salbutamol (2500 µg) and ipratropium bromide (250 µg). At visit B there was no late bronchoconstriction following sputum induction since mean FEV1 values remained above 95% of baseline at 10 and 20 minutes.
Although 18 patients produced an adequate sputum sample on at least one occasion, only 15 produced readable samples on both occasions allowing for comparison between the two procedures. Sputum induction failed in two patients at visit A and in two others at visit B. One patient was unable to produce any sample at any visit. In the patients who produced two adequate samples there was no significant difference between sputum cell counts and sputum albumin, tryptase and histamine levels measured at either visit (table 3).
Sputum cell counts and biochemical markers
DISCUSSION
This study shows that the addition of salbutamol 1500 µg in the ultrasonic nebuliser during sputum induction reinforces the bronchoprotection obtained with 400 µg inhaled salbutamol through pMDI in patients with moderate to severe asthma. Improved bronchoprotection is observed irrespective of current treatment with long acting β2 agonists. In addition, inhalation of a high dose of salbutamol does not modify cellular and mediator activity in the airway inflammatory process as evidenced by sputum cell counts, and albumin, tryptase and histamine levels.
Our data confirm that inhaling hypertonic and even isotonic saline carries the risk of significant bronchospasm in moderate to severe asthmatics despite premedication with salbutamol 400 µg delivered by pMDI, which highlights the need to improve the safety of the procedure. We have shown that complementary salbutamol (1500 µg) inhaled through an ultrasonic nebuliser markedly reduces the intensity of bronchospasm seen in patients with moderate to severe asthma undergoing sputum induction. None of the 20 patients studied had a fall in FEV1 of more than 20% during sputum induction when receiving nebulised salbutamol compared with six patients who had a fall in FEV1 of more than 20% (range 20.3–37.2%) at the end of sputum induction when only receiving 400 µg inhaled salbutamol through pMDI. In our study the rate of significant bronchospasm (30%) with standard premedication is slightly higher than that reported by Fahy et al (14%) in a recent multicentre study of asthmatics whose baseline FEV1 values were very similar to those of our subjects.11
In agreement with previous studies,12,13 we found that both baseline FEV1 values and β2 agonist consumption are parameters that may influence the magnitude of bronchospasm following inhalation of saline. It is therefore worth noting that these two parameters were similar between visits A and B, making comparison between the two study days valid. The relationship between the dose of inhaled salbutamol and the extent of bronchoprotection has only been studied over a narrow range of concentrations so far. Bel and colleagues14 showed that salbutamol 200 and 400 µg inhaled through a pMDI were both very efficient in shifting to the right the concentration of histamine or methacholine provoking a fall in FEV1 of 20% or more (PC20) with a small dose related effect for PC20 histamine but not for PC20 methacholine.14 Inhalation of salbutamol 100–400 µg by MDI produces strong bronchoprotection against methacholine that is, however, weakly proportional to the dose since 80% of protection is already achieved with 100 µg.15 On the other hand, inhalation of 1600 µg salbutamol dry powder on top of regular treatment with salmeterol (50 µg twice daily) or formoterol (12 µg twice daily) did not increase the bronchoprotection towards methacholine. The inability of a dose of salbutamol similar to the one we used and administered through a dry powder inhaler to further improve the bronchoprotection given by long acting β2 agonists16 therefore suggests that, in our study, the ultrasonic nebulisation itself may well reinforce the bronchoprotection obtained with salbutamol.
By showing no difference in the magnitude of bronchospasm induced by saline inhalation between patients with and without long acting β2 agonists, our results indicate that it would be unwise to consider that asthmatic patients are always protected against saline induced bronchoconstriction when regularly treated with long acting β2 agonists. The tolerance in bronchoprotection produced by chronic usage of β2 agonists may be involved.17 However, it should be kept in mind that the patients in our study who received long acting β2 agonists also suffered from more severe asthma, exhibiting the poorest baseline lung function, and were therefore the most likely to show a dramatic change in FEV1 after saline.
It is interesting that the delivery of high dose salbutamol into the airways does not alter the profile of sputum cells nor its albumin, tryptase and histamine content. Inhalation of hypertonic saline may trigger mast cell degranulation18 and favour vascular leakage19 into the airways. On the other hand, there is evidence in the literature that β2 agonists can prevent mast cell degranulation and inhibit plasma exudation.7 As these two properties may theoretically partly contribute to the bronchoprotective effect of β2 agonists,20 we wished to determine whether inhalation of a high dose of salbutamol, compared with a low dose, has any effect on the sputum content of mast cell derived mediators and a marker of plasma exudation. Our results show that high dose salbutamol had no effect on the levels of histamine, tryptase, or albumin. This suggests that the greater bronchoprotective effect of high dose salbutamol is neither related to mast cell stabilisation nor to the anti-exudative effect during sputum induction.
This study shows that additional inhalation of salbutamol through an ultrasonic nebuliser improves the safety of sputum induction in patients with moderate to severe asthma without altering its cellular and biochemical content. We believe that this may be of practical importance to the investigation of airways inflammation in patients with moderate to severe asthma.