Article Text

Abstract
Background: Leukotrienes play a key role in the pathophysiology of chronic asthma. Activation of leukotriene pathways is accompanied by rises in detectable urinary levels of leukotriene E4 (LTE4). The relationship between urinary LTE4 levels and factors associated with acute asthma has not been determined.
Methods: Adults aged 15–54 years presenting with moderate to severe acute asthma were evaluated at emergency departments in 16 US sites. Forced expiratory volume in 1 second (FEV1) was measured during the first 60 minutes after arrival and at specified times until discharge or admission. Urine samples for measurement of LTE4 levels were obtained either on arrival at the study site and/or before discharge. Patients were seen 2 weeks later for follow up, at which time repeat FEV1 measurements and urine samples for LTE4 were obtained.
Results: One hundred and eighty four patients were evaluated; LTE4 results from both the acute and follow up periods were available for analysis in 146. Urinary LTE4 levels were increased during asthma exacerbations compared with levels obtained 2 weeks later (geometric means 111.7 and 75.6 pg/mg creatinine, respectively, mean percentage change −32.3; 95% confidence interval (CI) for the mean percentage change −39.6 to −24.3, p<0.001). The correlation between improvement in FEV1 and decline in LTE4 over the 2 week interval was significant (p<0.001, r = 0.43).
Conclusions: Activation of leukotriene pathways in acute asthma is correlated with the degree of airflow obstruction, and resolution of the asthma exacerbation is associated with a reduction in leukotriene levels.
- asthma
- urinary leukotrienes
- montelukast
Statistics from Altmetric.com
Over the last two decades the incidence of asthma in both children and adults has risen worldwide.1,2 All individuals with asthma are at risk of an acute exacerbation of their disease requiring urgent or emergency department treatment.3 While international asthma management guidelines have been designed to control asthma symptoms and reduce asthma exacerbations, a recent study suggests that 17% of patients with acute asthma experience relapse attacks within 2 weeks.4 Although the factors underlying asthma exacerbations and relapses are complex, a better understanding of the pathology associated with asthma attacks may lead to improved treatments and reduced morbidity.
Cysteinyl leukotrienes (LTC4, LTD4, LTE4) play an important role in the pathogenesis of asthma. Leukotrienes are produced by mast cells, eosinophils, and other airway inflammatory cells and increase vascular permeability, constrict bronchial smooth muscle, and mediate bronchial hyperresponsiveness.5 Levels of urinary LTE4, the stable metabolite of LTC4 and LTD4,6,7 are increased in children8 and adults9 with asthma compared with healthy controls and in asthmatics after bronchial challenge with antigen,10,11 after oral challenge with aspirin in aspirin sensitive asthmatic subjects,12 and during exercise induced bronchospasm.13 The importance of leukotrienes in the pathology of asthma has been further demonstrated in large clinical trials with agents that block the actions of leukotrienes. For example, montelukast, a potent leukotriene receptor antagonist taken orally once daily, significantly improves asthma control in both children (aged 2–14 years)14,15 and adults16 and attenuates exercise induced bronchoconstriction.17,18
While leukotrienes play an important role in chronic asthma, activation of the leukotriene pathway in acute asthma is less well defined. Raised levels of LTE4 have been detected in the urine of patients during an asthma exacerbation or status asthmaticus,19,20 but the number of patients available for analysis was small. We have recently conducted a clinical trial comparing the effect of adding intravenous montelukast 7 or 14 mg or placebo to standard treatment in patients with moderate to severe asthma exacerbations.21
This study was undertaken to analyse the activation of leukotrienes in these patients during their treatment in the emergency department and at 14 days follow up, and to determine whether the degree of airflow limitation is correlated with activation of the leukotriene pathway.
METHODS
Patients
Sixteen US sites, primarily emergency departments affiliated with academic medical centres, participated in the study. Adults aged 15–54 years presenting with acute asthma were screened for enrolment in the study. Participants were required to have a history of asthma for at least 1 year, a history of tobacco use of less than 10 pack years, and no concomitant treatment with systemic corticosteroids, leukotriene modifiers, anticholinergic agents, or long acting β agonist bronchodilators. Patients with pneumonia, congestive heart failure, or other clinical explanations for dyspnoea were excluded, as were patients with significant co-morbid disorders requiring acute management. The study protocol was approved by each investigator’s respective Institutional Review Board and all patients gave written informed consent to participate.
Study design
The primary study examined the benefit of adding intravenous montelukast to standard treatment for adults with moderate to severe acute asthma; the benefit of intravenous montelukast in this setting has been reported elsewhere.21 Briefly, the study consisted of a screening period, active treatment period, and a 2 week follow up after discharge. The screening period began when the patient arrived in the emergency department and lasted up to 60 minutes. During the screening period patients were treated with short acting β agonists (albuterol (salbutamol) 2.5 mg by nebuliser) and oxygen. Patients also underwent an initial spirometric test (Puritan Bennett model PB-100) followed by albuterol nebulisation (a total of two albuterol nebulisations were allowed during the screening period) and a second spirometric test. Each spirometric test was performed and interpreted in accordance with the reproducibility and acceptability criteria of the American Thoracic Society.22 Patients whose forced expiratory volume in 1 second (FEV1) was more than 70% of the predicted value23 on either spirometric test were excluded. In addition, patients were excluded if the FEV1 (expressed as a percentage of the predicted value) increased or decreased by ⩾20 percentage points between the two measurements.
Patients included in the study received blinded treatment (intravenous montelukast or placebo) and, in addition, continued treatment with β agonists at the investigator’s discretion. When indicated, corticosteroids were administered at a standard dose (prednisone 60 mg orally). Serial spirometric tests were performed at selected times for up to 6 hours or until a decision was made for discharge or admission, whichever occurred first. All patients successfully discharged from the emergency setting were given a standard course of oral prednisone (50 mg/day for 5 days) and were scheduled for a follow up visit 14 (SD 3) days later, at which time the FEV1 measurement was repeated.
Urinary LTE4 measurements
As an exploratory objective of the main study, spot urine samples were obtained during the acute treatment period and at the follow up visit for those patients successfully discharged from the study site. Urine samples were placed on ice within 20 minutes, then frozen for analysis within 4 hours of collection. Urinary LTE4 levels were analysed by reversed phase liquid chromatography after precolumn extraction combined with radioimmunoassay as described elsewhere.24 The results were normalised to the creatinine concentration determined in the same sample.
Evaluations and statistical analyses
Data on urinary LTE4 levels were skewed so the analysis of urinary LTE4 levels was performed after applying a log transformation. Geometric means and 95% confidence intervals (CI) were used to summarise back transformed data. Pearson coefficients of correlation between percentage predicted FEV1 and LTE4 levels (at entry and follow up) and between change in LTE4 levels and change in percentage predicted FEV1 were computed. Regression models including other explanatory variables (sex, age, race, smoking status, allergic rhinitis history, years since asthma diagnosis, and treatment during the acute treatment phase) were also fitted to the LTE4 levels. Comparisons of LTE4 levels by subgroup of patients based on their FEV1 were performed using a t test.
RESULTS
A total of 274 patients were screened for enrolment; 201 were randomised for the study, 184 had LTE4 measurements either during the acute or the follow up phases, and 146 had LTE4 levels available for analysis from both phases. The major reason for exclusion was failure to meet spirometric criteria (57 of 73 patients (78%)). Of these, 49 were excluded because FEV1 was >70% of the predicted value (before or after albuterol) and eight were excluded because FEV1 (expressed as percentage predicted) increased by >20 percentage points following albuterol nebulisation.
Baseline characteristics of the patients are presented in table 1. Most patients enrolled in the study had moderate to severe asthma exacerbations (FEV1 <50–60% of the predicted value).25 The mean FEV1 before the start of the study was 1.6 l, corresponding to 47% of the predicted value. It should be noted that the baseline value was determined after patients had received initial treatment with β agonists and/or oxygen, so the pre-study baseline value most probably overestimated the FEV1 upon arrival at the study site, which was not measured at that time.
Demographic data and baseline characteristics of patients
LTE4 levels during the acute exacerbation or at the 2 week follow up visit were not significantly different between the group which received the single dose of intravenous montelukast (n = 123) and those who received placebo (n = 61; p = 0.36), a result that was not unexpected given that montelukast is a receptor antagonist and has no effect on leukotriene synthesis. Subsequent analyses were thus performed on pooled data between the treatment groups in order to explore the relationship between LTE4 levels and other clinical measures associated with asthma exacerbations.
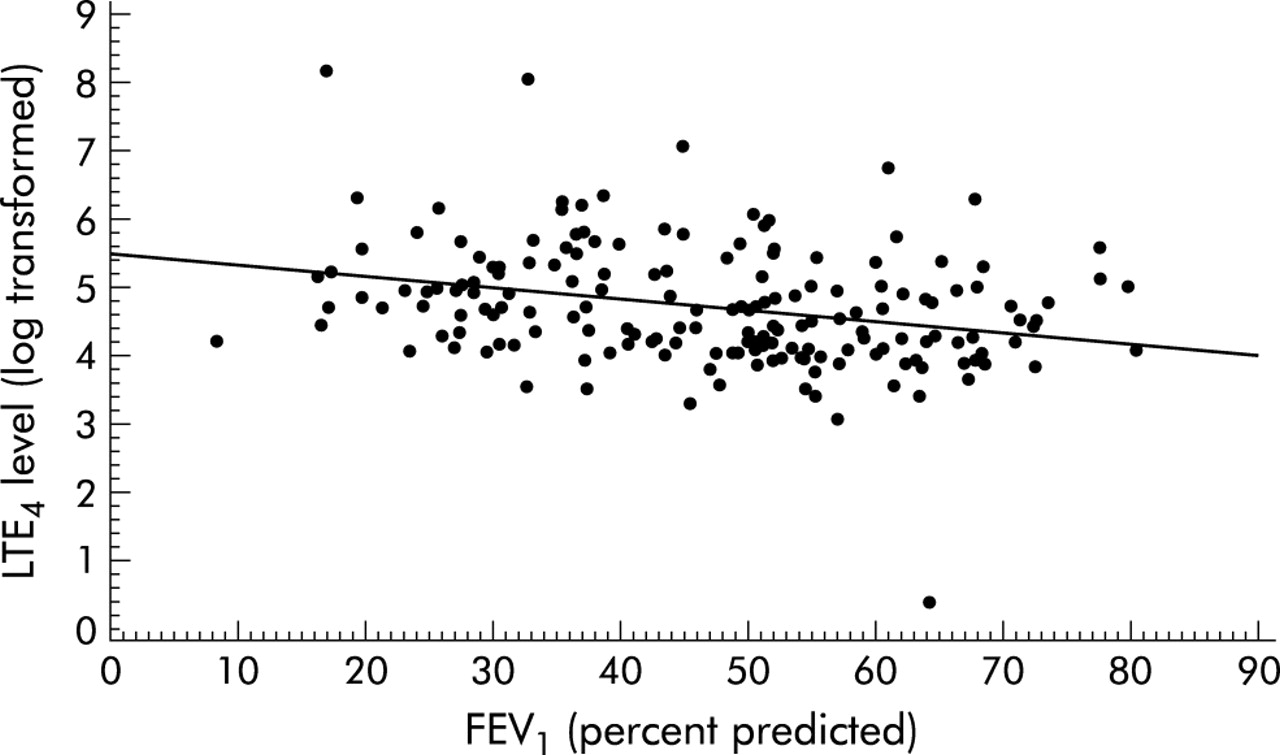
Urinary LTE4 levels were increased during asthma exacerbations compared with levels obtained 2 weeks later (geometric means 111.7 and 75.6 pg/mg creatinine, respectively), a mean percentage change of −32.3% (95% CI −39.6 to −24.3), p<0.001 (fig 1). Regression analysis of LTE4 levels and FEV1 during the acute exacerbation showed that LTE4 levels increased as FEV1 decreased (fig 2); the coefficient of correlation was equal to −0.29 (95% CI −0.42 to −0.15). The median percentage predicted FEV1 at baseline for all patients was 49%. During the acute phase LTE4 levels were significantly higher (p<0.001) in patients with a baseline FEV1 of <49% of the predicted value than in patients with FEV1 ⩾49% (table 2). At the 2 week follow up evaluation LTE4 levels decreased in both groups while the median percentage predicted FEV1 at the 2 week follow up increased to 66%. The coefficient of correlation between LTE4 levels and FEV1 at follow up was −0.35 (95% CI −0.48 to −0.20) (fig 3). LTE4 levels were still significantly higher in the subpopulation of patients with greater airflow limitation (FEV1 <66%) than in patients with less airflow limitation (FEV1 ⩾66%; p<0.001; table 2).
Urinary LTE4 levels in acute asthma and at follow up by subgroup of percentage predicted FEV1 (</⩾ median)

Change in urinary LTE4 levels during an acute asthma attack compared with levels at follow up for all patients with available data at both time points (n = 146). The difference between the two measurements was significant (p<0.001). Data are expressed as geometric mean (95% confidence intervals).
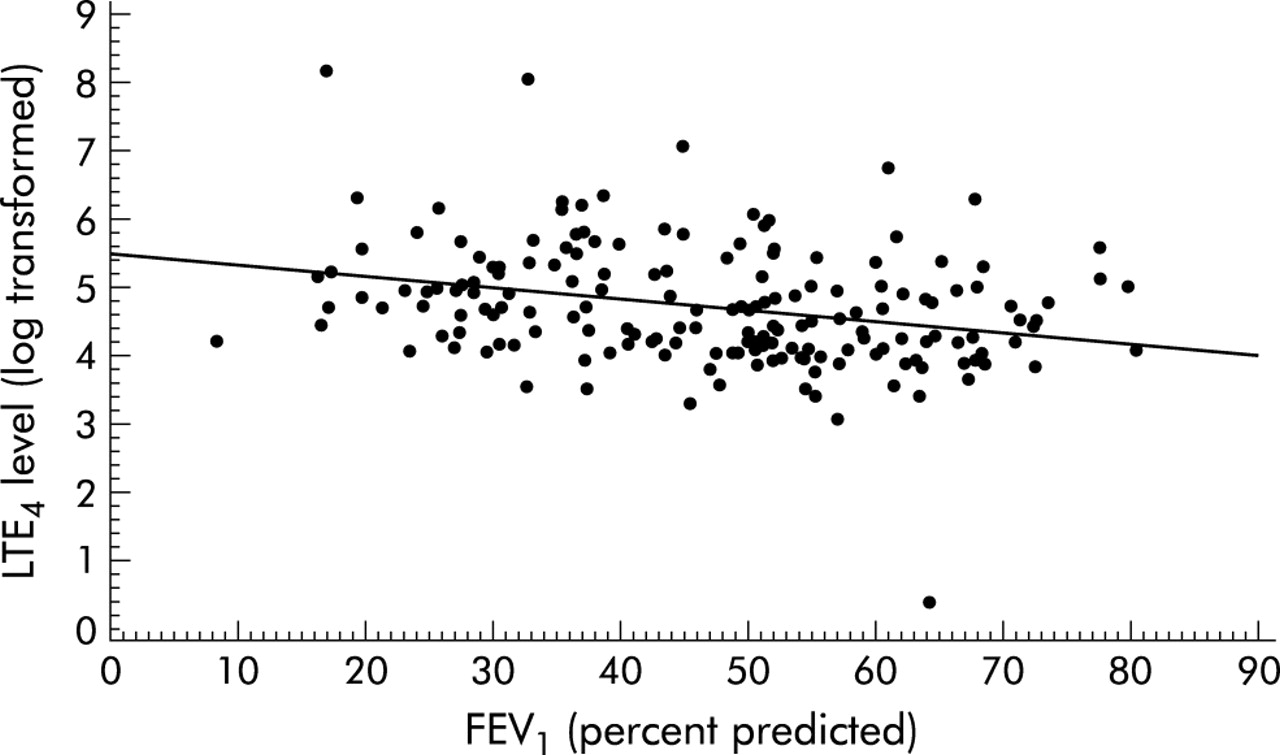
Regression analysis of baseline acute urinary LTE4 levels (log transformed) and percentage predicted FEV1 values; r = −0.29 (95% confidence interval −0.42 to −0.15).

Regression analysis of follow up urinary LTE4 levels (log transformed) and percentage predicted FEV1 values; r = −0.35 (95 % confidence interval −0.48 to −0.20).
Regression analysis showed that the change in LTE4 levels from acute to follow up correlated with the change in percentage predicted FEV1 (r = −0.43 (95% CI −0.55 to −0.28), fig 4). The median change in percentage predicted FEV1 from acute presentation to follow up was 18%. Patients with a change in FEV1 of ⩾18% from acute presentation to follow up had a significantly greater decrease in LTE4 than patients with a change in FEV1 of <18% (table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Regression analysis of change in urinary LTE4 levels (log transformed) from acute to follow up versus change in percentage predicted FEV1 values; r = −0.43 (95% confidence interval −0.55 to −0.28).
In order to determine the influence of baseline characteristics on LTE4 levels, regression analyses were performed using patient history in addition to pulmonary function measurements. Inclusion of sex, age, smoking status, allergic rhinitis history, or years since asthma diagnosis in the models described above did not increase the precision of the estimate of LTE4 levels compared with models with predicted FEV1 alone. Although one time treatment with intravenous montelukast was associated with a significant improvement in FEV1 during the acute exacerbation compared with placebo,21 this did not translate into differences in the change in LTE4 or FEV1 over the 2 week follow up interval.
DISCUSSION
In this study acute exacerbations of asthma were accompanied by increased levels of LTE4 in urine followed by a significant decrease during resolution. The degree of airflow limitation was correlated with levels of urinary LTE4 during both the exacerbation and follow up periods. These data suggest that the leukotriene pathway is activated during acute asthma and that leukotrienes play an important role in the pathophysiology of acute asthma.
Previous studies have shown that individuals without asthma have a mean urinary LTE4 concentration of approximately 80 pg/mg creatinine.26 In the current study the mean urinary LTE4 concentration was 75.6 pg/mg creatinine at the follow up visit, which suggests that LTE4 levels had normalised within 2 weeks of the asthma exacerbation. In contrast, urinary LTE4 levels obtained during the exacerbation were substantially higher (111.7 pg/mg creatinine).
Our study included urinary LTE4 levels from over 140 patients during acute asthma and after resolution. The findings confirm the results of previous studies in smaller numbers of patients which have also suggested that urinary leukotriene levels are raised during an asthma exacerbation.19,20,27 For example, Drazen and colleagues measured urinary LTE4 levels in asthmatic patients presenting in the emergency department with acute asthma. Urinary LTE4 levels were significantly increased in 16 patients whose peak flow increased after β agonists and tended to be increased in 12 patients who did not respond to β agonists.19 Oosaki and colleagues observed increased urinary LTE4 levels in both atopic and non-atopic asthmatics admitted to emergency departments with an acute asthma attack, suggesting that leukotrienes are important in the pathology of both types of asthma. In addition, they noted that LTE4 levels fell during recovery independent of steroid use.20 Children treated for acute asthma also have increased urinary levels of LTE4 and LTB4 compared with children without asthma.27 Urinary LTE4 levels have also been shown to be increased after antigen challenge in susceptible individuals.28
Taken together, these data strongly support the notion that cysteinyl leukotrienes (CysLT) play a significant role in acute asthma, as has been previously shown in chronic asthma.5 Inflammatory cells increase in the airways of asthmatic individuals and studies have shown that these cells appear to have large pools of the CysLT precursor, arachidonic acid.29 In addition, eosinophils from asthmatics have enhanced activity of a key CysLT enzyme, LTC4 synthase.30 LTE4 is the extracellular metabolite of LTC4, the first active metabolite in the arachidonic acid/CysLT cascade and the only one synthesised and secreted by inflammatory cells, principally mast cells, basophils and eosinophils. Although it is possible that extrapulmonary production of CysLT could account for some of the increase in urinary LTE4 excretion, the correlation of urinary LTE4 excretion and pulmonary function observed in the current study, the demonstrated efficacy of a CysLT receptor antagonist in acute asthma21 and the previous data supporting the role of CysLT in chronic asthma make this possibility highly unlikely.
Two potential limitations of the current study deserve comment. Firstly, the clinical trial on which these analyses are based was designed primarily to determine whether a CysLT antagonist could be efficacious in patients with acute asthma. For this purpose, patients were enrolled whose response to treatment with β agonists was inadequate as determined by failure to achieve a strong improvement in post bronchodilator FEV1 or an FEV1 that was less than the commonly accepted threshold (70% of the predicted value). Patients with mild or easily reversible exacerbations were therefore excluded. In addition, the most severely ill patients (that is, those who required admission to hospital) were not evaluated in the follow up period and were thus excluded from the current analyses. Nevertheless, the study population would appear to be representative of moderate to severe acute asthma in adults.21
The second limitation of the study is that patients were given standard treatment which included oxygen, β agonists and, at the investigator’s discretion, systemic corticosteroids consistent with current treatment guidelines.25,31 In fact, most (~80%) patients in the study received corticosteroids as part of treatment in the emergency department, and all patients were discharged with a standard 5 day course of oral prednisone. Nevertheless, a confounding effect of corticosteroid treatment on LTE4 levels cannot be excluded by the current data. In previous studies urinary levels of LTE4 were not altered by continued treatment with inhaled corticosteroids in children with moderate to severe asthma,8 or by treatment with corticosteroids in the emergency department in patients with acute asthma.20
In conclusion, activation of leukotriene pathways in acute asthma is correlated with the degree of airflow obstruction, and resolution of the asthma exacerbation is associated with a reduction in leukotriene levels. The consistency of these data with those determined in patients with chronic asthma8,9 support the common pathophysiology of acute and chronic asthma and substantiate the important role of leukotrienes as key mediators in the clinical spectrum of asthma.
Acknowledgments
The authors thank Dr Rene Verbesselt for performing the LTE4 analyses and Michelle Zakson-Aiken for editorial assistance. The following investigators also participated in this study: L Altman, Seattle, WA; B Brenner, Brooklyn, NY; T Burke, Olympia, WA; C Camargo Jr, Boston, MA; P Chervinsky, North Dartmouth, MA; R Cydulka, Cleveland, OH; L Graff, New Britain, CT; E Kerwin, Medford, OR; R F Lockey, Tampa, FL; R M Nowak, Detroit, MI; B O’Neil, Detroit, MI; J J Oppenheimer, Springfield, NJ; C Pollack, Phoenix, AZ; W W Storms, Colorado Springs, CO; C Terregino, Camden, NJ.
REFERENCES
Footnotes
-
This study was funded by Merck & Co, Inc.
-
Drs Green, Malice, Tanaka, Tozzi, and Reiss are employees of Merck.
Presented in part at the Society of Academic Emergency Medicine Conference, Atlanta, GA (May 2001) and the American Thoracic Society International Conference (San Francisco, CA, May 2001 and Atlanta, May 2002).