Article Text

Abstract
Background: A recent prospective study of children with asthma employing a within subject, over time analysis using dynamic logistic regression showed that severely negative life events significantly increased the risk of an acute exacerbation during the subsequent 6 week period. The timing of the maximum risk depended on the degree of chronic psychosocial stress also present. A hierarchical Cox regression analysis was undertaken to examine whether there were any immediate effects of negative life events in children without a background of high chronic stress.
Methods: Sixty children with verified chronic asthma were followed prospectively for 18 months with continuous monitoring of asthma by daily symptom diaries and peak flow measurements, accompanied by repeated interview assessments of life events. The key outcome measures were asthma exacerbations and severely negative life events.
Results: An immediate effect evident within the first 2 days following a severely negative life event increased the risk of a new asthma attack by a factor of 4.69 (p = 0.00). In the period 3–10 days after a severe event there was no increased risk of an asthma attack (p = 0.5). In addition to the immediate effect, an increased risk of 1.81 was found 5–7 weeks after a severe event (p = 0.002). This is consistent with earlier findings. There was a statistically significant variation due to unobserved factors in the incidence of asthma attacks between the children.
Conclusion: The use of statistical methods capable of investigating short time lags showed that stressful life events significantly increase the risk of a new asthma attack immediately after the event; a more delayed increase in risk was also evident 5–7 weeks later.
- asthma
- children
- stress
- Cox’s hierarchical regression
Statistics from Altmetric.com
While the role of stress in the pathogenesis of childhood asthma still remains controversial, a growing body of research suggests that psychosocial stress is likely to be a factor contributing to the development of wheezing illnesses and asthma, especially during early childhood.1–3 High levels of psychosocial stress have also been shown to predict greater morbidity in children who already have asthma,4–6 and to correlate with poorer quality of life.7
Three recent studies,8,9,10 one with children and two with adults, point to a time related association between exposure to stress and acute worsening of asthma symptoms among people who already have the disease.
A study involving college students8 with allergic asthma showed that, when challenged with antigen exposure at the time of stressful final examinations, a significant increase in eosinophilic airway inflammation was accompanied by a significant fall in forced expiratory volume in 1 second (FEV1) 24 hours after the challenge. A second study examined the effect of experimentally induced stress under laboratory conditions in adults with asthma.9 There was a rapid and significant increase in respiratory symptoms and an increase in respiratory resistance immediately following exposure to stressful stimuli eliciting negative emotions.
The only study to examine the temporal relationship between major stress experiences and asthma in a prospective design involved children with asthma and showed that stressful life events increased the risk of a new asthma attack in the coming few weeks.10 The magnitude and timing of the maximum risk was determined by the presence or absence of chronic psychosocial stress. On their own, severely negative life events significantly increased the risk of an acute exacerbation over the subsequent 3–6 week period. If, in addition, the child was living under conditions of high chronic stress, the risk was further increased and brought forward in time. This study used a dynamic logistic regression analysis with time dependent blocks of 2 weeks. Although this analysis confirmed that there were time dependent effects of stress, because of the statistical approach used it was not possible to detect any more immediate effects of the stressful life events.
There also exist two earlier experimental studies involving children.11,12 In both of these stressful emotions were deliberately induced (asking the child to recall and describe most frightening and most anger provoking memory in the former, and by a stress inducing academic task in the latter). Both studies showed a significant decrease in FEV1 under conditions of emotional arousal verified by an increase in heart rate.
More recently, animal studies have shown that exogenous stress can affect airway function13 or airway inflammation in mice,14 and have started to dissect out the pathophysiological mechanisms that led to the changes observed. An important conclusion from this evidence is therefore that stress can cause a relatively rapid decrease in airway function.
A key feature of asthma is the fact that it is episodic. It is feasible to view consecutive asthma exacerbations as serial events resembling a repeated phenomenon. This, in turn, can be modelled statistically by survival analysis techniques. In the case of an individual subject, the time periods between individual asthma attacks can be assumed to be nearly independent of one another and to follow a distribution specific to the particular child. Methods of survival analysis can then be used to examine the effects of the factors (covariates) influencing the length of the intervening time periods. Survival analysis techniques may therefore provide more appropriate statistical approaches to investigating the immediate effects of stress on function or disease physiology.
In the present study we have used a survival analysis approach (hierarchical Cox regression), using data previously collected in a prospective study of children with asthma,10 specifically to examine whether any immediate effect of stressful life events could be identified in children with asthma. We have focused on the impact of negative life events in children who were not living under conditions of high chronic stress. Of the 20 children with high chronic stress included in the previous analysis, only 12 would have been eligible for the present study—a number too small for meaningful comparisons.
METHODS
Design of study
The study was carried out as a prospective follow up over a period of 18 months. Separate teams, who were unaware of the other team’s results throughout the study, independently assessed the asthma and life events.
Subjects
Of the total of 70 children without high chronic stress aged 6–13 years (mean 8.5) originally taking part in the study, 60 were included in the analyses. Ten were excluded either because they had no or only one asthma attack in the study period (n = 8), while two children had two attacks but substantial periods of missing data. These 10 children also by chance had very few life events.
The sample selection procedure and the assessment methods have been fully described previously,10,15 so only a brief synopsis is included here. The children were regular attendees at a specialist asthma clinic at the Royal Hospital for Sick Children in Glasgow, Scotland from which recruitment took place, with the child’s age being the only selection criterion. The male/female ratio was 52%/48%, with 62% being children of parents in professional/managerial occupations, 32% in skilled occupations, and 6% in semiskilled/unskilled (including those on state benefits) occupations.16 The parental smoking ratio was 45%/55% non-smokers/smokers.
Severity of asthma
All the children had suffered from periodic asthma for a minimum of 3 years and from continuing medically diagnosed asthma in the year preceding the start of the study. All were taking prophylactic therapy with inhaled corticosteroids, together with intermittently or regularly administered bronchodilatators. The severity of asthma, rated on a 6-point scale from 1 to 5b (based on the management steps defined by the British Thoracic Society17) according to prescribed medication over the previous year, was scored as 3 (mild to moderate) in 24 cases, 4 (moderate to severe) in 20, and 5 (severe; collapsing original categories 5a and 5b because of small numbers) in 16 patients.
Measurement of life events
The Psychosocial Assessment of Childhood Experiences (PACE),15,18 a standardised investigator based interview of proven reliability and validity, was used in every case to assess the timing of occurrence, nature and impact of discrete life events. There were no missing data on any aspect of the PACE assessments.
The PACE interview is conducted independently with the child and his/her main caregiver (the mother in all but one instance) using two parallel versions, one for children and one for parents. The following areas of the child’s life are systematically covered: moves, changes in the household (births, people leaving/entering), separations from family, illnesses and hospital contacts, parents’ work, family relationships, school, major traumatic incidents, and especially good happenings. The principal criteria for accepting something as a life event are that most children of the subject’s age would find the incident either (a) threatening, upsetting, or unsettling, or (b) very pleasant, enhancing self-esteem or opening up new opportunities.
The information gathering and retrieval process took place in three stages:
Stage 1: As is usually the case with semi-structured interviewing, it is the job of the interviewer to decide when the incidents and experiences reported by the child or parent meet the requirements for inclusion as a “life event” or “long term experience”. The criteria for defining life events and long term experiences are clearly set out in a manual, together with operational guidelines. Further information is elicited about the circumstances and details of the life event including the timing of its occurrence. A great deal of care and skill is required in helping the younger children, in particular, to achieve this. Specific techniques of using certain ”anchor points” such as Christmas, family birthdays, or school starting dates are used to help the individual child to “order” and “time” their personal life experience material.
Stage 2: A synopsis of the child’s circumstances is then presented to a trained colleague (panel) referring to an extensive dictionary of examples and, following discussion, contextual ratings are made for the degree of negative and positive (not used in this study) impact each event is judged to have had on the child. The impact on the day the event occurred and 10 days later is rated for “short term” and “long term” threat, respectively. The weighted kappas range from 0.87 to 0.93.18
Stage 3: After the parent and child interviews have been separately processed and rated, a consensus meeting is held to combine them into a composite “best estimate” assessment of occurrence, timing, and impact (contextual threat). In the case of younger children, in particular, the timing is usually based on parent report.
Contextual threat refers to the level of threat caused or implied by the event to the child in question. Thus, contextual threat is simultaneously an objective and personalised measure. The existing evidence suggests that most of the risk associated with life events stems from their negative aspects. For this reason, the present study confined itself to severely negative life events (those carrying a high long term threat).
Measurement of chronic stress (long term experiences)
The existence of a wide range of chronic life experiences was also determined—for example, prolonged separation, illness (the child’s asthma excluded in the present study), and family breakdowns. Any such ongoing situations are rated for their type, timing, and objective impact. Of the individual types of negative long term experience, those to do with parenting difficulties, child’s friendship difficulties, or being socially isolated, and the parents’ marital problems are most often (4 out of 5 instances) regarded as having a high negative impact on the child. The majority of these (up to 80%) last at least a year.15 The present analyses were based on children with low to moderate chronic stress (up to three highly negative long term experiences).
Monitoring of asthma
The children, often with the help of a parent, continuously monitored the course of their asthma by completing twice daily peak flow recordings and daily diaries reporting symptoms with planned clinic review every 3 months. Acute asthma exacerbation was defined as a documented fall in peak flow (the mean of the day’s two readings) below 70% of the child’s normal value combined with a documented increase in reported symptoms.
Missing asthma data
Of the 60 children, 45 (75%) had complete records of peak flow data between the first and the last asthma exacerbation while the remaining 15 (25%) had some gaps in their diaries. The total number of intervals between consecutive asthma attacks in the returned diary booklets was 301; 30 of these (10%) contained missing data. The total length of time with missing data per child varied from 13 to 339 days, with the individual periods with no recordings varying between 7 and 229 days. The intervals with missing peak flow recordings were excluded from the data analysis.
Statistical methods
The focus of the present analysis was on the immediate effects of severely negative life events on asthma exacerbations in children. In order to achieve this objective, a model based on the length of the time intervals between consecutive asthma attacks was adopted. It assumed that a series of successive asthma attacks in a particular child are a renewal phenomenon where, without any external intervention, the attack intervals are independent and identically distributed.19 This type of process is called a “renewal process” and is specific for each child (fig 1). The present data included observations of attack intervals for each child. It should be noted that a so called intraclass correlation exists in such data for the whole study group because the asthma level varied between the children.

Description of asthma attacks in terms of intervals.
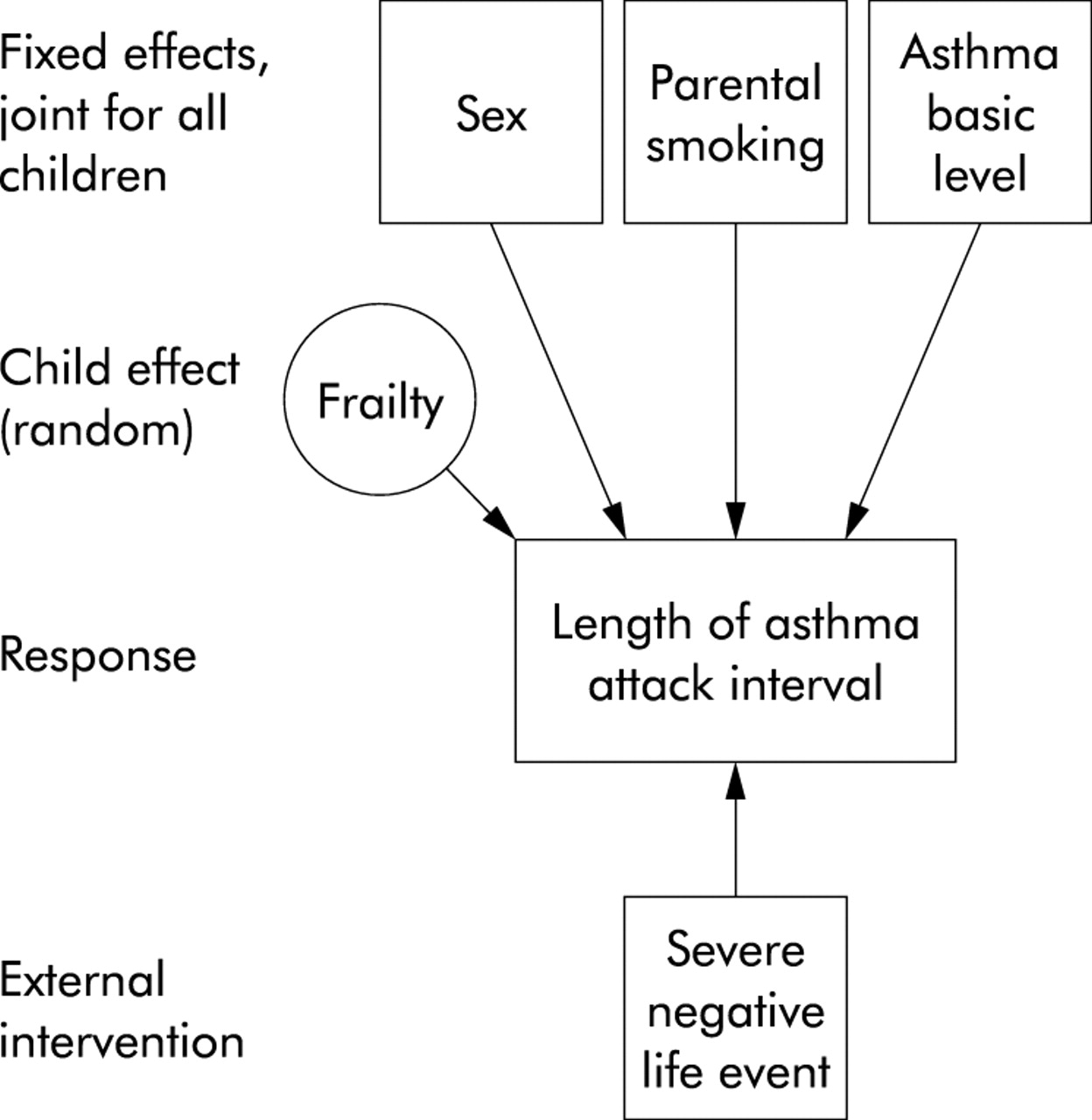
The analysis of renewal interval data under independence assumption is within the frame of survival analysis where a Cox’s proportional hazards model20 is a commonly used approach. Fixed effects such as sex, parental smoking, and baseline asthma severity (according to earlier assessment) are presumed to affect attack intervals and were used in the Cox regression as covariates. These effects are of interest as such and, in addition, reduce variation in the attack interval data. This model has the advantage of operating on a basic time unit of 1 day and hence allows better investigation of any effects of stress occurring soon after exposure.
Variation between children was modelled in the data in terms of individual level random components called frailties. These were assumed to be gamma-distributed. The role of the random component is to model the effect of unobserved factors in children such as asthma severity that potentially affect the incidence of asthma attacks. This led to a hierarchical Cox regression known as the frailty model.20
The main objective was to study more immediate effects of severely negative life events on asthma exacerbations or, in this case, on intervals between consecutive asthma attacks. This type of covariate differs from the previous ones by being time dependent. The crucial choice to be made here was to tailor the measurement to the model. Given the definition used in the interview schedule15 and the evidence highlighted above about the early effects of stress, it was assumed that a severely negative life event had a possible effect on the asthma interval for a minimum of 10 days. In order to capture any immediate effects, this interval was further divided into two consecutive intervals, 1–2 days and 3–10 days (that is, 2 and 8 days of length, corresponding approximately with the short and long term threat). This effect was additively modelled by means of two functions being indicators of the intervals 1–2 and 3–10 days and having different regression coefficients. These functions were included in the basic hazard function. We called this effect an external (time dependent) covariate. Figure 2 illustrates the hierarchical model.

The hierarchical structure of the model.
The computation was carried out using the function coxph, which can be obtained in the R-library survival.
RESULTS
Number of severe life events and acute asthma exacerbations
The mean (SD) length of observation time in the 60 children included in the study (date between the first and last recorded peak flow) was 633 (57) days (range 343–757), leaving out attacks on 18 children before or after the time range.10 These data are included in the present analysis with the time window for each child chosen to be from the first asthma attack to the last one. Altogether, 361 new asthma exacerbations occurred (mean number 6; mean duration 12.2 days), ranging from two (in seven children) to 23 (in one child). The number of severely negative life events was 124 with a mean (per child) of 2.1, ranging from 0 (in 19 children) to 9 (in one child).
Risk of new asthma exacerbations following severe events
The fixed effects included in the model were sex (boy = 0, girl = 1), parental smoking (none = 0, smoking = 1), and the baseline level of asthma for which the two lowest grades (“mild to moderate” and “moderate to severe”) were aggregated resulting in two categories of severity (0 for “not severe” (44 children) and 1 for “severe” (16 children)). Other potential covariates available in the data were socioeconomic status of the parent and season (a time dependent covariate), but the resulting subgroups (for example, four children in low socioeconomic group) were too small for analysis.
The final model included the three fixed effects and two time dependent covariates (time intervals of 1–2 and 3–10 days after a severely negative life event). These life event covariates correspond to the classification suggested by previous evidence10 and preliminary data analysis.
The estimation results corresponding to this model are shown in table 1. Sex and the baseline asthma level had a statistically significant effect. For girls the risk of an asthma attack was 1.57 times higher than for boys. Children whose asthma was classified as severe had a 1.71 times higher risk than those with less severe asthma. Risk related to parental smoking was not statistically significant although it was larger than 1 (1.13).
Estimated multiplicative changes in hazard for a new asthma attack obtained by hierarchical Cox regression
The effect of a severely negative life event was as follows. The immediate effect corresponding to 1–2 days after the event increased the risk of a new asthma exacerbation by a factor of 4.69 which was statistically significant (p = 0.00), whereas the effect for days 3–10 after the event was not statistically significant (p = 0.5). The risk of an asthma attack varied considerably between children; the frailty term was highly significant (p = 0.00).
It is of interest to compare how the results obtained by the frailty model based on the intervals between consecutive asthma attacks correspond to those10 derived from a dynamic logistic regression using a 14 day aggregation. Due to aggregation, the immediate effect observed using the present approach was not detectable. A further time dependent covariate—an indicator variable corresponding to the time interval starting 28 days (4 weeks) after the life event and lasting for 21 days (3 weeks)—was therefore added. The results of this analysis are shown in table 2.
Estimated multiplicative changes in hazard for a new asthma attack obtained by hierarchical Cox regression: the model with severe events having immediate and delayed effects
The life event increased the risk by a factor of 1.81 which is statistically significant (p = 0.002). This is in accordance with the original findings.10 Note that the immediate effect was of the same magnitude as in the first model in this analysis.
DISCUSSION
In this study we have used the technique of survival analysis (Cox’s hierarchical regression) on data previously collected in a prospective study10 specifically to examine whether any immediate impact of stressful life events could be identified in children with asthma who had no background of high chronic stress. The results were unequivocal: a rapid effect corresponding to 1–2 days after a severely negative life event was noted. In this time the risk of a new asthma attack was increased nearly fivefold. After that time the risk was substantially reduced. However, the risk almost doubled again at 5–7 weeks after the severely negative life event. A statistical technique capable of examining the time-wise association between life events and asthma exacerbations in finer detail showed a rapid increase in the risk which was obscured by previous analyses employing dynamic regression using 2 week time periods. This analysis also confirmed the more delayed effect seen in the previous analysis. Figure 3 shows that the delayed effects obtained by the Cox regression model are consistent with those obtained by the dynamic regression model.10

{kind=link}
{kind=link}
{kind=link}
Comparison of the effects in the Cox regression model and the logistic dynamic regression model.10 In the latter model the first 2 week effect containing the negative effect cannot be detected (unbroken line), no effect was observed during the second 2 week period (dotted line), and a statistically significant lagged effect was observed during the following 4 week period (broken line).
One of the differences between the two models comes from modelling dependence. In the dynamic regression this was done by regression with the outcomes in the earlier time blocks. In the Cox regression model the difference is captured by a latent factor (frailty) for each child. The corresponding results show that, in the former case, an increased risk of an attack in the past predicts an increased risk in the near future and, in the latter case, the frailty is large.
The immediate and delayed effects of stressful life events on children’s asthma exacerbations identified in this analysis are likely to be due to different underlying mechanisms.21 Previous research, however, offers only limited and somewhat inconsistent guidance for explaining the likely mechanisms. One reason for the seemingly contradictory findings and ensuing conclusions relates to the fact that the effects of stress have frequently been equated with those of emotional arousal.22 Although the two are often connected, they are far from equivalent.21 Only a few studies in children (or in adults) with asthma have so far examined the rapid effects of stress under experimental or laboratory conditions8,9,11,12,23 and, of these, all but one8 were probably measuring the effects of emotional arousal. Only animal studies13 have so far measured mediators of stress induced pathways such as neurohormones, neuropeptides, or markers of airway inflammation.
Complex neural mechanisms and alterations of the autonomic nervous system control the pathophysiology and symptomatology of asthma,6,24 with autonomic nerves impacting on airway calibre and function via effects on smooth muscle, bronchial vessels, and mucous glands. Hormones and neuropeptides released into the circulation when individuals experience stress are assumed to regulate inflammatory and airway responses. Conversely, many of the same autonomic mechanisms thought to have a role in asthma are involved in the activation and regulation of physiological responses to stress. In recent times the pivotal role of cytokines in coordinating the events of airway inflammation has been highlighted.25
Clinical and experimental studies suggest that stress and states of emotional arousal produce increases in airway resistance and can thus act as potential precursors of asthmatic symptoms.24,26 Most of the research has focused on negative emotional states such as anger, sadness and depression, linking these to symptom aggravation.11,12,22–24 It has also been suggested that increases in airway resistance are more readily explainable when stressful situations are unavoidable or inescapable, and therefore demand a passive coping response.27 A non-reciprocal pattern of autonomic functioning has been put forward as the underlying physiological mechanism.9 This is because, in some stressful situations, both vagally mediated bronchial constriction and extrabronchial sympathetic activity appear to increase in parallel. The relative strength of sympathetic versus parasympathetic control in response to certain forms of stress differs among individuals, with some showing a predominantly parasympathetic response. Such individuals may be particularly susceptible to stress induced bronchoconstriction.6,26
Sympathetic activation itself might also contribute to asthma symptoms. It is, for example, known that increases in circulating levels of adrenaline and noradrenaline alter immune parameters causing the airways to become more susceptible to inflammation. The results of a recent experimental study8 appear to support this.
The more delayed effects of stress are perhaps more difficult to explain at present. It may be that, in the presence of chronic/repeated stress, the physiological response to acute stressors results in more sustained effects on the immune system, even following sympathetic recovery. Stress induced alterations in the immune response implicated in asthma25 could therefore explain the delayed effect seen in the present study.
Lower cortisol levels found in children with asthma28 may also be responsible for the lack of suppression of airway inflammation. It is possible that children with asthma experiencing high levels of repeated stress have lower cortisol levels and/or flatter cortisol rhythms indicating a less active HPA system to control inflammation processes related to asthma.25 This could serve as a further explanation for the delayed effect of stressful life events on asthma attacks found in this sample.
Forsythe et al14 have recently found both short and long term effects in experimental studies of differing durations of stress in mice. Repeated exposure to stress over the long term engaged different mechanisms than short term stress. In the short term, the anti-inflammatory effects of corticosterone were apparent leading to a decrease in inflammatory cells in lavage fluid. In the longer term, cell influx was exacerbated, an effect that did not appear to be mediated by the effects of corticosterone. Our present analysis may be the first evidence that similar short and long term effects can be observed in humans.
This report highlights a number of points that will be important for future clinical studies of the relationship between stress and asthma. Firstly, there is a need for prospective studies of sufficient size and duration to allow more detailed investigation of both the short term effects of stress on asthma and airway function, evident within days, and the longer term effects evident weeks to months later. Such studies should be analysed using statistical techniques that can allow detailed investigation of the time course of measured outcomes. Future studies will also need to distinguish between stimuli or events that cause stress and those more likely to be temporarily increasing physiological arousal, and to consider factors such as duration of the stress and levels of chronic adversity.
Acknowledgments
The authors thank the children and their parents for their generous cooperation in the study, Dr Clive R Hillary for his valuable contribution during the data gathering stage, and Mr David McGuinness for his statistical expertise throughout the study.
REFERENCES
Supplementary materials
Publisher Correction
Please note that some of the statistics have been incorrectly presented.
In the Results section of the abstract on page 1046, the first sentence should read:
"An immediate effect evident within the first 2 days following a severely negative life event increased the risk of a new asthma attack by a factor of 4.69, 95% confidence interval 2.33 to 9.44 (p <_0.001. p="p"> The third sentence should read:
"In addition to the immediate effect, an increased risk of 1.81 (95% confidence interval 1.24 to 2.65) was found 5�7 weeks after a severe event (p=0.002)".On page 1049 the third paragraph should read:
"The effect of a severely negative life event was as follows. The immediate effect corresponding to 1�2 days after the event increased the risk of a new asthma exacerbation by a factor of 4.69 (95% confidence interval 2.33 to 9.44) which was statistically significant (p <_0.001 whereas="whereas" the="the" effect="effect" for="for" days="days" _310="_310" after="after" event="event" was="was" not="not" statistically="statistically" significant="significant" p="p" risk="risk" of="of" an="an" asthma="asthma" attack="attack" varied="varied" considerably="considerably" between="between" children="children" frailty="frailty" term="term" highly="highly" p0.001.="p0.001."> The errors are much regretted.
Footnotes
-
This study was supported by the Medical Research Council, UK (grant G9102413N), the Academy of Finland (grant 41224), and Laboratory of Data Analysis, Center for Mathematical and Computational Modelling, University of Jyväskylä, Finland.