Article Text

Abstract
Background:Stenotrophomonas maltophilia (SM) is a Gram-negative non-fermenting bacteria cultured from the sputum of patients with cystic fibrosis (CF). To date, no information is available regarding the effect of this organism on lung function in CF.
Methods: A cohort study was conducted to assess the effect of SM on lung function among CF patients aged ⩾6 years in the CF Foundation National Patient Registry from 1994 to 1999. Repeated measures regression was used to assess the association between SM and lung function.
Results: The cohort consisted of 20 755 patients with median age at entry of 13.8 years and median follow up time of 3.8 years; 2739 patients (13%) were positive at least once for SM and 18 016 (87%) were never positive. After adjusting for sex, height and age, patients with SM had a mean forced expiratory volume in 1 second which was 0.09 l less (95% CI 0.05 to 0.14) than those without SM. The mean rate of decline associated with SM positivity was 0.025 l/year (95% CI 0.012 to 0.037) but, after adjusting for confounders (sex, height, weight, intravenous antibiotic courses, hospital admissions, pancreatic insufficiency, and Pseudomonas aeruginosa and Burkholderia cepacia status), the mean rate of decline decreased to 0.008 l/year (−0.008, 95% CI −0.019 to 0.003).
Conclusions: Although CF patients with SM have worse lung function at the time of positivity, no association was found between SM and increased rate of decline after controlling for confounders.
- Stenotrophomonas maltophilia
- cystic fibrosis
- lung function
- outcome
Statistics from Altmetric.com
Cystic fibrosis (CF) is one of the most common inherited fatal diseases in white ethnic groups with a reported incidence ranging from 1 in 2000 to 1 in 3200 live births.1 With improved survival, physicians caring for these patients have witnessed the emergence of new pathogens in the CF lung including Burkholderia cepacia, Stenotrophomonas maltophilia, Achromobacter xylosoxidans, and Mycobacterium avium complex.2–4Stenotrophomonas maltophilia (previously Pseudomonas or Xanthomonas maltophilia) is a non-fermenting Gram-negative rod and one of the more prominent emerging pathogens in the CF airway with significant resistance to broad spectrum antibiotics, resulting in only limited treatment options. S maltophilia has been isolated from a wide range of nosocomial sources including nebulisers and oxygen humidifier reservoirs.5
The importance of S maltophilia colonisation in CF patients is still unclear. Three small single centre case-control studies have been performed which found no definitive evidence that S maltophilia is associated with a worse prognosis.6–8 A cohort study previously performed by our group using the CF Foundation National Patient Registry (CFF NPR) revealed that detection of S maltophilia was not associated with worse short term (3 year) survival.9 While the results of this study support the results from previous studies, evidence is still limited with regard to the effect of S maltophilia on morbidity in CF patients, as assessed by surrogate markers such as decline in lung function. For this reason, we analysed data from the CFF NPR to investigate the effect of the organism on lung function.
METHODS
Study subjects
The CFF NPR contains data collected annually from participants at US CFF accredited centres.10 We studied all patients in the NPR between January 1994 and December 1999 who were ⩾6 years of age and had at least one pulmonary function measure by the end of the observation period. Patients under 6 years of age do not routinely have spirometry data in the NPR. The study was approved by the CFF and Institutional Review Board at the University of Washington, Seattle, WA.
Study design
The design was a cohort study. Lung function was the primary outcome, as measured by forced expiratory volume in 1 second (FEV1) at most quarterly for each patient during each year of observation. Colonisation with S maltophilia was recorded for each year of observation. Potential confounders of the relationship between S maltophilia and lung function were also obtained over the observation period (weight, height, use of pancreatic enzymes, number of CF related hospital admissions, number of courses of home intravenous antibiotics, and presence of Pseudomonas aeruginosa and Burkholderia cepacia).
Statistical analysis
Annual incidence and prevalence rates were computed. The incidence of newly diagnosed S maltophilia cases was calculated for each year as the number of patients with their first detection of S maltophilia divided by the total number of patients at risk for first detection of S maltophilia in that year. The annual prevalence of S maltophilia was calculated as the total number of cases of S maltophilia each year divided by the total number of patients during that year. An overall S maltophilia “case rate” was calculated for each centre as the total number of cases of S maltophilia at that centre during the observation period divided by the total number of patients at that centre during the observation period.
Repeated measures linear regression11 models were used to assess the effect of S maltophilia on FEV1 over time, with adjustment for potential confounders. Each patient contributed a maximum of four measurements each year of observation and the effect of time was captured in the model using age in years. Thus, in these models the effect of S maltophilia on lung function is interpreted as the average effect across age. Clinically relevant interactions were decided before assessment in the model. To ensure parsimonious models, only bacteria found to be significantly associated with clinical outcome in earlier models and the literature were assessed; thus, Staphylococcus aureus and Haemophilus influenzae culture status were not included in the current models. To assess the effect of first detection of S maltophilia during the study period on subsequent decline in lung function, the time since first detection of S maltophilia was included in the model and used to estimate rate of decline in FEV1. Time from first detection was zero when patients were negative for S maltophilia since the beginning of the observation period. For patients positive for S maltophilia during the observation period, time was calculated as number of years since first positive culture. To investigate the sensitivity of the results of the model to potential differences in detection of S maltophilia rates across centres, the final models were applied to subsets of the cohort who came from centres with different case rates and total number of S maltophilia cases. Observations with missing data were excluded from the analysis.
Analyses were performed with SAS 8.2 (SAS Institute Inc, Cary, NC) and Splus 6.1 (Insightful Corp, Seattle, WA). Overlapping research from our group is reported elsewhere.9
RESULTS
S maltophilia cohort characteristics
A total of 20 755 patients aged 6 years and over were included in the cohort from all 176 CFF accredited centres (including pediatric CF centres, adult CF centres, and CF centres comprised of both a pediatric and adult centre). The mean (SD) age at entry into the cohort was 16.1 (10.3) years (median 13.8 years), with a median follow up time of 3.8 years. 2739 patients (13%) were positive for S maltophilia at some point during follow up and 18 016 (87%) were never positive.
The mean (SD) age of the patients who were positive for S maltophilia during the first year in which it was detected during the study period was 18 (10.4) years. Nearly half were females and 55% were ΔF508 homozygous compared with 36% heterozygous for the ΔF508 mutation. The mean FEV1 % predicted was 66.1% and, while 35% used home intravenous antibiotics during the year they were first detected with S maltophilia in the registry, 57% were hospitalised at least once. 63% of the patients were concurrently infected with P aeruginosa and only 5% with B cepacia.
S maltophilia detection rates
There was only a slight increase in the incidence rate of first detected S maltophilia cases in the cohort over time, with the lowest incident rate of 2.7% in 1995 and the highest rate of 4.2% in 1999. The annual prevalence rate during each year of observation ranged from 3.2% in 1994 to 6.9% in 1999 (fig 1). The mean case rate of S maltophilia infection was 12.3% across the 176 centres, ranging from seven centres with no S maltophilia cases to one centre with a maximum rate of 38.6% (fig 2). There was no distinct association between the S maltophilia case rate and centre size (see fig S1 on the Thorax website at www.thoraxjnl.com/supplemental). The distribution of the S maltophilia incidence and prevalence rates did not differ significantly by geographical region (p values 0.06 and 0.07, respectively; see fig S2 on the Thorax website at www.thoraxjnl.com/supplemental).

Incidence and prevalence of newly diagnosed S maltophilia cases during each year of observation in the cohort. Annual incidence (%) of new cases: number of new cases/number at risk. Annual prevalence (%) of current cases: number of cases/number at risk.

Distribution of S maltophilia case rates among the 176 centres.
Association between S maltophilia and lung function
S maltophilia was shown to be significantly negatively correlated with FEV1 (model 1, table 1). Patients with S maltophilia had a mean FEV1 0.140 l (95% CI 0.112 to 0.167) less than patients without S maltophilia after adjusting for physiological confounders including sex, height, and age. The mean FEV1 was 0.111 l less in females than in males (95% CI 0.090 to 0.132) and increased 0.034 l for every centimetre increase in height (95% CI 0.032 to 0.035). Age was independently associated with decreased lung function as measured by mean FEV1 after adjusting for height and sex; each increase in age of 1 year was associated with a decrease in FEV1 of 0.036 l (95% CI 0.033 to 0.039). There were no significant interactions between S maltophilia positivity and age, height, or sex. Thus, the association observed between FEV1 and S maltophilia was similar across the different ages included in the cohort.
Model 1 investigating the association between S maltophilia and FEV1 (in litres) after adjusting for physiological confounders
Effect of S maltophilia on lung function decline
To investigate the effect of S maltophilia on lung function decline after adjusting for age, sex, and height, time from first detection of S maltophilia during the study period was included in model 2 (table 2). The mean rate of decline after first detection of S maltophilia was 0.025 l (95% CI 0.012 to 0.037), indicating that S maltophilia has a modest impact on the decline in lung function without taking potential clinical confounders into account.
Model 2 investigating the association between time from first detection of S maltophilia during the observation period and FEV1 (in litres) after adjusting for physiological confounders
Effect of S maltophilia on lung function after adjusting for clinical confounders
Since the effect of S maltophilia on lung function and its decline may be confounded by important clinical variables, further modelling was done to include additional clinical characteristics (model 3, table 3). Genotype and pancreatic insufficiency were not found to be significantly related to FEV1 in this model. For each kilogram increase in weight, FEV1 increased by 0.036 l (95% CI 0.034 to 0.038). FEV1 was significantly worse in patients who received intravenous antibiotics and/or were hospitalised. Patients who used two or more home intravenous antibiotic courses had a mean FEV1 0.235 l less than patients who did not use antibiotics (95% CI 0.211 to 0.256), and in patients with two or more hospital admissions the mean FEV1 was 0.387 l less than patients not admitted to hospital (95% CI 0.367 to 0.407). P aeruginosa and B cepacia were shown to have a similar effect on FEV1. Patients infected with these organisms had a mean FEV1 that was 0.149 l (95% CI 0.135 to 0.163) and 0.142 l (95% CI 0.103 to 0.181) less, respectively, than patients without these organisms. These two organisms contrast with the relatively mild impact of S maltophilia on FEV1 of −0.035 l (95% CI −0.056 to −0.014). The time from first detection of S maltophilia was no longer significant in this model (−0.008 l, 95% CI −0.019 to 0.003).
Model 3 investigating the association between time from first detection of S maltophilia during the observation period and FEV1 (in litres) after adjusting for both physiological and clinical confounders
Impact of repeated S maltophilia detection
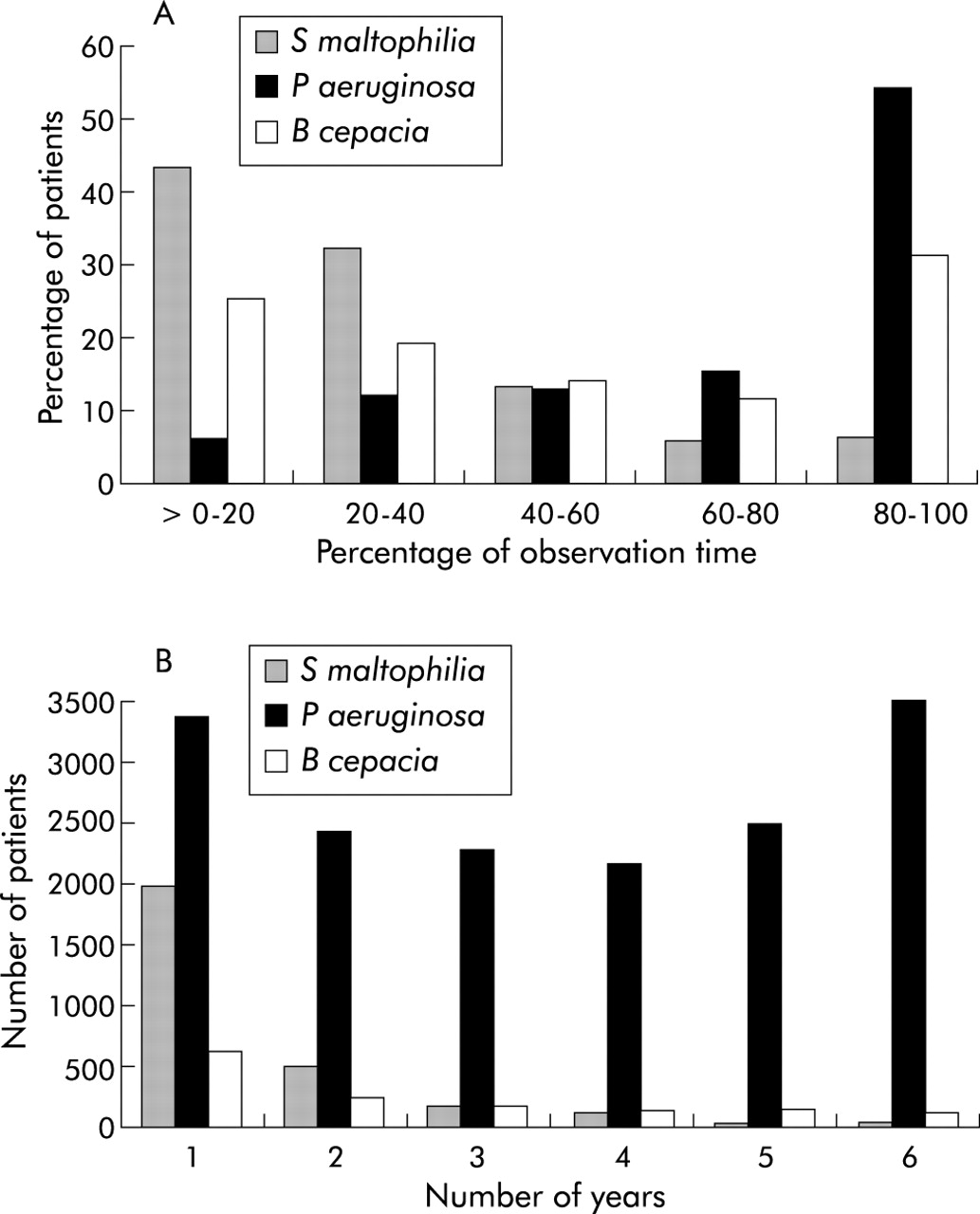
Compared with P aeruginosa, repeated positivity for S maltophilia was not a common event (fig 3). Only 29% of the 2739 S maltophilia positive patients had S maltophilia detected for 2 years or more (not necessarily consecutive) during the observation period. In addition, only 11% of the S maltophilia positive patients had S maltophilia detected for more than 2 years, in contrast to data suggesting that over 80% of P aeruginosa positive patients have persistent positive cultures for 5 years or more. To assess the impact of more than 1 year of S maltophilia detection, the effect on the decline in lung function after the second year of positivity for S maltophilia was evaluated. After adjusting for height, age and sex, the mean rate of decline after the second detection of S maltophilia was 0.046 l (95% CI 0.021 to 0.071). However, after adjusting for additional confounders, the decline in lung function associated with 2 years or more of infection with S maltophilia was no longer significant.

{kind=link}
{kind=link}
{kind=link}
(A) Percentage of observation time (follow up time) during which annual culture results remain positive for patients who have been culture positive for S maltophilia, P aeruginosa, and B cepacia. (B) Number of years per patient that annual culture results are positive during the observation period (not necessarily consecutive) for S maltophilia, P aeruginosa, and B cepacia.
Sensitivity of models to S maltophilia detection rates
To investigate the sensitivity of the models to potential S maltophilia detection differences between centres, the analyses were repeated in a subset of centres that had a minimum S maltophilia case rate of 10% and at least 10 S maltophilia cases (representing 60% of the 20 755 patients in the cohort, 77% of the 2739 S maltophilia cases, and 43% of the 176 centres). Similar results were obtained from these analyses when compared with the entire cohort, with comparable effect sizes and significance of the coefficients. In particular, the time to first detection of S maltophilia remained non-significant. Further analyses were performed using subsets of data with different cut off values for the S maltophilia case rate and count and similar results were obtained, affirming the robustness of these findings.
DISCUSSION
S maltophilia continues to be a relatively common organism cultured from the sputum of patients with CF. Patients with S maltophilia are older, have mild to moderate decreases in lung function, and are commonly co-infected with P aeruginosa, as noted in earlier work.9 Annual incidence rates of S maltophilia detected and reported in the CFF NPR did not change appreciably during the study period, which argues against a significant detection bias during the study period or a rapidly evolving outbreak in CF patients. However, we found significant variability of rates of S maltophilia detection at different centres and by region, with an increasing prevalence rate during the study period. On average, CF patients with S maltophilia had mildly decreased lung function after adjusting for age, sex, and height, and also had a mild increase in the rate of decline in lung function. The rate of lung function decline increased from 0.025 to 0.046 l/year after having S maltophilia detected in at least two separate or consecutive years. However, after adjusting for important confounders (age, sex, weight, height, pancreatic insufficiency, P aeruginosa and B cepacia colonisation, use of intravenous antibiotics), S maltophilia no longer had a significant effect on lung function decline. These findings were similar when only large centres with high case rates were analysed. The lack of evidence for a decline in lung function after adjusting for important confounders supports the contention that S maltophilia is not associated with a worse short term clinical outcome.9
In CF populations the prevalence rates of S maltophilia have varied depending on the population studied but, overall, the prevalence appears to have increased over the last 15 years.12–14 In one of the most comprehensive studies using microbiology of sputum samples from a study of aerosolised tobramycin in 595 patients at 69 CF centres in 1995–6, the prevalence of S maltophilia was 10.3%.14 We now present data which support a relatively stable incidence rate from 1994 to 1999, despite fairly wide variation between centres. We cannot delineate whether this is due to differences in culturing frequency or culturing techniques. A report by Shreve and colleagues noted that, by 1995, the majority of sites in the US followed the CFF consensus conference recommendations for quarterly cultures published in 1994, with all but two of 142 responding laboratories reporting growth of organisms like S maltophilia and Achromobacter xylosoxidans.15,16 The relatively constant annual incidence rate seen in the current study argues against a sudden increase in detection or culturing techniques. Persistent S maltophilia infection (defined as three or more positive cultures in a 12 month period) is not a common event;8,17 Demko and colleagues found persistent S maltophilia colonisation in only 11% of their cohort.8 Episodic infection with S maltophilia (defined as only one positive culture out of a minimum of three cultures) has clearly been identified in the literature and was noted to be very common (50%).8 Because the patients included in our study were denoted as positive if one or more cultures were positive during the year, one must be cautious in interpreting our results in comparison with other reports whose definitions have relied on the number of positive cultures over a discrete time period. We found that S maltophilia infection and detection (when based on positivity over a period of 1 year) is not a common event, with most patients in our cohort noted to be positive in only 1 year of the 6 year study period. In our population, only 29% of patients were positive for more than 1 year and 11% for more than 2 years. The isolation of S maltophilia in CF patients tends to be associated with more advanced disease.8,9,13,18 Characteristics associated with S maltophilia detection include lower mean weight percentile, lower Shwachman-Kulczycki score, lower FEV1 % predicted, more advanced age, oral quinolone antibiotic use, and long term antibiotic use.9,13,18,19 Despite these results, nebulised tobramycin has not been conclusively associated with an increased risk of acquiring S maltophilia.18 A significant proportion of patients in the current study had been hospitalised and received home intravenous antibiotics during the year of first detection of S maltophilia during the study period.
The clinical relevance of this increase in prevalence in S maltophilia remains unclear; however, the literature increasingly points to this pathogen acting as an intermittent coloniser of the CF airway without evidence of associated clinical decline.6,9 Neither Gladman and colleagues6 nor Karpati et al7 found evidence of a clinical decline associated with S maltophilia colonisation in their studies. S maltophilia has been associated with a statistically significant decline in lung function (the absolute change was not noted)7 and, in patients with severe pulmonary impairment, worse 2 year and possibly 5 year survival.8 Formal survival modelling using data from the CFF NPR did not, however, corroborate the latter finding.9 We have shown that S maltophilia is associated with a lower mean FEV1 (0.092 l less) than in patients without S maltophilia after adjusting for height, sex, and age. However, the impact on mean lung function was much less than the effect of detecting P aeruginosa and B cepacia in the sputum of CF patients (0.035 l v 0.149 l and 0.142 l, respectively) after adjusting for important confounders. The rate of lung function decline after first detection of S maltophilia in this cohort was significant but small (0.025 l/year) after adjusting for physiological variables. Of some concern was the fact that this effect on lung function decline increased when evaluated after the second year of reported positivity for S maltophilia (0.046 l/year). However, this effect was not seen after adjusting for other important confounders.
Important limitations of these analyses relate to the assessment of S maltophilia status. Differences in the number of sputum samples requested, the specific organisms requested, and sputum culturing techniques may have changed over time, leading to misclassification of S maltophilia status and ascertainment bias. However, the effects of S maltophilia were noted to be similar when limited to large centres with high case rates. In our analyses, patients with a single positive culture per year are treated the same as patients with multiple positive cultures per year, thus limiting our ability to assess the effect of multiple infections within a given year. We also do not have specific data regarding compliance with the 1994 CFF consensus conference on microbiological procedures, nor were we able to control for treatment of S maltophilia. However, we were able to assess the effect of being repeatedly positive for S maltophilia over different years and found no evidence of an increased rate of lung function decline. Finally, the generalisability of the results is restricted to those patients included in the CFF NPR, but the NPR captures a significant proportion of the US CF population and an estimated 95% of all deaths in CF patients in the US.10
In conclusion, we have shown that S maltophilia is associated with lower mean lung function without evidence of an increased rate of decline in lung function after adjusting for confounders. S maltophilia remains a relatively common intermittent (not persistent) infection in CF, with relatively stable annual incidence rates during the period of study. S maltophilia is a pathogen, but its role in increasing the decline in lung function in CF is minimal, as suggested in this study. Further studies are needed to address treatment patterns for S maltophilia and the impact of such treatment on clinical outcome.
Acknowledgments
The authors thank Preston Campbell III, Vice President for Medical Affairs, CF Foundation, Bruce Marshall, Director of Clinical Affairs, CF Foundation, Monica Brooks, CF Foundation, and the CF community for their support of this project and for providing the CF Registry data.
REFERENCES
Footnotes
-
Support: Leroy Matthew Physician Scientist, Cystic Fibrosis Foundation, The Firland Foundation.