Article Text

Abstract
Background: Severe α1-antitrypsin deficiency, usually related to homozygosity for the protease inhibitor (PI) Z allele, is a proven genetic risk factor for chronic obstructive pulmonary disease (COPD). The risk of COPD in PI MZ heterozygous individuals is controversial.
Methods: A search of MEDLINE from January 1966 to May 2003 identified studies that examined the risk of COPD in PI MZ individuals and studies that measured forced expiratory volume in 1 second (FEV1) in heterozygotes.
Results: In 16 studies that reported COPD as a categorical outcome, the combined odds ratio (OR) for PI MZ versus PI MM (normal genotype) was 2.31 (95% CI 1.60 to 3.35). The summary OR was higher in case-control studies (OR 2.97; 95% CI 2.08 to 4.26) than in cross sectional studies (OR 1.50; 95% CI 0.97 to 2.31) and was attenuated in studies that adjusted for cigarette smoking (OR 1.61; 95% CI 0.92 to 2.81). In seven studies that reported FEV1 as a continuous outcome there was no difference in mean FEV1 between PI MM and PI MZ individuals.
Conclusions: Case-control studies showed increased odds of COPD in PI MZ individuals, but this finding was not confirmed in cross sectional studies. Variability in study design and quality limits the interpretation. These results are consistent with a small increase in risk of COPD in all PI MZ individuals or a larger risk in a subset. Future studies that adjust for smoking and include other COPD related phenotypes are required to conclusively determine the risk of COPD in PI MZ heterozygotes.
- α1-antitrypsin
- chronic obstructive pulmonary disease
- heterozygote
- meta-analysis
- genetics
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of death in the United States and a major cause of respiratory disability.1 Exposure to cigarette smoke is a well known environmental risk factor for COPD. Severe deficiency of α1-antitrypsin (AAT) is a proven genetic risk factor, but only 1–3% of all cases of COPD are estimated to be due to severe AAT deficiency.2
AAT is a serine protease inhibitor that protects the lung from the action of proteases, primarily neutrophil elastase. It is encoded by the polymorphic protease inhibitor (PI) locus on chromosome 14q32.1. The most common alleles are the normal M allele (95% frequency in the US) and the deficient variants S (2–3%) and Z (1–2%).3 Severe AAT deficiency is most commonly due to homozygosity for the Z allele (PI ZZ). Heterozygotes for the Z allele (most commonly PI MZ) have lower serum levels of AAT than normal individuals (PI MM)4 but the risk of lung disease in PI MZ individuals remains uncertain.
Although the risk of COPD in PI MZ heterozygotes has been analysed in many previous studies, the results have been inconsistent.5–7 In general, case-control studies have found an increased prevalence of PI MZ heterozygosity in COPD patients. However, PI MZ individuals identified from population surveys have not consistently been found to have higher rates of airflow obstruction than PI MM individuals. With an estimated six million PI MZ individuals in the US and over 10 million in Europe, determination of the COPD risk in PI MZ individuals may have broad public health implications.8 We therefore performed a systematic review of the medical literature to examine the risk of COPD in AAT PI MZ heterozygotes.
METHODS
Study selection
A search of MEDLINE was performed to identify all studies that examined the risk of COPD or that measured pulmonary function in AAT PI MZ heterozygotes published between January 1966 and May 2003 using the medical subject headings “α1-antitrypsin”, “α1-antitrypsin deficiency”, “protease inhibitors”, “obstructive lung diseases”, “chronic obstructive pulmonary disease”, “pulmonary emphysema”, “forced expiratory volume”, “respiratory function tests”, and “spirometry”. Bibliographies of pertinent articles and reviews were searched for additional references.
Two investigators independently evaluated studies for inclusion (CPH, MD). Disagreements were resolved by discussion including a third author (EKS). Included studies were case-control, cohort, and cross sectional studies using the categorical outcome of COPD based on spirometry or a physician’s diagnosis. Studies reporting forced expiratory volume in 1 second (FEV1) as a continuous outcome measure were also included. In the case-control design, comparison with controls from a previously published report was permitted as long as the cases and controls were from the same country and the same method was used for determination of PI type. In all included studies, PI type had to be determined using isoelectric focusing, acid starch gel with crossed immunoelectrophoresis, or a polymerase chain reaction (PCR) based genotyping method.
Studies defining heterozygotes based on serum AAT levels or functional activity were excluded since PI MZ heterozygotes could not be consistently distinguished from other genotypes. Family studies and studies of children only were also excluded. For the continuous outcome, studies that did not present FEV1 as a percentage of the predicted value were analysed separately. We also attempted to exclude duplicate analyses of the same population of cases.
Study quality
A global assessment of the quality of each study was made, based on the following criteria: (1) Was the phenotype of obstructive lung disease defined by objective spirometric indices? (2) Were the cases and controls (in case-control studies) or the PI MZ and PI MM individuals (in population based studies) matched on ethnicity? (3) Did the studies control for cigarette smoking? (4) Did the authors test for Hardy-Weinberg equilibrium in the controls (case-control design) or in the population (cross sectional design)?
The quality of a study was not a factor in its inclusion, except when the cases and controls were derived from studies in different countries as mentioned above. The quality criteria were used for the subgroup analyses.
Data analysis
Two investigators independently extracted data from each study. When studies determined COPD both by spirometric criteria and by physician diagnosis, the spirometric definition was used. Due to the small number of longitudinal studies, only the baseline cross sectional data from cohort studies were used. The effect estimates were combined using the random effects method of DerSimonian and Laird.9 All analyses were performed using STATA release 8 (STATA Corp, College Station, TX, USA). The Q-statistic was used to assess for heterogeneity among studies.
Funnel plots and weighted regression were used to search for publication bias.10 Subgroup analyses were used to examine three potentially important sources of heterogeneity. The predetermined subgroups were based on study design, use of spirometric criteria to define COPD, and adjustment for cigarette smoking. The stability of the summary risk estimate was evaluated using a sensitivity analysis; each study was individually removed and the odds ratio (OR) was recalculated.
The studies that reported FEV1 as a continuous outcome were analysed separately. A summary difference in mean FEV1 between PI MM individuals and PI MZ individuals was calculated using the random effects model.
RESULTS
Search results and study eligibility
The initial search yielded 1125 references. From these, 106 studies were retrieved for detailed review and 22 were selected for primary analysis (tables 1 and 2).11–32 Sixteen studies were case-control or cross sectional studies with the binary outcome of COPD or airflow obstruction. Seven cross sectional studies measured FEV1 (% predicted) as a continuous outcome; four additional studies reported FEV1 in litres and were used for confirmatory analysis. One study included both the continuous and categorical outcome measures and was included in both analyses.15
Studies examining risk of COPD in α1-antitrypsin PI MZ heterozygotes
Studies reporting FEV1 (% predicted) in α1-antitrypsin PI MZ heterozygotes
The reasons for exclusion were: determination of PI type by suboptimal methods (n = 14),33–46 reviews, editorials, or conference proceedings (n = 13),5,38,47–57 absence of an adequate control group (n = 11),45,58–67 measured pulmonary function tests other than FEV1 (n = 10),68–77 analysed other PI types but not PI MZ (n = 10),56,57,78–85 recorded FEV1 as an absolute volume and not as percentage of predicted (n = 9, of which four were included in a separate analysis),86–94 did not differentiate PI MZ from other variant genotypes (n = 8),87,90,95–100 used AAT level to define the exposure or the outcome (n = 8),44,47,101–106 COPD defined by self-report or hospital discharge records (n = 3),88,107,108 duplicate studies in the same population of cases (n = 3),109–111 children only (n = 3),97,112,113 and family based study design (n = 2).114,115 Some studies were excluded for more than one reason.
Study quality
The quality criteria fulfilled by each study are shown in tables 1 and 2. Nine studies used specific spirometric criteria to define COPD;11,12,15,17,23–25,30,31 these criteria were usually based on a reduced value for the FEV1 and/or the ratio of FEV1 to forced vital capacity (FVC). The other seven studies used clinical diagnoses which may have included pulmonary function testing, but explicit criteria were not stated. By definition, spirometry was recorded in all seven studies that reported mean FEV1 as the outcome measure.
Most of the case-control studies derived their controls from local sources; only two studies used blood donors as controls. In most of the cross sectional studies the PI MM and PI MZ individuals were derived from the same source population. Four of the North American studies were restricted to Caucasian subjects11,14,26,30 and one matched cases and controls by ethnicity.17 Six studies were conducted in European nations where ethnic homogeneity is likely.13,15,18,20,24,29 Among the studies that examined FEV1 as a continuous outcome, only one of the four North American studies was restricted to Caucasians.28 Three studies measuring FEV1 as a continuous outcome were done in Europe.15,16,19 None of the included studies explicitly addressed population stratification—for example, by testing a panel of unlinked markers.116
In the categorical analysis of COPD in case-control and cross sectional studies, five studies controlled for cigarette smoking.11,15,23,25,30 Kueppers and coworkers25 matched cases and controls on smoking history categorised into non-smokers, moderate smokers, and heavy smokers based on lifetime pack-years smoked. Two studies stratified by smoking status. Klayton et al23 divided subjects into never versus ever smokers, and Chan-Yeung et al11 into non-smokers, ex-smokers, and current smokers. The study by Dahl et al15 used logistic regression modelling to control for smoking status. One additional study used logistic regression but the resulting OR was not presented;30 for our analysis, the OR was calculated by adding a correction factor of 0.5 to all cells to account for a zero cell. In the analysis of mean FEV1 as a continuous outcome, four studies controlled for cigarette smoking. Hall and colleagues21 restricted the study to non-smokers. Eriksson and coworkers16 performed a stratified analysis, presenting mean FEV1 values for smokers, ex-smokers, and non-smokers. In the studies by Girard et al19 and Horne et al22 PI MZ and PI MM individuals were matched by smoking status.
In the study by Dahl and colleagues15 a test of Hardy-Weinberg equilibrium was performed; in this population sample the observed genotype frequencies did not differ from those predicted under Hardy-Weinberg equilibrium. In no other study did the authors report testing for Hardy-Weinberg equilibrium. Based on the predetermined criteria, the majority of studies were judged to be of suboptimal quality. The study by Dahl and coworkers15 was the only one that met all four of the predefined quality criteria.
Odds ratio (OR) for COPD in PI MZ heterozygotes
Six of the 16 studies examining the categorical outcome of obstructive lung disease found significantly higher ORs for COPD in PI MZ heterozygotes than in PI MM individuals (fig 1). In nine other studies the OR was increased, but not significantly. One study found a reduced OR, but not significantly. The individual study ORs ranged from 0.15 to 16.78. Using the random effects method,9 the summary OR for COPD in PI MZ compared with PI MM individuals was significantly increased at 2.31 (95% CI 1.60 to 3.35).

Case-control and cross sectional studies of COPD in α1-antitrypsin PI MZ heterozygotes. Sizes of boxes represent inverse variance weights (random effects model).9 Lines represent 95% confidence intervals.
Significant heterogeneity was detected among the studies (Q test: χ215df = 36.1, p = 0.002). Subgroup analyses are shown in fig 2. In a subgroup analysis based on study design, the 11 case-control studies were found to have a larger summary OR than the five cross sectional categorical studies (case-control OR 2.97, 95% CI 2.08 to 4.26; cross sectional OR 1.50, 95% CI 0.97 to 2.31). There was less heterogeneity within each of these subgroups than in the combined analysis (case-control χ210df = 12.3, p = 0.27; cross sectional χ24df = 5.9, p = 0.21).

Subgroup analysis of studies of COPD in α1-antitrypsin PI MZ heterozygotes. Odds ratios with 95% confidence intervals are shown.
The magnitude of the effect estimate was similar in the nine studies that used spirometric criteria for the definition of obstructive lung disease (OR 2.17, 95% CI 1.22 to 3.87) and the seven studies that relied on clinical diagnoses of COPD (OR 2.52, 95% CI 1.65 to 3.85); heterogeneity was reduced, but still possible, within each of these subgroups as well (spirometric criteria χ28df = 15.4, p = 0.051; no spirometric criteria χ26df = 10.3, p = 0.11).117
The magnitude of the effect estimate was lower in the five studies that adjusted for cigarette smoking (OR 1.61, 95% CI 0.92 to 2.81) than in the 11 studies that did not (OR 2.73, 95% CI 1.86 to 4.01); in the studies that stratified by smoking status, data were pooled across each stratum for analysis. Again, heterogeneity was reduced within each of these subgroups (adjustment for smoking χ24df = 6.8, p = 0.15; no adjustment for smoking χ210df = 14.7, p = 0.14). Due to the different methods used to control for smoking in the different studies, separate summary ORs for smokers and non-smokers could not be derived.
In the sensitivity analysis, when the study by Dahl et al15 was removed from the analysis, the summary OR was increased above that obtained using all 16 studies. When each of the other 15 papers was removed individually, the summary OR was unchanged. The funnel plot of OR versus standard error (both log transformed) appeared to be symmetrical, and the regression method of Egger et al10 did not indicate significant evidence for publication bias (p = 0.15).
Mean FEV1 in PI MZ heterozygotes compared with normal subjects
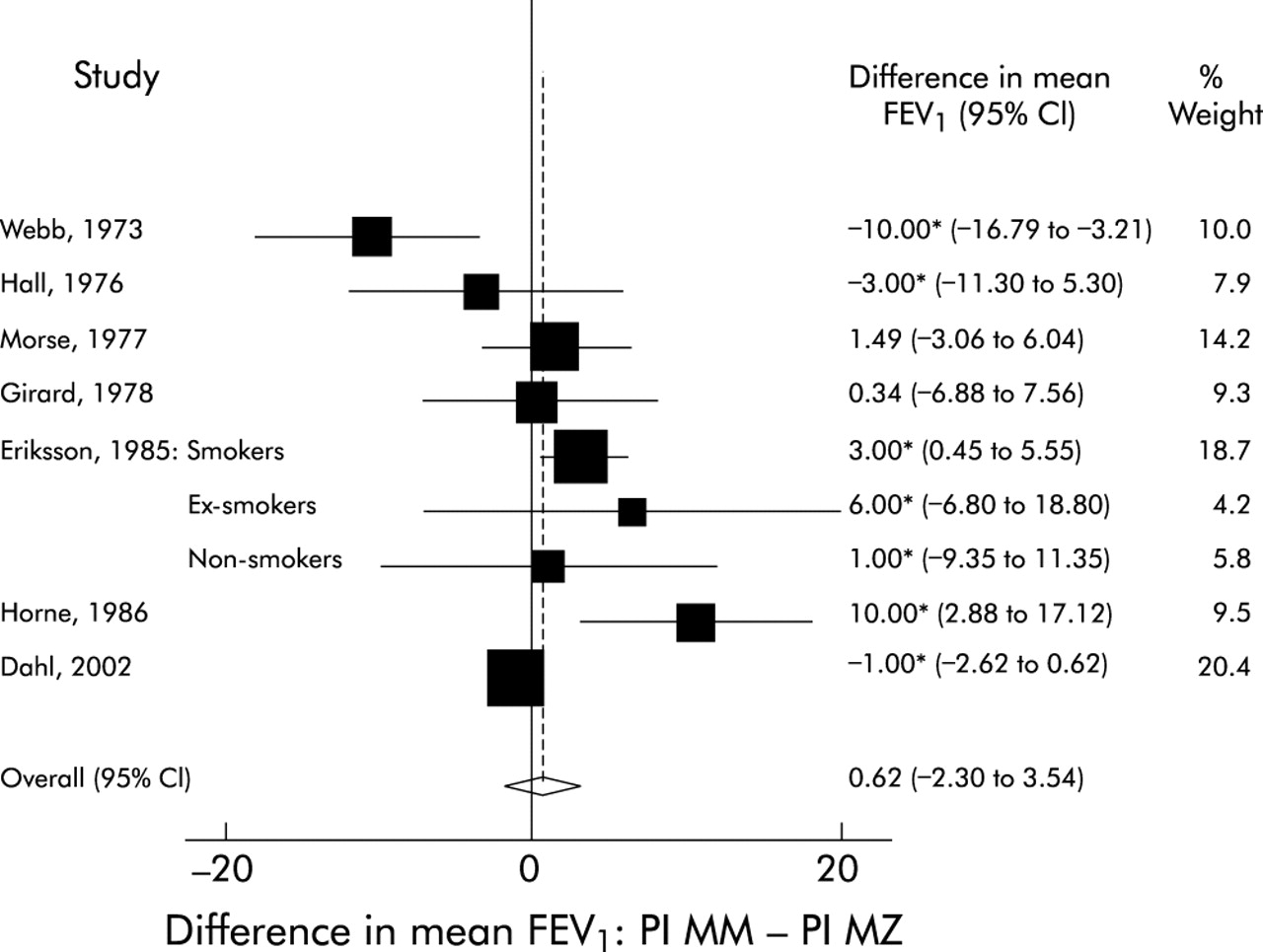
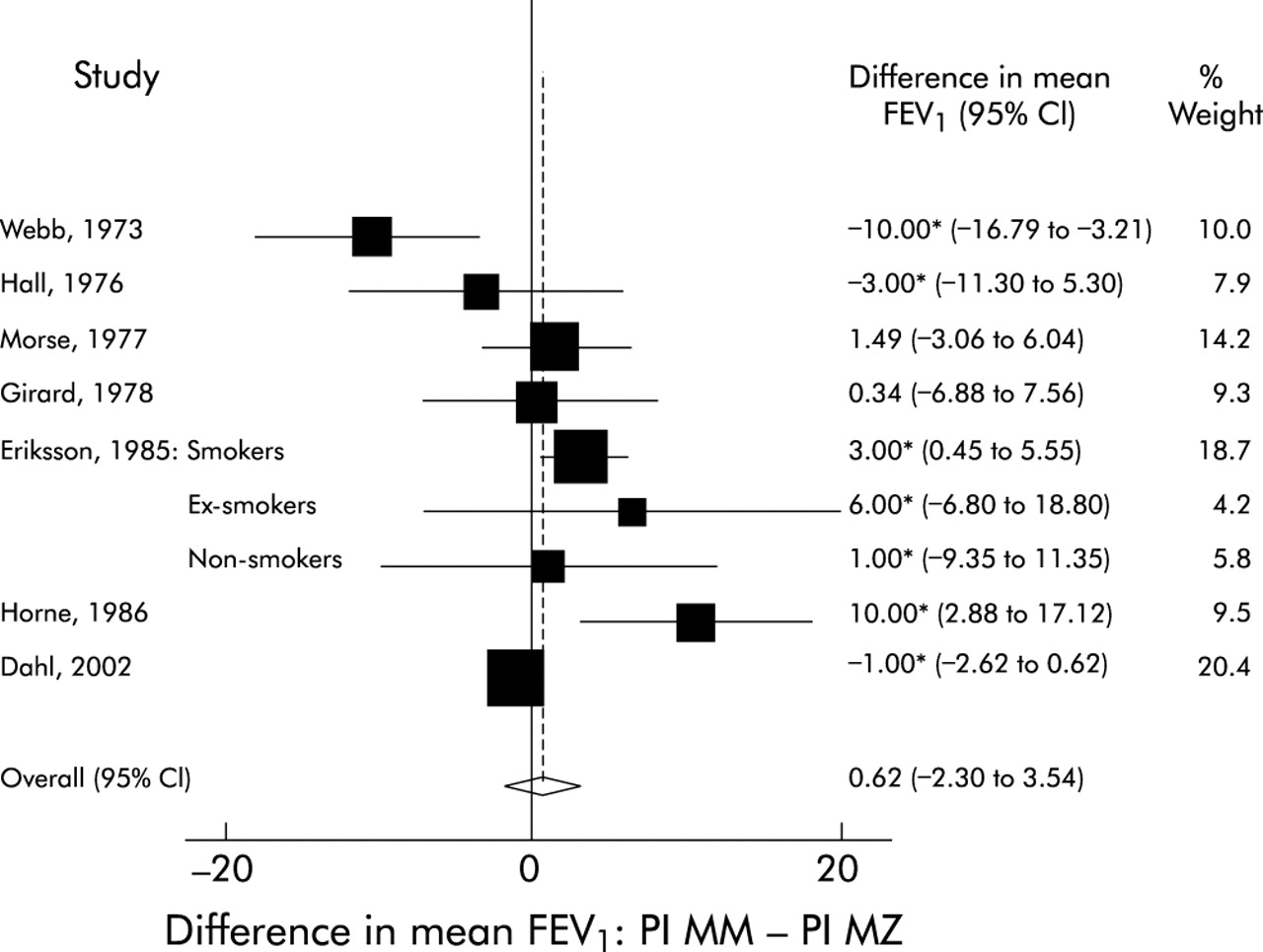
The seven cross sectional studies that compared mean FEV1 (% predicted) in PI MM and PI MZ individuals are shown in table 2. One study from the categorical outcome analysis also reported mean values for FEV1 and was included in the continuous outcome analysis.15 For the one study that reported mean FEV1 values stratified by smoking status, data from the individual strata were entered into the analysis.16 In the pooled analysis (fig 3) there was no difference in mean FEV1 (% predicted) between PI MM and PI MZ individuals (summary difference PI MM – PI MZ = 0.62% predicted, 95% CI –2.30 to 3.54). Significant heterogeneity was detected in these studies (χ28df = 24.4, p = 0.002).
{kind=link}
{kind=link}
{kind=link}
Studies reporting FEV1 as percentage predicted in α1-antitrypsin PI MZ heterozygotes. The mean difference is calculated by subtracting the mean FEV1 (% predicted) of PI MZ individuals from that of PI MM individuals. Sizes of boxes represent inverse variance weights (random effects model).9 Lines represent 95% confidence intervals. *Presented mean FEV1 to the nearest percent.
No asymmetry was detected in the funnel plot of the difference in mean FEV1 versus standard error. Egger’s test did not reveal significant publication bias (p = 0.71). In the sensitivity analysis the mean difference in FEV1 was increased when the study by Dahl et al15 was removed; the mean difference was unaffected when each of the other studies was excluded. Because of the small number of studies, no subgroup analyses were performed for the mean differences in FEV1. A separate analysis of four cross sectional studies that expressed FEV1 in litres (but otherwise met inclusion criteria) was performed.89,91,93,94 There was no difference in mean FEV1 between PI MM and PI MZ individuals (summary difference PI MM – PI MZ = −0.01 litres, 95% CI –0.23 to 0.21).
DISCUSSION
We have conducted a systematic review of the medical literature to evaluate the risk of COPD in AAT PI MZ heterozygotes. Combining studies reporting a categorical outcome, we found moderately increased odds of obstructive lung disease in PI MZ individuals (OR 2.31). As has been noted in previous narrative reviews, the effect estimate was larger in the case-control studies than in the cross sectional studies.6,7 The magnitude of the OR was attenuated in the studies that adjusted for cigarette smoking, but was not substantially different in the subgroup of studies that used objective spirometric criteria to define COPD. The studies measuring lung function as a continuous outcome did not show a difference in mean FEV1 (% predicted) between PI MM and PI MZ individuals.
Overall, the study quality was variable. Only one study fulfilled all four of the quality criteria. The differences in study design and quality, including adjustment for cigarette smoking, probably contribute to the significant heterogeneity found among the studies in the analyses of both the categorical and continuous outcome measures. These studies were all observational, so they are all susceptible to a variety of biases. Some of the studies used different sources for the cases and controls (or PI MM and PI MZ individuals), leading to the possibility of selection bias. Only one study tested for Hardy-Weinberg equilibrium; deviations from Hardy-Weinberg equilibrium could be indicative of problems such as genotyping error or population stratification.118
Confounding by environmental exposures is another potential concern in observational studies. Cigarette smoking is the major environmental risk factor for COPD, but many of the studies did not adjust for smoking as a potential confounder. This is a likely source of heterogeneity between studies. Other potential confounders may also be important, yet control for factors such as age and sex was also inconsistent. In the analysis of lung function as a continuous outcome, the primary analysis included studies that expressed FEV1 as a percentage of predicted since the equations used to calculate the predicted values adjust for important covariates—namely, age, sex, and height. Although different studies used different prediction equations, the same equations were used for both the cases and the controls within an individual study.
A strict phenotype definition is necessary for genetic epidemiology studies,118 but not all of the studies used objective spirometric criteria for the diagnosis of COPD. This may also be a source of heterogeneity between studies. Although the inclusion criteria allowed for different methods of assessment of PI type, this should not lead to important heterogeneity since the included methods are generally quite reliable.119
The divergent conclusions reached by the analyses of the categorical and continuous outcomes require further investigation. Overall, the categorical studies—specifically the case-control studies—showed an increased risk of COPD yet no reduction in mean FEV1 was seen in PI MZ individuals in the cross sectional lung function studies. If PI MZ heterozygosity is a risk factor for COPD, one would expect to find both an increased OR in the categorical studies and a reduction in lung function in the studies measuring continuous outcome; reduced FEV1 is a defining feature of COPD.
If the overall risk increase in PI MZ individuals is uniform but small, then case-control studies may detect this risk more efficiently than cross sectional studies.120 Among the categorical studies, the case-control studies did show an increased OR but the cross sectional categorical studies showed only a trend towards increased risk of COPD in PI MZ individuals.
Alternatively, these results are consistent with an increased risk of COPD in a subgroup of PI MZ individuals. Cigarette smoking may be an important co-factor, and many of the published population based studies may not be large enough to detect this genotype-by-environment interaction. Other genetic factors are likely to modify the risk of development of lung disease in PI ZZ homozygotes,114,121 and it is possible that genetic modifiers of lung disease in PI MZ individuals also exist.
The results of a recent cohort study are consistent with a modifier of COPD risk in PI MZ individuals. Among 1551 PI MZ subjects from the Danish Alpha 1-Antitrypsin Deficiency Registry, the relative risk for hospital admission for obstructive lung disease (asthma, emphysema, or chronic bronchitis) was twice that of population controls.107 First degree relatives of PI Z index cases, with the index cases identified based on respiratory symptoms, were the subgroup responsible for this increased risk. This suggests the presence of other genetic and/or environmental factors aggregating in the families of the PI Z index cases.
Based on this systematic review, the risk of COPD in PI MZ heterozygotes remains uncertain. However, a small increase in risk for all PI MZ individuals or a larger increase in risk in a subgroup of heterozygotes are possible explanations for the apparently discordant results from the analyses of the categorical (especially the case-control studies) and continuous outcome measures. Further studies using rigorous epidemiological methods—including careful control for age, sex, ethnicity, and cigarette smoking—will be required to determine the presence and magnitude of the risk of COPD in PI MZ individuals as a group and in relevant subgroups. It will be important to examine the interaction between PI MZ genotype and cigarette smoking to accurately quantify risk in both smokers and non-smokers. Future studies using other COPD related phenotypes, such as quantitative radiographic measures of emphysema, may also identify clinically relevant subgroups.
Acknowledgments
The authors thank Drs Anne Tybjærg-Hansen, Peter Lange, and Jørgen Vestbo for their helpful suggestions and Dr Clare Ramsey for her assistance with translation from French.
REFERENCES
Footnotes
-
C P Hersh and M Dahl contributed equally to this report.
-
This study was supported by National Institutes of Health grants T32-HL07427 and R01-HL68926 and by grants from the Danish Lung Association and the Danish Heart Foundation.
Linked Articles
- airwaves