Article Text

Abstract
Background: Increased nasal airflow resistance (NAR) may contribute to the pathophysiology of obstructive sleep apnoea syndrome (OSAS) but studies investigating the effects of relieving nasal obstruction in OSAS have produced differing results. There are no reports of intranasal corticosteroid therapy in adult OSAS patients with reversible nasal obstruction.
Methods: We evaluated an intranasal corticosteroid, fluticasone propionate, in 24 consecutive snorers with associated rhinitis using a randomised, placebo controlled, crossover design. Patients underwent polysomnography, snoring noise, and NAR measurements at baseline and after each 4 week treatment period.
Results: Twenty three patients completed the protocol and were divided into an apnoeic group (group A; 13 patients) and a non-apnoeic snoring group (group S; 10 patients) based on an apnoea-hypopnoea frequency (AHI) of ⩾10/h or <10/h. AHI was significantly lower following treatment with fluticasone than with placebo in the total population (median (quartile range) 11.9 (22.6) v 20 (26.3); p<0.05) and in group A (23.3 (21.3) v 30.3 (31.9); p<0.05). Median (95% confidence interval) within subject differences for AHI were −3.2 (−17.7 to −0.2) in the total population and −6.5 (−29.5 to 1.8) in group A. NAR was also lower on fluticasone (2.74 (1.21) v 3.27 (1.38), p<0.01), within subject difference being −0.45 (95% CI −0.87 to −0.21). The changes in AHI and NAR in group A were significantly correlated (r = 0.56; p<0.05). Snoring noise and sleep quality were unchanged but daily diary records indicated subjective improvements in nasal congestion and daytime alertness with fluticasone (p<0.02).
Conclusions: Intranasal fluticasone is of benefit to some patients with OSAS and rhinitis. The data suggest that this form of nasal obstruction may contribute to the pathophysiology of OSAS.
- intranasal corticosteroids
- sleep apnoea
- rhinitis
Statistics from Altmetric.com
Increased nasal airflow resistance (NAR) may contribute to the development of upper airway obstruction during sleep,1 and several studies have reported snoring and obstructive sleep apnoea in patients with nasal obstruction of various aetiologies.2–4 However, the impact of relieving nasal obstruction on the severity of obstructive sleep apnoea syndrome (OSAS) is unclear, with some reports indicating reductions in apnoea-hypopnoea frequency (AHI) following surgical intervention5 or with medical treatment6 while other studies have failed to demonstrate improvement.7,8 Furthermore, studies that have quantified NAR in unselected patients with OSAS have produced differing results, some finding higher NAR in patients with OSAS than in non-apnoeic controls9 while others have failed to show a difference.10,11 These different findings have cast some doubt on the importance of nasal obstruction in OSAS.
The potential role of nasal obstruction in the pathophysiology of OSAS and its treatment has particular clinical relevance because of the high prevalence of nasal obstruction in the general population. A particularly frequent cause of nasal obstruction is rhinitis, either seasonal or perennial, which is reported in up to 26% of the general population.12 Intranasal corticosteroids are commonly used to treat rhinitis, but no previous study has evaluated the efficacy of corticosteroids in the treatment of OSAS among adult patients with rhinitis. A study was therefore undertaken to examine the efficacy of intranasal fluticasone propionate, a topical corticosteroid, in a group of patients with snoring and rhinitis who were being investigated for suspected OSAS. The aims were to assess the efficacy of fluticasone on sleep apnoea severity, snoring noise, sleep quality, and daytime symptoms.
METHODS
Twenty four consecutive adult patients were enrolled from patients referred to our respiratory sleep disorders clinic for sleep studies because of a clinical suspicion of OSAS. All had a history of loud snoring and symptoms compatible with rhinitis, either perennial or seasonal. The study design was chosen to minimise the possibility of selection bias and to provide a spectrum of disease ranging from clinically significant OSAS to non-apnoeic snoring. Our clinical experience is that about 60% of snorers referred for sleep studies have an AHI of ⩾10/h. An a priori decision was made to divide patients into apnoeic and non-apnoeic snorers based on an AHI threshold of 10 events/h during the baseline sleep studies. The criteria for rhinitis were the presence of nasal congestive symptoms, which varied in both time and laterality. Patients with fixed nasal obstruction such as previous nasal fracture or deviated septum were excluded. No other medications that could influence nasal patency, such as antihistamines and decongestants, were allowed during the study, and no subject was on bronchodilator or corticosteroid inhalers.
The protocol used a randomised, double blind, placebo controlled, crossover design with each treatment lasting 4 weeks. Patients were randomly assigned to receive either fluticasone by aqueous nasal spray 100 μg twice daily or matching placebo spray, both supplied by Glaxo Wellcome plc. After 4 weeks each subject was switched to the alternative preparation for a further 4 weeks. All patients had polysomnography and nasal airflow resistance (NAR) measurements before and after sleep at the commencement of the study to establish baseline data and to allow familiarisation with the study techniques, and in particular to reduce the likelihood of a first night effect influencing the comparison of fluticasone with placebo. Polysomnography together with pre and post sleep NAR measurements were repeated at the end of each treatment period. The primary study end point was the change in AHI between sleep studies performed at the end of the placebo and fluticasone treatment periods, and secondary end points were objective sleep quality, measured snoring noise, nasal resistance, and diary record scores compared between the same treatment periods.
Our hospital ethics committee approved the study and all patients gave written informed consent.
Sleep studies
Polysomnography was performed using the Medilog SAC847 system (Oxford Instruments, Oxford, UK). Sleep studies were manually analysed according to standard criteria13 by an experienced technician who was blinded to the patient’s identity and treatment status.
Nasal airflow resistance (NAR) measurement
NAR was measured by posterior active rhinomanometry (PRh) while seated and consisted of simultaneous transnasal pressure and flow measurements which were digitised and recorded by computer. Nasal airflow was measured with a calibrated pneumotachograph (Fleisch, Switzerland) attached to a modified nasal mask and a calibrated Validyne transducer (model DP45-26; Validyne Engineering, Northbridge, CA, USA). The mask was carefully fitted to avoid air leakage and compression or distortion of the nasal passages. The transnasal pressure gradient (ΔP) was the difference in pressures between the mask (P1) and the posterior oropharynx (P2) measured through a modified 8.5 mm endotracheal tube (Mallinckrodt). Both pressures were measured with a Validyne DP45-14 transducer.
The flow and pressure signals were captured by a 16-bit analogue to digital converter (MP100WSW, Biopac Systems, Santa Barbara, CA, USA) at a sampling rate of 100 Hz, and displayed on the computer in real time. ΔP was plotted against simultaneous nasal airflow and a ΔP of 1.5 cm H2O was used as the reference gradient14,15 at which NAR was calculated according to the equation NAR = ΔP/airflow (cm H2O/l/s). Repeated recordings were performed over 5 minutes and the mean value calculated for NAR. The data were reproducible within individuals if measured over a short time period in the same body position. Measurements were made at the same time each evening and morning before and after bed, and before treatment. The mean of the pre-sleep and post-sleep values was used to compare NAR between fluticasone and placebo. Mean (SD) NAR in normal controls in our centre is 2.11 (0.77) cm H2O/l/s.
Measurement of snoring
Two calibrated microphones were used: one, a small (0.75 cm × 1.5 cm) omni-directional pre-polarised condenser microphone (C407, AKG Acoustics, Munich, Germany) placed at the nasion recorded snoring noise, and a second omni-directional microphone (CK92 and SE300B, AKG Acoustics, Munich, Germany) recorded room noise. Microphone signals were amplified and digitised and a calibration scale was constructed against the simultaneously recorded noise level for each microphone using a sound meter (SL120, Wessels Messtechnik, Neuss, Germany). Before the study the acoustic characteristics of the bedroom were analysed and a sound baffle positioned to flatten the acoustic profile, thus minimising distortion to the room microphone sound detection.
The nasion microphone was fixed to the nose 6 cm above the external nares and recorded both nasal and oronasal snoring noise. The sound meter and room microphones were suspended 60 cm above the nares with the patient supine. The signals were amplified and moving-time averaged with a time constant of 100 ms. Snoring noise was recorded at a sampling rate of 50 Hz by the computer. A threshold of 63 dB(C) measured by the nasion microphone was chosen as most appropriate for the detection of snoring following several overnight pilot studies. Noise recordings below this level were considered as possible artifacts and excluded from the analysis. Data were analysed by the software package used in the analogue-digital converter (AcqKnowledge 3.0, Biopac Systems, Santa Barbara, CA, USA), apportioning the total number of samples into a series of 5 dB “bins” (that is, 63–67 dB(C) etc).
Diary records
For each of the two 4 week study periods patients completed a daily diary of four symptoms—namely, sleep quality, nasal congestion, daytime alertness, and snoring intensity as perceived by bed partners. The questions were answered on a 4 point scale in which a score of 1 indicated the best positive answer for a symptom (least severity) and 4 indicated the most negative answer (highest severity). Daily data were analysed for weeks 2–4 of each treatment period and the mean score for each period was compared between fluticasone and placebo. The first week was regarded as representing treatment stabilisation or between treatment washout.
Statistical analysis
In keeping with the study design, tests for period effect and treatment × period interaction were performed by analysis of variance (ANOVA).16 The data were analysed for the total group and separately for the subgroups of apnoeic and non-apnoeic snorers. Paired data were analysed using Wilcoxon’s (non-parametric) matched pairs test. All analyses were performed with a commercial package (Statistica, StatSoft, Tulsa, Oklahoma, USA) and rechecked by an independent statistician.
RESULTS
There was no evidence of any significant period or order effect or treatment × period interactions during the study. Twenty three patients completed the protocol but one other was excluded because he self-medicated with nasal decongestants, thus violating the protocol; there were 19 men and four women. Thirteen patients had an AHI of >10/h and 10 had an AHI of <10/h at baseline (table 1); these measurements were used to divide the study population into apnoeic (group A) and non-apnoeic snorers (group S). Group A patients were also significantly sleepy with a mean (SD) Epworth score of 12 (2.6) consistent with a clinically significant sleep apnoea syndrome,17,18 whereas most of the patients in group S were not sleepy (Epworth scores <9). Patients in group A were significantly heavier than those in group S (table 1). There were no significant differences between baseline and placebo values for AHI or NAR in the group analysed as a whole or as subgroups.
Clinical details of total study population (all) and the subgroups of non-apnoeic (S) and apnoeic (A) snorers
Severity of sleep apnoea
AHI was significantly lower in patients on fluticasone than on placebo in the total population and in group A (p<0.05; table 2). Median within subject differences were −3.2 (95 CI −17.7 to −0.2) in the total population, −6.5 (95% CI −29.5 to 1.8) in group A, and −1.25 (95% CI −6.51 to 1.31) in group S. The changes in AHI for individual patients are shown in fig 1. Using a lower AHI threshold of 5/hour for diagnosing OSAS as recommended by the recent American Academy of Sleep Medicine report,18 AHI was still significantly less on fluticasone than on placebo (17 (23.6) v 24.3 (28.4) events/h; n = 18, p = 0.01), with a within subject difference of −5.6 (95% CI −22.8 to −0.7) events/h.
Sleep apnoea severity, sleep quality, nasal airflow resistance, and diary record details during treatment with fluticasone and placebo

Comparison of apnoea-hypopnoea index (AHI) with placebo (P) and fluticasone (F) after treatment for 4 weeks in individual apnoeic (group A) and non-apnoeic (group S) snorers. Allocation to groups A or S was based on the AHI in the baseline sleep study.
Nasal airflow resistance (NAR)
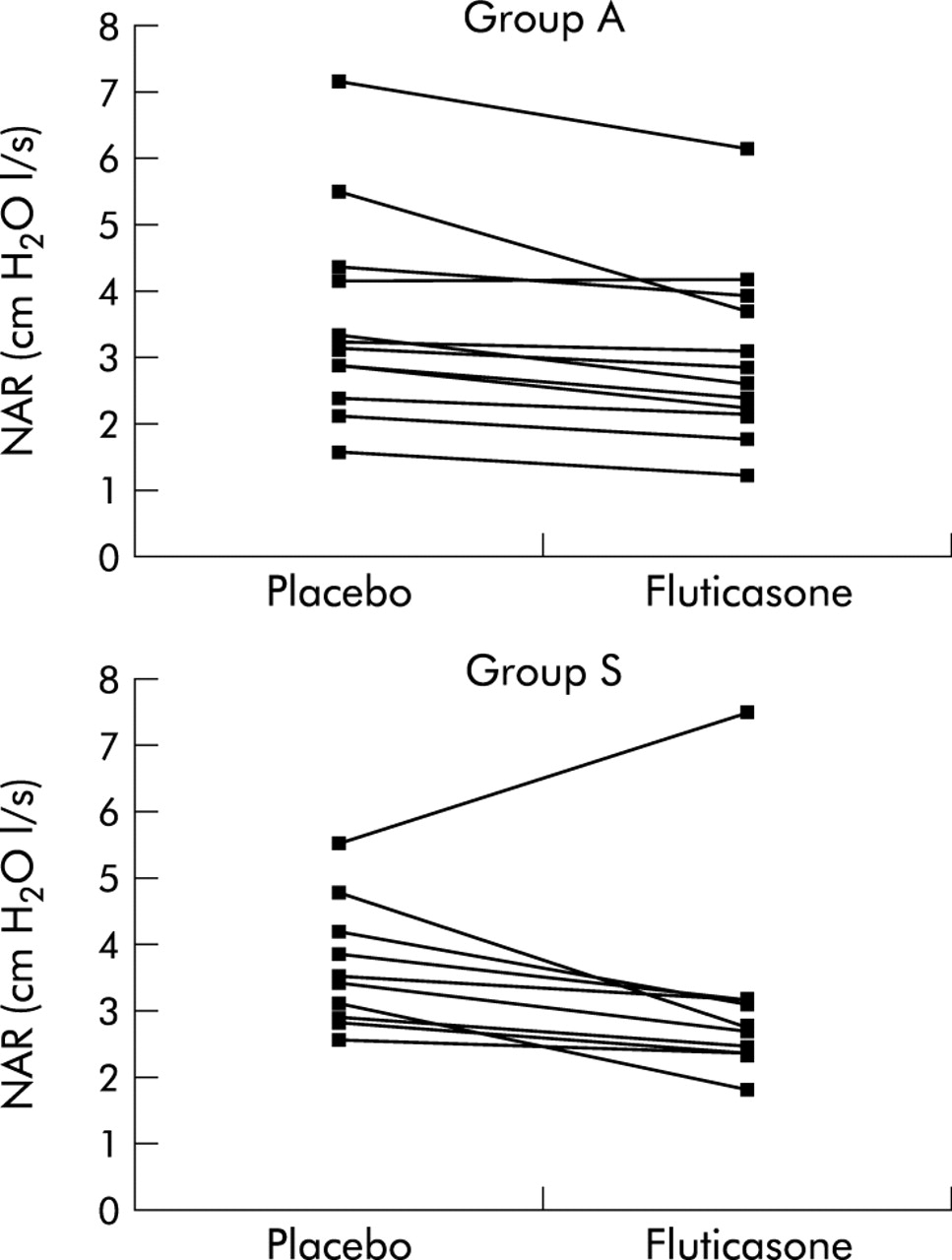
NAR fell with fluticasone in the total population (p<0.01) and in group A (p<0.01) and a strong trend towards a reduction was seen in group S (p = 0.06; table 2). Median within subject differences were −0.45 (95% CI −0.87 to −0.21) in the total population, −0.4 (95% CI −0.84 to −0.25) in group A, and −0.59 (95% CI −1.26 to 0.20) in group S. Data for individual patients are shown in fig 2. The differences in AHI between placebo and fluticasone correlated significantly with the differences in NAR in group A patients (Spearman’s r = 0.56, p = 0.05; fig 3).
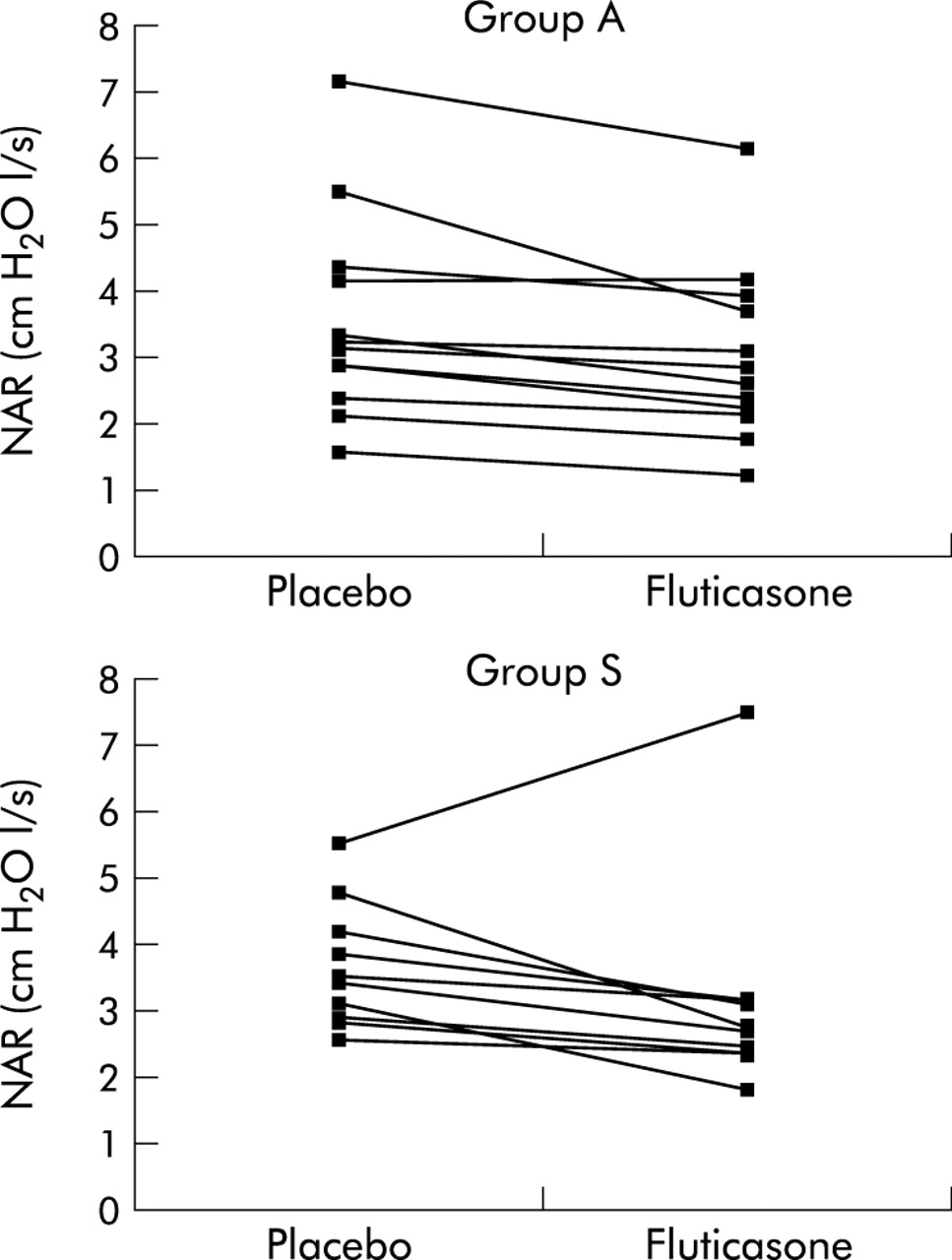
Comparison of nasal airflow resistance (NAR) between placebo and fluticasone after 4 weeks of treatment in individual apnoeic (group A) and non-apnoeic (group S) snorers.
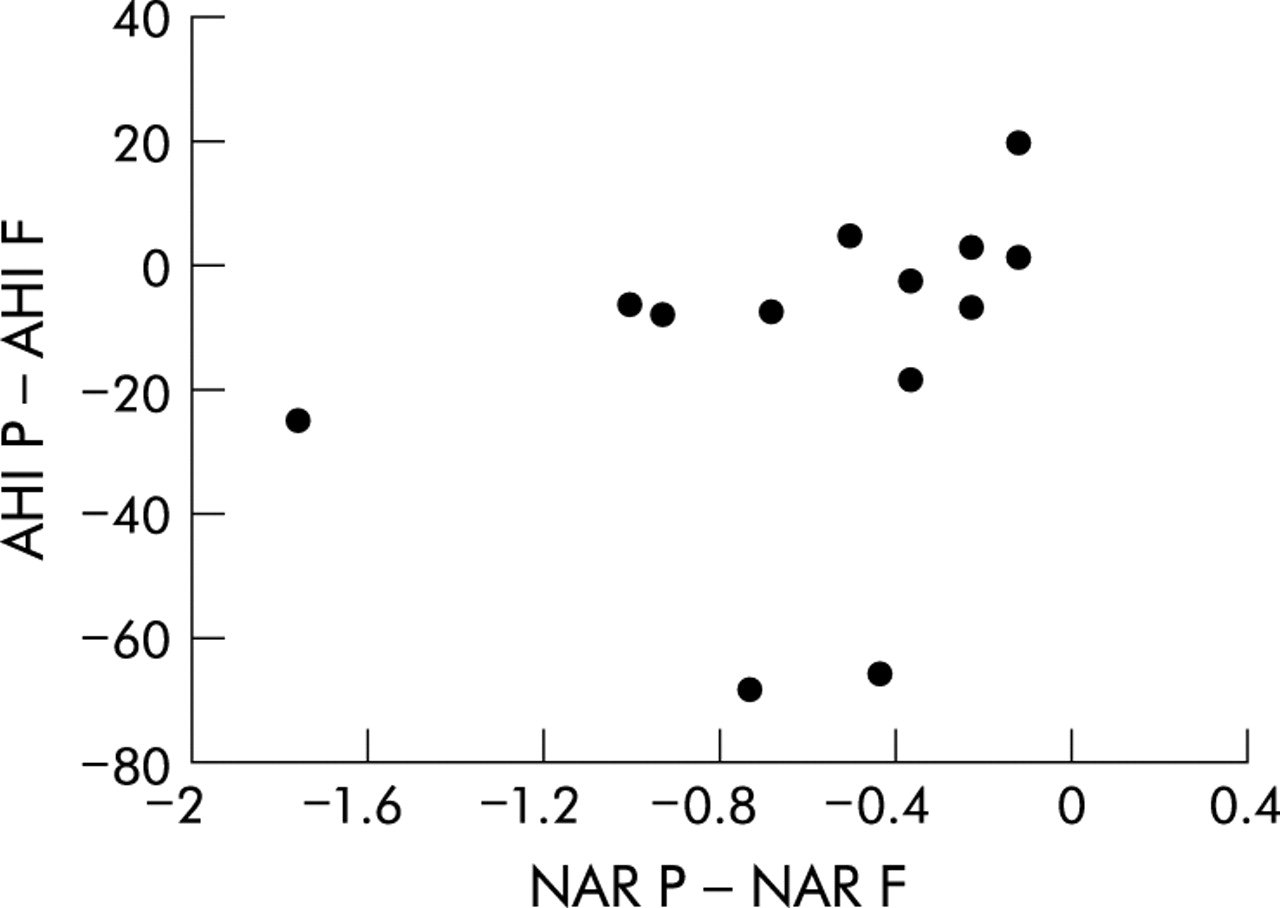
Correlation between the change in apnoea-hypopnoea index (AHI, events/h) and the change in nasal airway resistance (NAR, cm H2O/l/s) between fluticasone and placebo (AHI P − AHI P v NAR P − NAR F) in patients with sleep apnoea. The relationship was statistically significant (Spearman’s r = 0.56, p<0.05).
Objective sleep quality
Details of overnight sleep studies are given in table 2 and show little difference in objective sleep quality when fluticasone and placebo nights are compared. However, there was an increase in stages 3 and 4 (slow wave sleep) of borderline significance on fluticasone (p = 0.06). No differences were observed for REM sleep. A trend for more slow wave sleep was also observed separately in both groups A and S on fluticasone. No differences were seen in sleep efficiency (TST as a percentage of sleep period time) in group A or in the total population on fluticasone compared with placebo, although sleep efficiency was significantly improved in group S on fluticasone.
No significant differences were observed in mean or lowest oxygen desaturation between treatments. However, in the 15 patients with increased baseline NAR (>3.0 cm H2O/l/s) the median (quartile range) number of desaturations of ⩾4% per hour of sleep was significantly lower on fluticasone than on placebo (12.0 (25.1) v 11.7 (32), p = 0.035) with a median within subject difference of −2.15 (95% CI −7.0 to 0.14).
The automated detection of arousals by the polysomnography system software was found not to be reliable on visual inspection of the polysomnographic tracings and, although the arousal frequency was lower in group S on fluticasone than on placebo, we feel that no reliable conclusions can be drawn since the system did not allow manual editing of arousal scores.
Snoring
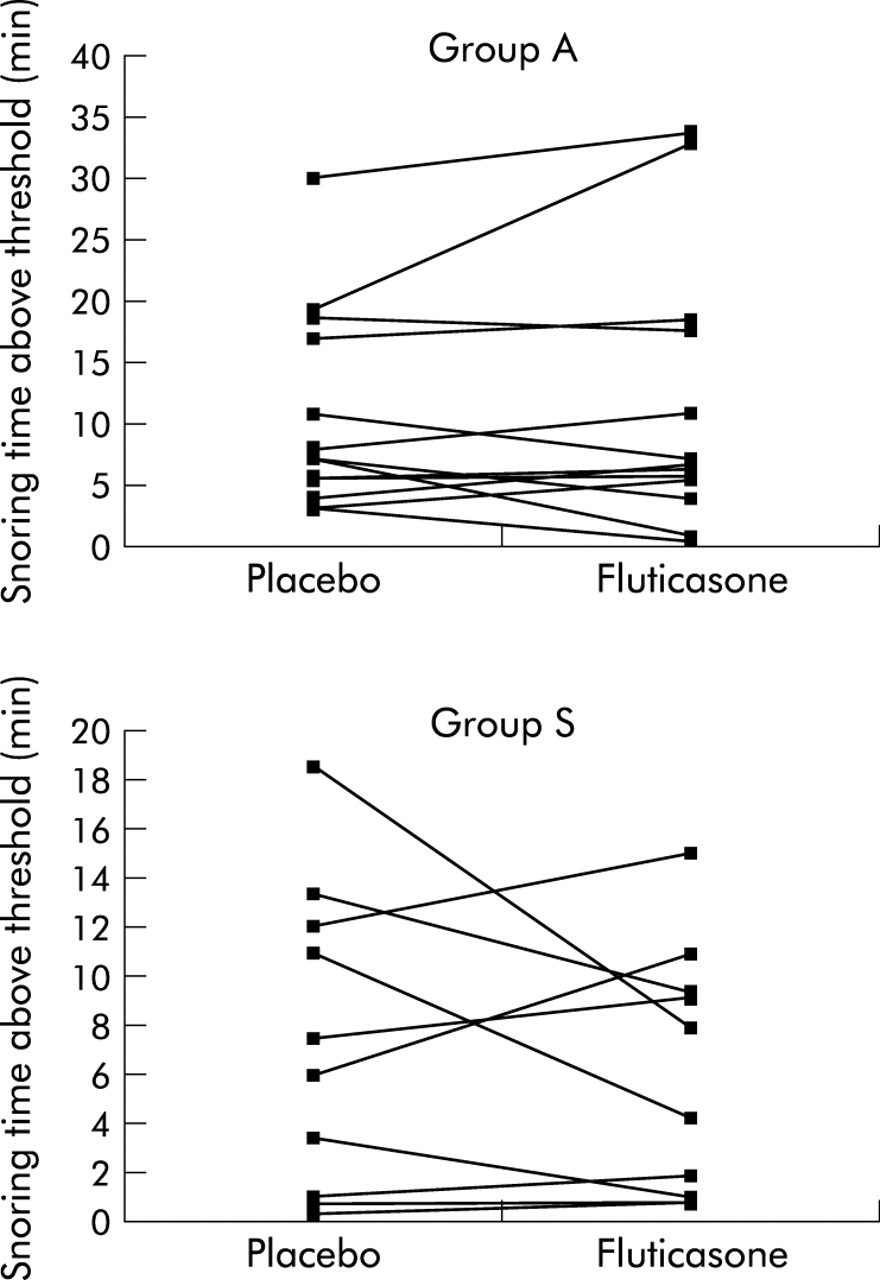
Figure 4 provides individual patient data for snoring noise above the chosen threshold of 63 dB(C) on fluticasone and placebo. There were no significant differences in snoring noise between fluticasone and placebo in the total group, or separately for either group A or S. This was true when overall snoring intensity was analysed as total time above threshold levels and also when the intensity distribution of snoring noise was analysed in 5 dB segments.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Snoring characteristics of patients in group A (top) and group S (bottom) after 4 weeks of treatment with placebo or fluticasone. Snoring noise data are displayed as time in minutes spent above the threshold of 63 dB(C) as discussed in the text.
Diary record cards
There were significant improvements with fluticasone in symptoms of nasal congestion (p = 0.02) and daytime alertness (p = 0.02) in the total population and in group S, but no significant differences for sleep quality or partner-reported snoring intensity (table 2). Median within subject differences for nasal congestion were −0.18 (95% CI −0.38 to −0.03) in the total population, 0 (95% CI −0.19 to 0.14) in group A, and −0.36 (95% CI −0.75 to −0.12) in group S, and for daytime alertness were −0.16 (95% CI −0.36 to 0.0) in the total population, −0.10 (95% CI −0.22 to 0.08) in group A, and −0.23 (95% CI −0.72 to 0.07) in group S.
DISCUSSION
The findings of this study indicate a significant improvement in the severity of OSAS but not in snoring noise levels in patients with OSAS and associated rhinitis following intranasal corticosteroid treatment, and indicate that this treatment may benefit selected patients with OSAS. The data also support a role for nasal obstruction in the development of OSAS in patients with increased NAR, particularly since there was a significant correlation between the differences in NAR and AHI on fluticasone and placebo study nights (fig 3).
The nose and upper airway can be viewed as a form of Starling resistor19 with a collapsible segment in the oropharynx. Increased NAR results in a more negative intrapharyngeal pressure during inspiration which may predispose to oropharyngeal collapse since the nose represents the primary route of breathing, particularly during sleep.20 NAR increases in the recumbent position,21,22 and thus would be expected to rise during sleep. This increased NAR may predispose to OSAS in susceptible individuals, and patients with seasonal allergic rhinitis2 and occupational allergen induced rhinitis23 have been reported to have higher apnoea frequencies during periods of higher NAR than during asymptomatic periods when NAR is normal. Even in the absence of disordered breathing during sleep, prolonged nasal obstruction may affect waking function, probably due to sleep disturbance.24
We recognise that some studies have failed to show an association between nasal obstruction and OSAS,10,11 although NAR has been shown to correlate significantly with snoring.25 Some of these reports have analysed NAR in unselected patients with suspected OSAS and have not specifically focused on patients with nasal obstruction.10 Other studies that assessed the impact of surgical correction of anatomical nasal obstruction have produced differing conclusions on the benefits to OSAS.5,8,26 The role of symptomatic nasal obstruction in the pathophysiology of OSAS is therefore not yet clear. However, we believe that the present report, in combination with previous reports that have examined the influence of nasal obstruction due to the vascular engorgement of rhinitis in selected subjects with obstructive sleep apnoea,2,23 support the hypothesis that this type of reversible nasal obstruction predisposes to OSAS. Kramer and colleagues reported no increase in the incidence of OSAS in a small group of patients with allergic rhinitis compared with other patients being investigated for OSAS, but NAR was not measured.27
We failed to show a benefit from fluticasone on snoring noise, either by objective measurement in the laboratory or by subjective assessment in the diary records. However, the duration of time spent above the threshold of 63 dB(C) was relatively short in most patients, which may reflect the fact that patients were not objectively prescreened to include only patients who snored loudly for most of the night. Nonetheless, all subjects presented with snoring as a prominent symptom and thus represent a cross section of patients presenting to a clinical sleep disorders unit. The threshold level of 63 dB(C) was chosen to exclude normal breathing sounds, movement and intermittent extraneous noises, but was sufficiently low to ensure that all snoring noise of moderate or greater intensity would be included. Previous studies of the impact of treating nasal obstruction on snoring noise have reported differing findings,7,28–30 and therefore the potential benefit of relieving nasal obstruction to reducing snoring noise remains unproven.
Despite the improvements in AHI with fluticasone, the data indicate that intranasal corticosteroids are likely to have a limited clinical role in the management of OSAS since most patients continued to have significant OSAS on treatment. Nonetheless, the fall in mean AHI in the apnoeic group from 40 to 26 (median values fell from 30.3 to 23.3; table 2) moved this group from severe OSAS to moderate OSAS as recently proposed18 and, overall, the AHI fell by about 40% in the total population and in group A. Changes in objective sleep quality were small and of questionable clinical significance, but did show a trend towards increased slow wave sleep with fluticasone.
We chose an AHI threshold of 10/h to define OSAS, which is higher than the recent proposal18 that an AHI of 5/h together with daytime symptoms should be the minimum requirement for a clinically significant sleep apnoea syndrome. This threshold of 10/h would have been widely accepted at the time of our study but the choice did not significantly influence our findings since the benefits of fluticasone were evident in the total population and also among OSAS patients regardless of whether an AHI threshold of 5/h or 10/h was used. We also recognise that there are limitations in using AHI on single night sleep studies as the primary end point because of the likelihood of night-to-night variability. However, this variability should not have introduced any consistent bias in favour of fluticasone. Furthermore, we recognise that it would have been preferable to measure NAR in the recumbent position but this was not possible because of practical considerations in our laboratory.
This study represents the first report of treatment with intranasal corticosteroids in adult patients with OSAS. However, a recent report by Brouillette and coworkers31 documented improvements in OSAS severity in children with OSAS and adenotonsillar hypertrophy treated for 6 weeks with intranasal fluticasone. The mechanism of benefit in this study is unclear since NAR was not measured.
Nasal continuous positive airway pressure (CPAP) remains the treatment of choice for patients with moderate to severe OSAS. However, patients with mild OSAS—who constitute the majority of patients—are less likely to tolerate this cumbersome treatment and effective alternatives are desirable. Furthermore, compliance studies of nasal CPAP treatment indicate an average usage of 5–6 hours per night.32 Thus, patients are exposed to the potential harmful effects of untreated OSAS when sleeping without the device in place. These considerations indicate that intranasal corticosteroids may be effective as part of a treatment strategy for patients with mild to moderate OSAS where there is co-existing rhinitis, and in some patients with more severe OSAS, together with nasal CPAP therapy.
Acknowledgments
The authors wish to acknowledge C Hallett for his contribution to the statistical analysis, and also G Lawless, C Delahunty, and S Matthews who performed the sleep studies.
REFERENCES
Footnotes
-
Supported by a grant from Glaxo Wellcome plc.