Article Text

Abstract
Background: A study was undertaken to examine the dose-response relation of inhaled fluticasone in adolescents and adults with asthma.
Methods: A meta-analysis was carried out of randomised clinical trials that presented data on at least one outcome measure of asthma and that used at least two doses of fluticasone given twice daily. The main outcome measures were forced expiratory volume in 1 second (FEV1), morning peak expiratory flow (amPEF), β agonist use, and withdrawals due to exacerbations of asthma.
Results: Seven studies of 2431 adolescents and adults with moderate to severe asthma met the inclusion criteria for the meta-analysis. Four studies examined a dose of >500 µg/day. For all outcome measures there were no statistically significant differences between a dose of 200 v 500 μg/day, 500 v 1000 μg/day, and 200 v ⩾500 µg/day, although the point estimates favoured the higher doses. The mean improvement for FEV1 and amPEF resulting from an increase in dose from 200 to ⩾500 µg/day was 0.07 l (95% CI −0.01 to 0.14) and 5.9 l/min (95% CI −3.0 to 15.3), respectively. The odds ratio for withdrawals with 200 µg/day compared with ⩾500 µg/day was 1.27 (95% CI 0.78 to 2.07).
Conclusions: In adolescents and adults with asthma, most of the therapeutic benefit of fluticasone is achieved with a total daily dose of 200 µg/day with minimal further clinical benefit achieved with higher doses. This conclusion is qualified by the recognition that there is considerable individual variability in the response to inhaled corticosteroids in asthma, which would suggest that some patients may obtain a greater clinical benefit at higher doses.
- asthma
- inhaled corticosteroids
- fluticasone
- dose-response
Statistics from Altmetric.com
We have shown in a previous meta-analysis of placebo controlled dose-response studies of fluticasone propionate in adults and adolescents that the dose-response curve begins to plateau at around 100–200 µg/day with the maximum achievable therapeutic benefit obtained with a dose of around 500 µg/day.1 However, the interpretation of these findings was limited by the small number of studies that included doses of more than 500 µg/day because of the requirement for studies to be placebo controlled. This led to the exclusion of two large dose-response studies involving 895 subjects which included a 1000 µg/day treatment group that would have provided greater power and allowed the dose-response above 500 µg/day to be more accurately determined.2,3
This present meta-analysis was undertaken to determine with greater certainty the dose-response relation of fluticasone, particularly at higher doses. We have specifically focused on comparisons between a dose of 200 µg/day and higher doses to determine whether the 200 µg/day dose regime provides most of the therapeutic benefit as was suggested in our previous study. For all major clinical outcome measures including exacerbations, comparisons were made between the dose levels of 200, 500 and 1000 µg/day of fluticasone, which represent the standard dosage regimes provided by inhalers currently available to clinicians.
METHODS
Search strategy
We conducted a search of Medline from 1 January 1966 to August 2002 and of Embase from 1980 to August 2002. On Medline we combined a search of studies containing the keyword “fluticasone” with a search using the MeSH subject heading “asthma” and “chemical and pharmacologic phenomena” (MeSH) or “dose-response relationship, drug” (MeSH) or the keywords “dose” or “dosage”. When limited to English, the total number of studies was 275. We also asked GlaxoSmithKline, the manufacturer of fluticasone, for details of all relevant studies; no additional studies were identified. We did not find any relevant studies published in other languages on Medline and Embase. Finally, we examined the reference lists of relevant studies but found no others. The search strategy as recommended by the QUORUM statement is shown in fig 1.

Process of inclusion of studies in the meta-analysis.
Inclusion criteria
Two people examined the title and abstract of each paper, then the full paper if necessary. To be included in this meta-analysis, studies had to meet all the following criteria: a double blind, randomised trial of adolescents (⩾12 years of age) or adults with asthma; two or more doses of fluticasone ⩾200 µg per day given twice daily; studies were of at least 6 weeks’ duration; and data on measures of clinical efficacy were reported. Studies in which participants were dependent on oral steroids or involved in oral steroid reduction regimes were excluded.
Data extraction
Extraction of data was based on reported summary statistics (means, standard deviations, standard errors of means) for the intention to treat population. The outcome measures assessed were forced expiratory volume in 1 second (FEV1) measured at the clinic, morning peak expiratory flow (amPEF), use of β agonists, total withdrawals, and exacerbations of asthma leading to withdrawal. Several other outcome measures were used in some studies—for example, quality of life questionnaires and symptom scores—but these were not analysed as they were assessed using non-comparable methods (for example, different types of symptom score or data in the format required were not available). In one study4 the amPEF was measured from the figure. The mean values for change in amPEF from this figure did not correspond to the values given in the table; however, only the graphical data presented standard deviations and could therefore be included in the analysis.
Data analysis
For the four major clinical outcome variables (FEV1, amPEF, β agonist use, and withdrawals due to asthma) comparisons were made between a dose of 200 v 500 µg/day, 500 v 1000 µg/day, 200 v 1000 µg/day, and 200 v ⩾500 µg/day. The comparison of 200 v ⩾500 µg/day represented the primary outcome of interest.
For continuous variables (FEV1, amPEF, and β agonist use) the standardised mean difference was pooled using the inverse variance weighted method, treating the studies as random effects.5 The weighted standard deviation was calculated for each dose comparison using the average of the study dose group standard deviations weighted by the number of subjects in each study dose group. This was multiplied by the estimates of the pooled standardised mean difference to give an estimate of the difference between the two groups in the original units of measurement. For the binary outcome variable the odds ratio for withdrawals was pooled using the inverse variance weighted method for the logarithm of the odds ratio and treating the studies as random effects.5
RESULTS
Seven studies met the criteria for inclusion in this analysis.2–4,6–9 These studies, which were funded by Glaxo Wellcome (the manufacturer of fluticasone), were published between 1994 and 1999 and were of 6–24 weeks duration (table 1). A total of 2431 adolescents and adults with asthma were included in the studies, with a mean age of 37 years (range 12–87). All studies involved patients with moderate or severe asthma with a mean FEV1 of 67% of predicted (range 45–90%) at enrolment.
Summary of studies used in the meta-analysis
Primary analyses
200 v ⩾500 µg/day
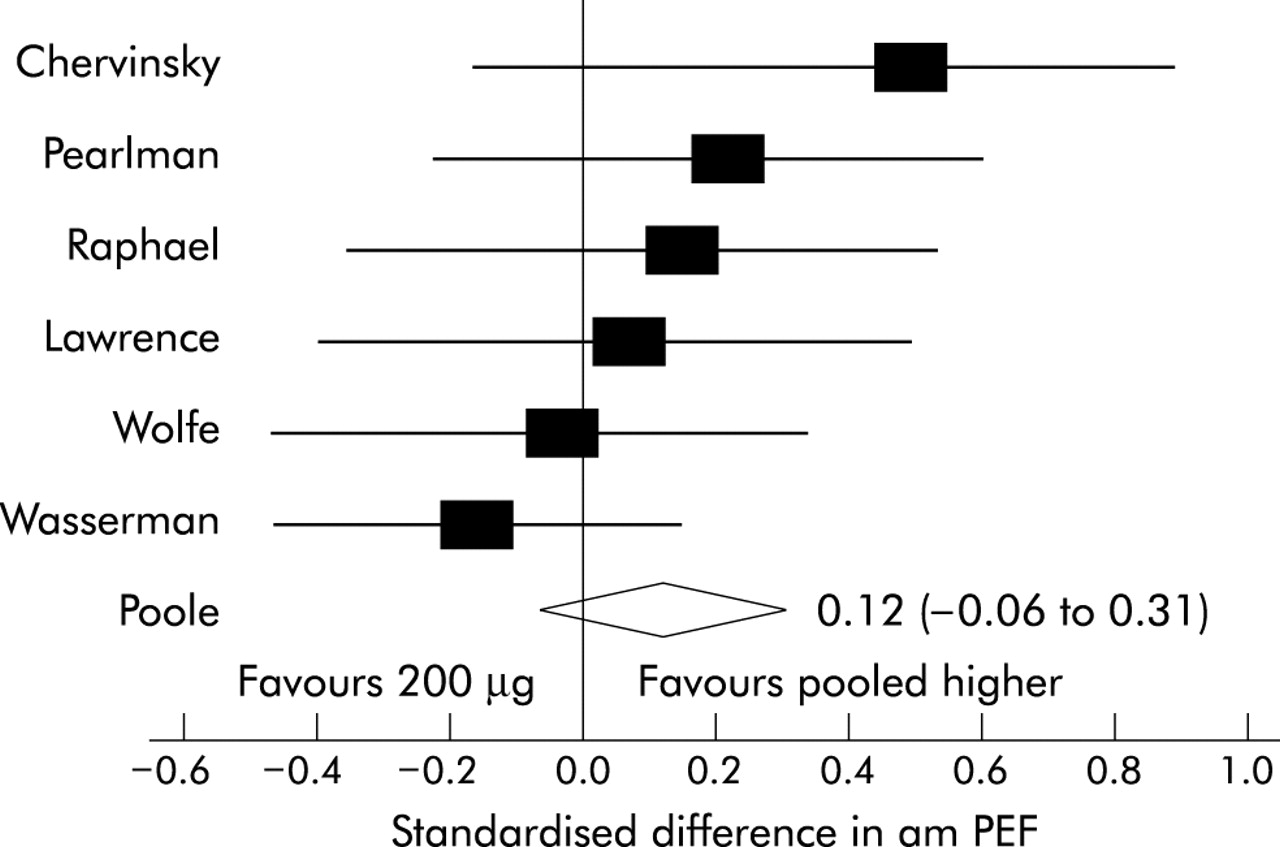
There was no statistically significant difference in FEV1, amPEF, or β agonist use between the 200 μg/day and ⩾500 µg/day dose regimes, although for all three outcomes the point estimates favoured the higher dose group (table 2, figs 2–4). The difference using weighted average standard deviation was 0.07 l (95% CI −0.01 to 0.14) for FEV1, 5.9 l/min (95% CI −3.0 to 15.3) for amPEF, and −0.05 puffs per day (95% CI −0.34 to 0.25) for β agonist use. The withdrawals due to asthma also favoured the ⩾500 µg/day group although the confidence intervals were wide: odds ratio 1.27 (95% CI 0.78 to 2.07), fig 5.
Pooled difference (95% CI) using weighted standard deviation

Forest plot for FEV1: 200 µg versus higher doses.
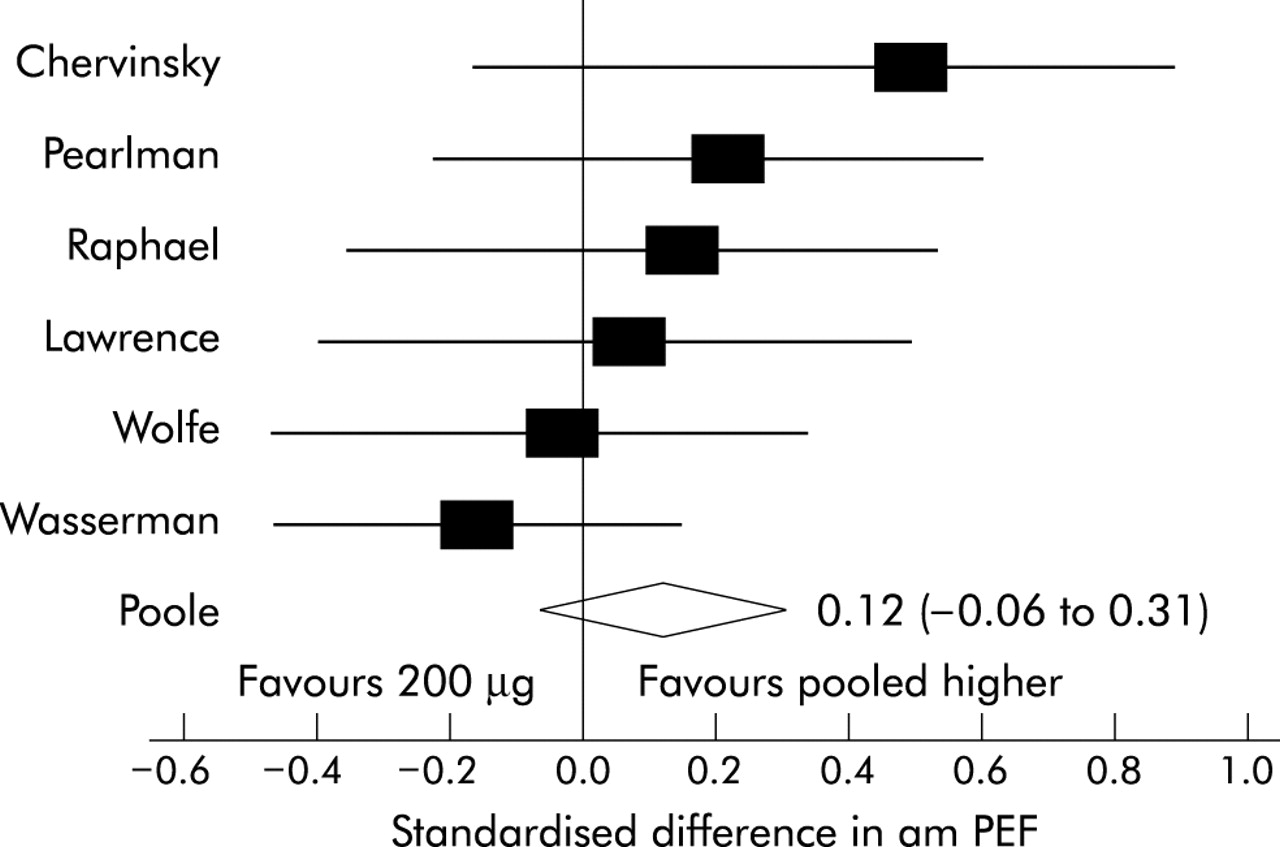
Forest plot for amPEF: 200 µg versus higher doses.
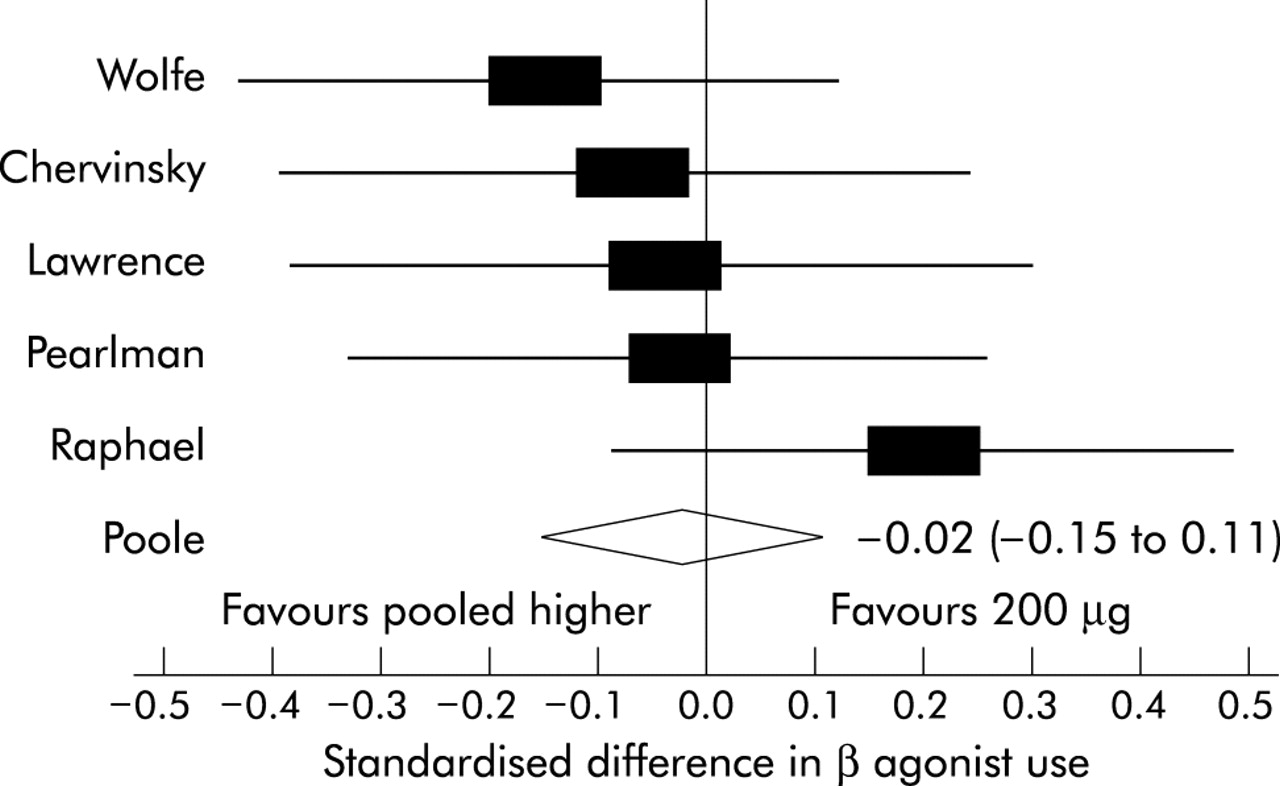
Forest plot for β agonist use: 200 µg versus higher doses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for odds ratio of study withdrawals due to exacerbations: 200 µg versus higher doses.
Secondary analyses
200 v 500 µg/day
There was no significant difference in FEV1, amPEF, or β agonist use between the dose regimes, although all the point estimates favoured the 500 µg/day group (table 2). The pooled risk of withdrawals due to asthma favoured the 500 µg/day group, but the 95% confidence intervals were also consistent with no difference: odds ratio 1.23 (95% CI 0.71 to 2.13).
500 v 1000 µg/day
Data were only available for amPEF and for withdrawals due to asthma. For amPEF the difference using weighted average standard deviation was 7.5 l/min (95% CI −2.8 to 17.4). For withdrawals due to asthma, both studies favoured the higher dose but the confidence interval was again wide: odds ratio 1.17 (95% CI 0.48 to 2.90).
200 v 1000 µg/day
The 1000 µg/day dose resulted in a significantly greater increase in FEV1 of 0.13 l (95% CI 0.03 to 0.24) compared with the 200 µg/day dose. The differences in amPEF, β agonist use, and risk of withdrawal due to asthma favoured the 1000 µg/day dose but were not statistically significant: odds ratio 1.21 (95% CI 0.44 to 3.35).
DISCUSSION
This meta-analysis has shown that, for all major clinical outcomes including exacerbations, most of the clinical efficacy of fluticasone is obtained with a dose of 200 µg/day in adults and adolescents with asthma. These findings are strongly consistent with our previous meta-analysis,1 indicating that the dose-response curve for fluticasone is relatively flat above doses of 200 µg/day, and that increasing the dose to 500 or 1000 µg/day will produce relatively little further improvement in clinical efficacy.
Limitations of the study
We have addressed many of the limitations of our previous meta-analysis with the inclusion of non-placebo controlled dose-response studies of fluticasone. This has allowed us to include two further studies of 895 patients2,3 and, in conjunction with forthcoming additional data on 602 patients from two of the previous studies, has given considerably greater power.4,7,10 This has enabled us to compare more accurately the efficacy between commonly prescribed doses and to establish the dose-response relationship of fluticasone at higher doses with more certainty.
We included in this meta-analysis seven studies of almost 2500 subjects which compared the efficacy of a dose of 200, 500 or 1000 µg/day. We primarily focused on dose comparisons with 200 µg/day as this was the dose where around 90% of the maximum clinical benefit was obtained in our previous meta-analysis.1 Together with the 200 µg/day dose, the 500 and 1000 µg/day doses represent the standard dose regimes available to physicians with the current inhalers. As with the previous meta-analysis, we included studies of at least 6 weeks’ duration based on time course studies which have indicated that most of the clinical improvement is achieved within the initial 6 week treatment period.7,11,12
We have made no adjustment for multiple comparisons in presenting our 95% confidence intervals, thereby increasing the chance of a type 1 error; however, this would not have influenced the interpretation of our findings. To reduce the effect of multiple comparisons between the different doses, we restricted the analysis to four dose comparisons for four major clinical outcome measures, with the 200 v ⩾500 µg/day dose comparison representing the primary analyses. Another consideration is that the comparisons between the different doses are not independent as the same studies contributed to the different dose comparisons. Furthermore, the different outcome variables are likely to be correlated, but they do provide different clinical measures by which the efficacy of fluticasone can be assessed. In this regard, we should emphasise that, although we have presented the results in the original units of measurement, this is for ease of understanding as the meta-analysis was carried out on the standardised mean difference.
Key findings
The different methods of analysis indicated that most of the efficacy of inhaled fluticasone was achieved at a dose of 200 µg/day for all major clinical outcome measures. An increase in the dose from 200 µg/day to ⩾500 µg/day provided a mean improvement of only 0.07 l and 5.9 l/min for FEV1 and amPEF, respectively. Even with the maximum change defined by the 95% confidence intervals, the improvements in FEV1 (0.14 l), amPEF (15.3 l/min), and β agonist use (−0.34 puffs/day) were less than those considered “clinically significant”, for which improvements of at least 0.234 l, 18.8 l/min, and−0.81 puffs/day have been proposed.13 This suggests that, for patients with moderate or severe asthma, increasing the dose of fluticasone above 200 µg/day is unlikely to result in clinically significant benefit. However, this interpretation is qualified by the considerable individual variability which has been observed in subjects with asthma.14–16 The lack of individual patient data prevented the investigation of intersubject variation in clinical response in this meta-analysis.
This dose-response relation is also strongly consistent with that of other inhaled corticosteroids given the established 2:1 potency ratio of fluticasone compared with budesonide and beclomethasone dipropionate.17,18 A recent meta-analysis of budesonide in adult asthma showed that most of the clinical benefit was achieved with a total daily dose of around 400 µg/day, and that the maximum achievable effect occurs with a dose of around 1000 µg/day.19 Furthermore, two large dose-response studies of CFC-beclomethasone dipropionate showed no statistically significant difference in clinical benefit between doses of 400 and 800 µg/day,3,20 consistent with these findings.
Three additional studies examined high doses of fluticasone but could not be included in the meta-analysis as there was no concordance with the dose comparisons of the studies which were included. The only study which has examined a dose greater than 1000 µg/day showed no statistically significant difference between 1000 and 2000 µg/day for all clinical outcome measures.21 The study of steroid naïve subjects with moderately severe asthma was unable to show clinically significant differences between a dose of 100 and 1000 µg/day fluticasone for all clinical outcome measures, bronchial response to methacholine, and markers of inflammation in induced sputum.22 In the study comparing the efficacy of incremental dose increases of fluticasone with beclomethasone dipropionate there was no further increase in FEV1 beyond that achieved with 100 μg/day fluticasone when the dose was increased to 2000 µg/day.14 Thus, there was consistency between the findings of our meta-analysis both with other dose-response studies of fluticasone not meeting our inclusion criteria and with dose-response studies of other inhaled corticosteroids.
Implications for clinical practice
While this meta-analysis did not include studies which examined the efficacy of long acting β agonists, the findings do explain in part why long acting β agonists provide greater therapeutic benefit than increasing doses of inhaled corticosteroids beyond the level of 200 µg/day of fluticasone or equivalent.23,24 This has been recognised by the recently published GINA and British guidelines which recommend the introduction of a long acting β agonist at step 3.25,26
We conclude that, in adolescents and adults with asthma, most of the therapeutic benefit of fluticasone is achieved with a total daily dose of 200 µg/day. Minimal further clinical benefit is achieved with higher doses for all major clinical outcomes including exacerbations. This conclusion is qualified by the recognition that there is considerable individual variability in the response to inhaled corticosteroids in asthma, which would suggest that some patients may obtain a greater benefit at higher doses, just as some may obtain maximum benefit at lower doses.
Acknowledgments
The authors acknowledge the assistance of Denise Fabian in the preparation of the manuscript. The Medical Research Institute of New Zealand, the Wellington School of Medicine & Health Sciences and P3 Research have received funding from GlaxoSmithKline, however GlaxoSmithKline had no role in the design, data analysis, or writing of the manuscript. No specific funding was sought for this study.
REFERENCES
Linked Articles
- airwaves