Article Text

Abstract
Background: Respiratory infection with Pseudomonas aeruginosa is very common in patients with cystic fibrosis (CF) but antimicrobial resistance rates of CF isolates across the UK are largely unknown.
Methods: The susceptibility of 417 CF patient isolates of P aeruginosa from 17 hospitals to six commonly prescribed antibiotics were examined. Isolates were tested by an agar break point dilution method and E-tests according to British Society of Antimicrobial Chemotherapy guidelines. Genotyping of isolates was performed by XbaI DNA macrorestriction and pulsed field gel electrophoresis.
Results: 38% of isolates were susceptible to all of the agents tested; almost half were resistant to gentamicin compared with ceftazidime (39%), piperacillin (32%), ciprofloxacin (30%), tobramycin (10%), and colistin (3%). Approximately 40% were resistant to two or more compounds with ceftazidime in combination with gentamicin, piperacillin or ciprofloxacin being the most common cross resistances. Resistance rates were generally similar to those reported recently from the USA and Germany. A selection of resistant isolates proved to be predominantly genotypically distinct by XbaI DNA macrorestriction but six pairs from three centres had similar genotypes.
Conclusions: The level of resistance to front line antipseudomonal agents, with the exception of colistin, is disturbingly high. The prudent use of antimicrobial drugs and closer monitoring of accumulation of resistant strain populations should be actively considered.
- cystic fibrosis
- Pseudomonas aeruginosa
- antimicrobial resistance
Statistics from Altmetric.com
The most common organism isolated from the sputum of patients with cystic fibrosis (CF) is Pseudomonas aeruginosa. Reports suggest that approximately 30% of children aged 2–5 and 80% of adults (aged 26–30 years) are colonised or infected with this organism.1 Its presence and persistence correlates with deterioration of lung function and clinical decline of patients and, despite treatment with antipseudomonal drugs, it is seldom eradicated from the lungs. Indeed, the use of antibiotic treatment for respiratory infections with P aeruginosa has been questioned, particularly with regard to short term clinical benefits when sputum colony counts may remain unchanged during or after intravenous treatment.2 Nevertheless, the bulk of clinical opinion supports the view that antibiotic treatment leads to improvement in lung function and improves survival of patients, particularly if aggressive treatment is begun on the first isolation of the organism.
P aeruginosa isolated from the natural environment and from non-CF patients is generally susceptible to the widely used antipseudomonal agents including ticarcillin, piperacillin, ceftazidime, imipenem, aztreonam, gentamicin, tobramycin, ciprofloxacin, and colomycin. Resistance rates for these isolates have changed little over the last two decades,3,4 and remain today around 12% for these agents.5 Prevalence data on resistance rates of P aeruginosa isolated from patients with CF have been reported from Italy6 and Denmark,7 but the rates across Great Britain are unknown. We performed a survey of P aeruginosa from selected hospitals throughout the UK to provide an indicator of the prevalence of resistance of CF isolates to six antimicrobial agents widely used for the treatment of Pseudomonas respiratory infections.
METHODS
Isolates of P aeruginosa
Isolates were requested from hospital microbiology laboratories serving CF patient populations. Senders were requested to avoid duplicate samples from the same patient but no information was sought regarding prior antimicrobial treatment. Four hundred and seventeen isolates were confirmed as P aeruginosa on the basis of oxidase and pyocyanin production or, for atypical isolates, by standard tests and API 20NE (Biomerieux).
Antimicrobial susceptibility tests
Isolates were subcultured on Kings A agar8 and those showing mixed colonial morphologies were tested as mixed morphotypes.9 Agar media (Isosensitest, Oxoid) were prepared for the following antibiotics at the low break point (a concentration defining the border between susceptibility and resistance to an antibiotic) recommended by the British Society of Antimicrobial Chemotherapy (BSAC)10: ceftazidime (8 μg/ml), ciprofloxacin (1 μg/ml), colistin (4 μg/ml), gentamicin (1 μg/ml), piperacillin (16 μg/ml), and tobramycin (1 μg/ml). Isolates were grown overnight in Trypticase Soy Broth (Oxoid) and diluted in sterile distilled water to give an inoculum of approximately 105 cfu per spot delivered with a multipoint applicator (Denley). Isolates that failed to grow on low break point concentrations were recorded as fully susceptible. The minimum inhibitory concentrations (MICs) for isolates that grew on these concentrations were determined with plastic support strips carrying a concentration gradient of antibiotic (Etests, Cambridge Diagnostic Services).
Selected isolates were examined after XbaI DNA macrorestriction analysis by pulsed field gel electrophoresis11 to assess the relatedness of their DNA profiles.
RESULTS
Four hundred and twenty eight isolates of P aeruginosa were received from 17 hospitals (9–68 isolates per centre); most were collected in September and October 2000. The isolates were submitted as a representative sample of the CF patient population attending a clinic in the study period. The centres varied from large regional specialists to provincial hospital clinics serving small numbers of CF patients. No attempt was made to select patients on the basis of early or chronic colonisation with P aeruginosa.
Table 1 shows that gentamicin was the least active antibiotic against the panel of isolates (47% resistant) followed by ceftazidime (39%), piperacillin (32%), ciprofloxacin (30%), tobramycin (10%), and colistin (3%). A high proportion of isolates displayed intermediate susceptibility to gentamicin (40%), tobramycin (35%), and ciprofloxacin (27%) and MICs ranged respectably above and below the high break point concentration for these agents.
Number (%) of isolates in stated category of susceptibility to antimicrobial agents at given concentrations (μg/ml)
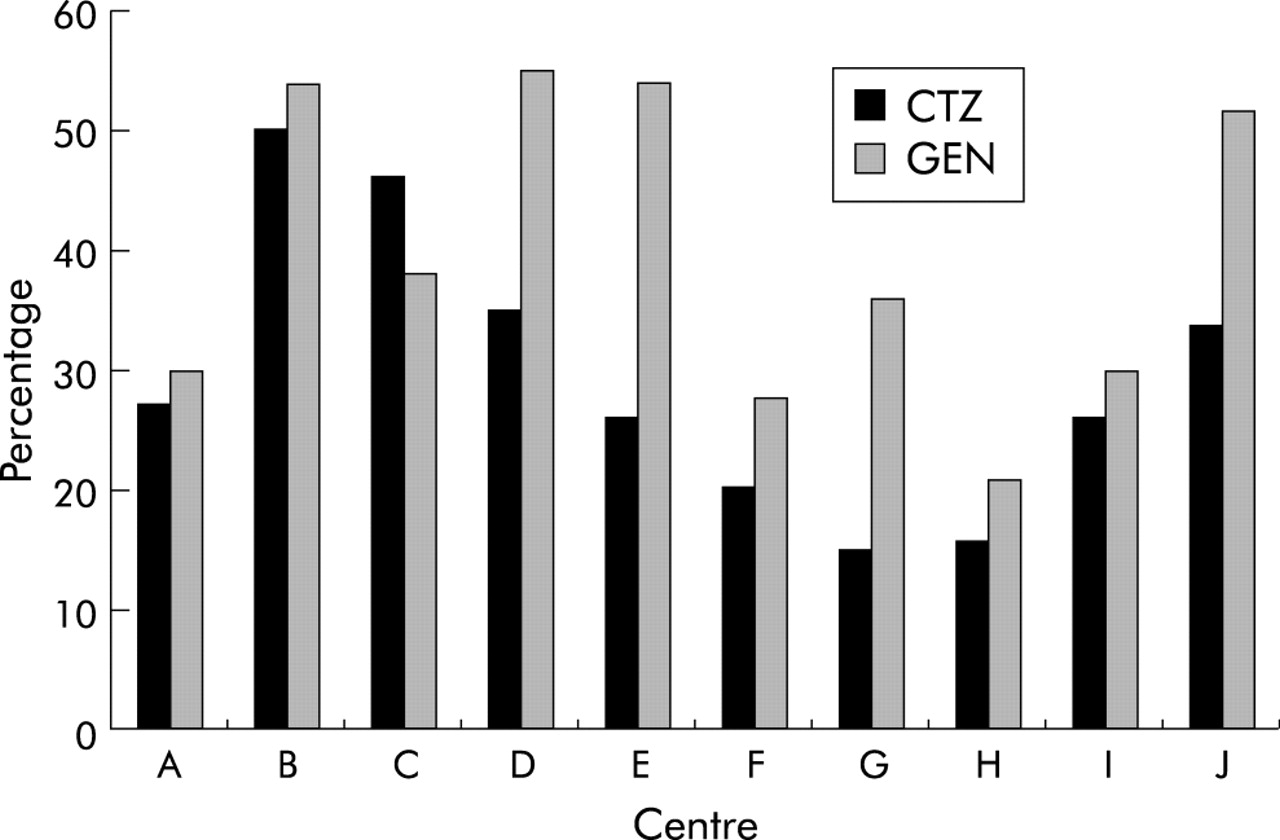
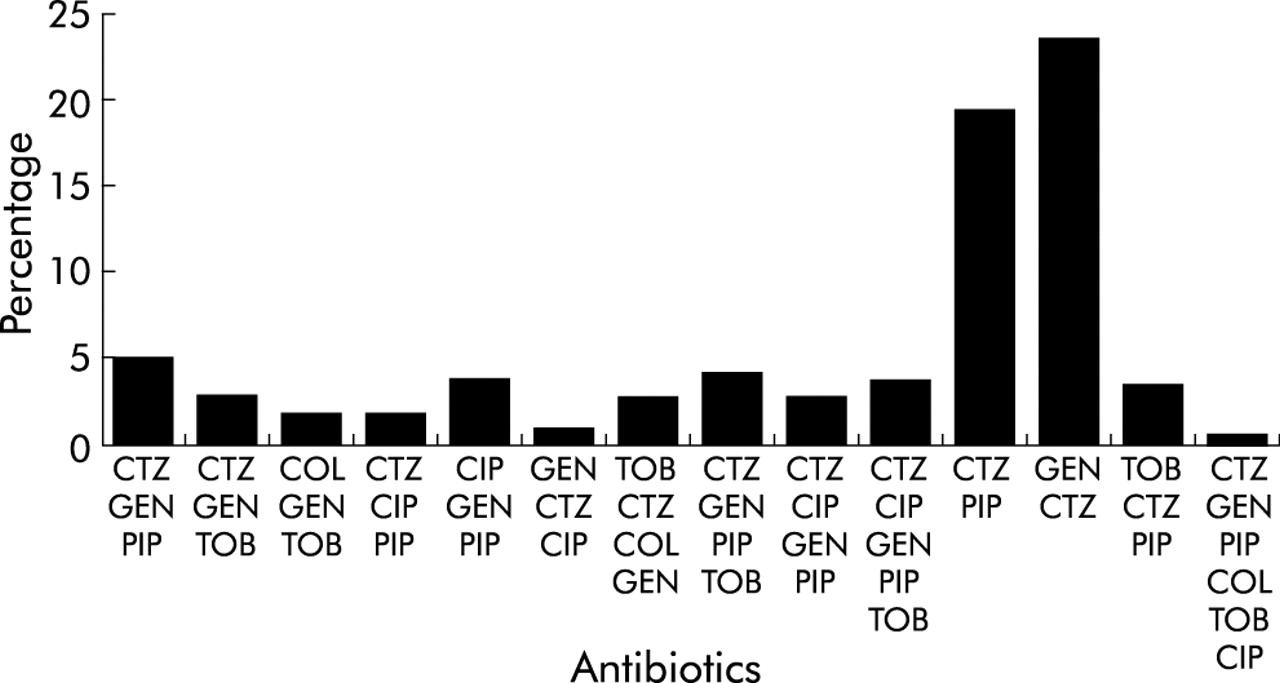
One hundred and fifty nine isolates (38%) were susceptible to all six antimicrobial agents, 87 (21%) were resistant to one, 72 (17%) were resistant to two, 45 (11%) were resistant to three, 32 (8%) were resistant to four, 19 (4.5%) were resistant to five, and three (0.7%) were resistant to all six agents tested; 87% exhibited resistance to three or fewer agents. Eighty three isolates that were resistant to ceftazidime were also resistant to gentamicin, and 91 gentamicin resistant isolates were resistant or had only intermediate susceptibility to tobramycin. Other notable cross resistances were ceftazidime/piperacillin (n=74) and ceftazidime/ciprofloxacin (n=41). Fourteen patterns of cross resistances were identified but only two (ceftazidime with piperacillin or gentamicin) accounted for more than 5% of all multiresistant isolates (fig 1). All colistin resistant isolates were gentamicin resistant and eight were resistant to four or five compounds, but two were susceptible to ceftazidime, three to ciprofloxacin, and four to tobramycin. Resistance rates for all antimicrobial drugs varied with CF centre, but fig 2 shows that, in the 10 centres which submitted the bulk of the isolates, ceftazidime and gentamicin resistance was widespread. For seven centres more than 25% of isolates were resistant to ceftazidime and only two centres had resistance rates for gentamicin under 30%.

Percentage distribution of antimicrobial resistance patterns of P aeruginosa isolates from patients with cystic fibrosis.
{kind=link}
{kind=link}
Prevalence of ceftazidime and gentamicin resistance of P aeruginosa from 10 cystic fibrosis centres.
Fifty five isolates exhibiting single or multiple resistances from various centres were selected as a representative panel for DNA analysis to assess the degree of relatedness among them. Most isolates were heterogeneous and unique for an individual, but six pairs from three centres had similar genotypes. Similar DNA profiles were given by four colistin resistant isolates. Two of these from a London CF centre were indistinguishable from a Cambridge patient isolate, perhaps reflecting transfer of patients between the centres. A second pair of colistin resistant isolates from patients in a Belfast hospital had a DNA pattern closely related to that of an isolate from a different Belfast centre.
DISCUSSION
Knowledge of the susceptibility of P aeruginosa to antimicrobial agents used for treatment not only serves as a guide to treatment for individual CF patients, but it is also valuable for identifying the prevalence of resistant strains within and between different treatment centres, given the mobility of some patients. The survey reported here showed that rates of insusceptibility and frank resistance of P aeruginosa isolated from patients with CF are disturbingly high in the UK. This confirms a recent nationwide survey of 2194 P aeruginosa isolates which found that 98 isolates from CF patients were among the most resistant.5 In particular, very high levels of resistance to two mainstay drugs (ceftazidime and gentamicin) were evident, leading one to question their empirical use in this patient group. The rate of gentamicin resistance (47%) is comparable with USA data (TSN Database USA; Focus Technologies, VA, USA) for the same antibiotic (41%), but the resistance to ceftazidime here (40%) is twice that reported in the USA database.12 Resistance to ciprofloxacin in the UK CF population is similar to that in the USA.
However, the data obtained here appear to contrast sharply with a recent report from Freiburg, Germany13 which used National Committee for Clinical Laboratory Standards (NCCLS) break points14 (German DIN break point for colistin15) and found that 84% of 385 isolates from 57 patients were susceptible to ceftazidime (MIC ⩽8 μg/ml) and piperacillin (MIC ⩽64 μg/ml), and 42% and 43% were susceptible to colistin (MIC ⩽0.5 μg/ml) and tobramycin (MIC ⩽4 μg/ml), respectively. Owing to the differences in break point values between BSAC and NCCLS, these data are not directly comparable with those reported here for most of the compounds except for ceftazidime. Indeed, if one applies the BSAC break point values in table 1 to the isolates in the Freiburg study, 92% would be susceptible to colistin with 33% resistant to piperacillin and 36% resistant to tobramycin, values which are more in line with the present study.
Cross resistance was widespread with approximately 40% of CF isolates resistant to two or more antibiotics, most often ceftazidime and gentamicin or ceftazidime and piperacillin. This may be explained by repeated exposure of organisms to sublethal concentrations of antibiotics in the lung leading to the accumulation of multiple mutations over time. These mutations affect the efflux mechanism which pumps β-lactams and other compounds except aminoglycosides out of the bacterial cell and, combined with impermeability to aminoglycosides, leads to phenotypic resistance.12 Colistin was clearly the most active antimicrobial tested, with 97% of isolates susceptible to ⩽4 μg/ml. Resistance is rare, partly because the compound self-promotes its penetration of the cell envelope and causes irreversible disruption of the cytoplasmic membrane. Also, P aeruginosa appears unable readily to modify the lipid A target of its lipopolysaccharide to prevent binding of colistin.16 It is noteworthy that, unlike the other agents tested, colistin is used almost exclusively in the CF population.
We chose to use a combination of screening susceptibility at the low BSAC break point, confirming the MIC of insusceptible strains by E-tests. Furthermore, we preferred to mix colonial morphotypes to avoid the problem of selecting all discrete colony forms which may give highly variable MIC results.13,17 Marley et al18 reported good agreement between the results of E-tests and agar dilution susceptibility tests for the determination of the MIC of antibiotics for P aeruginosa isolates from subjects with CF. The mean E-test MIC was 0.82 log2 lower than that obtained by agar dilution and, of 400 comparisons, only three major discrepancies in susceptibility between the two methods were found. Two studies of note have addressed the question of mixed morphotype susceptibility testing. Morlin et al9 attempted to correlate the MIC of mixed colonies with the MIC of the most resistant morphotypes tested separately and concluded that the MIC of the mixture correctly predicted the highest MICs of resistance for isolated colonies. The second study19 combined colonies direct from the primary isolation agar or selected pure colonies and mixed them together before testing. They found that agreement with morphotypes tested individually against the combination or mixed pure cultures was in excess of 85% and 92%, respectively.
Although most of the isolates were distinct genotypes, suggesting the absence of clonal expansion of specific strains, DNA profiling identified a few pairs of related antibiotic resistant isolates. However, as no patient identifiers were submitted with the isolates, this may have been due to sharing of strains by siblings or close patient contacts. No isolates from the recent reports of cross infection with multiresistant strains of P aeruginosa20,21 were included in this survey and no evidence was found to indicate the wide existence of a cross infection problem due to antimicrobial resistant strains. Further genotyping studies of larger samples of isolates, both susceptible and resistant, from different centres are therefore warranted.
In conclusion, this snapshot survey has revealed a high prevalence of resistance to commonly used antimicrobial drugs of P aeruginosa from patients with CF in a number of centres across the UK. Restriction of the empirical use of some agents and closer monitoring of the rates to identify accumulation of resistant strains within clinics may prove beneficial and inform prescribing policies.
Acknowledgments
The authors thank Dr Ian Bowler, Dr Mary Crowe, Dr Judith Foweraker, Dr Harry Gaya, Professor John Govan, Dr John Gray, Dr Elizabeth Price, Dr Grace Smith, Dr James Soothill, Dr Robert Spencer, and other microbiologists who sent isolates for the survey, and Dr Caroline Henwood and Dr David Livermore (CPHL) for access to additional strains and for constructive discussion. We also thank Dr Christopher Sheldon for his comments on the manuscript. The study was supported by a grant from Forest Laboratories Europe.