Article Text

Abstract
Background: Patients with asthma are interested in the use of breathing exercises but their role is uncertain. The effects of the Buteyko breathing technique, a device which mimics pranayama (a yoga breathing technique), and a dummy pranayama device on bronchial responsiveness and symptoms were compared over 6 months in a parallel group study.
Methods: Ninety patients with asthma taking an inhaled corticosteroid were randomised after a 2 week run in period to Eucapnic Buteyko breathing, use of a Pink City Lung Exerciser (PCLE) to mimic pranayama, or a PCLE placebo device. Subjects practised the techniques at home twice daily for 6 months followed by an optional steroid reduction phase. Primary outcome measures were symptom scores and change in the dose of methacholine provoking a 20% fall in FEV1 (PD20) during the first 6 months.
Results: Sixty nine patients (78%) completed the study. There was no significant difference in PD20 between the three groups at 3 or 6 months. Symptoms remained relatively stable in the PCLE and placebo groups but were reduced in the Buteyko group. Median change in symptom scores at 6 months was 0 (interquartile range −1 to 1) in the placebo group, −1 (−2 to 0.75) in the PCLE group, and −3 (−4 to 0) in the Buteyko group (p=0.003 for difference between groups). Bronchodilator use was reduced in the Buteyko group by two puffs/day at 6 months; there was no change in the other two groups (p=0.005). No difference was seen between the groups in FEV1, exacerbations, or ability to reduce inhaled corticosteroids.
Conclusion: The Buteyko breathing technique can improve symptoms and reduce bronchodilator use but does not appear to change bronchial responsiveness or lung function in patients with asthma. No benefit was shown for the Pink City Lung Exerciser.
- Buteyko breathing technique
- complementary medicine
- yoga
- asthma
Statistics from Altmetric.com
There is interest in the use of complementary treatment for asthma and a third of respondents in a recent asthma survey had tried one or more breathing techniques to relieve symptoms.1 However, few controlled studies have been undertaken to determine the effectiveness of these approaches. We have previously studied two components of pranayama,2 the yoga breathing exercise, by asking subjects with asthma to breathe twice a day through a cylinder with an expiratory resistance (the Pink City Lung Exerciser (PCLE)) designed to reduce breathing frequency and increase the duration of expiration. There was a small reduction in airway responsiveness to histamine after using the PCLE for 2 weeks compared with a placebo device without a resistance.
A BBC television programme in 1998 generated considerable interest in the Buteyko breathing technique. The technique, developed in Russia by Konstantin Buteyko, is based on the belief that asthma is caused by hyperventilation and hypocapnia and can be cured in most patients by using special techniques to reduce minute ventilation.3 The effects on asthma control in two small controlled studies in Australia were modest, however.4,5 The Eucapnic Buteyko method is an adaptation of the Russian technique which was first introduced in Australia but is now used worldwide. It includes the same focus on ventilation control but the approach has been designed to suit patients in western countries.
We compared the effect of the Buteyko technique, pranayama exercises using the PCLE, and the PCLE placebo device in subjects with asthma. Symptom scores and bronchial responsiveness to methacholine were the primary outcome measures.
METHODS
Subjects
Non-smoking volunteers aged 18–70 with stable asthma but no other important illness were recruited between September 1999 and November 2000 from our asthma volunteer database and from posters and newspaper advertisements. Inclusion criteria included: taking an inhaled short acting β2 agonist at least twice a week and regular inhaled corticosteroids with no change in dose in the preceding 4 weeks; pre-bronchodilator forced expiratory volume in 1 second (FEV1) of at least 50% predicted and a 10% increase following 400 μg inhaled salbutamol; a provocative dose of methacholine causing a 20% fall in FEV1 (PD20) of 10.24 μmol or less; and a mean daily symptom score of one or more during the run in period. Subjects taking treatment other than sodium cromoglycate (one subject) were excluded.
Written consent was obtained from all subjects and Nottingham City Hospital ethics committee approved the study.
Measurements
FEV1 and forced vital capacity (FVC) were measured with a dry bellows spirometer (Vitalograph, Buckingham, UK) as the highest of two successive readings within 100 ml. Methacholine PD20 was measured by a breath activated dosimeter (MEFAR, Brescia, Italy). Nebulisers had an output of 10 (0.5) μl at 1 second and calibration was checked every 6 months. Subjects inhaled three puffs of saline followed by doubling doses of methacholine (dose range 0.02–42 μmol) until FEV1 had fallen by 20% from the post-saline value. FEV1 was measured 2 minutes after each dose and PD20 by linear interpolation on a log-dose response plot.
Subjects kept diary cards to record breathing exercises, medication use, and asthma symptom severity during the day and night (both 0–5), plus activity limitation due to asthma (0–3; maximum combined score 13). Quality of life was assessed using the SF-366 and Asthma Quality of Life7 questionnaires.
Protocol
The study had a parallel group design with participants randomised to be taught the Eucapnic Buteyko technique or use of the PCLE or PCLE placebo device. Subjects underwent training (see below) and were asked to perform the exercises for at least 15 minutes twice a day throughout the study. A card sent 2 weeks later gave further encouragement. Subjects were followed for 6 months with an optional extension during which inhaled steroid reduction was attempted.
Bronchodilator reversibility and methacholine PD20 were measured on separate screening visits. Subjects fulfilling the entry criteria entered a 2 week run in period. Eligible subjects were then allocated to one of the three treatment groups using the next available number from computer generated numbers, randomised in blocks of six, and using sealed envelopes prepared independently. To ensure sufficient numbers for the Buteyko sessions, randomisation was skewed towards the Buteyko group except for the last 12 patients who were randomised between the two PCLE groups. Subjects were only given details of their treatment. They attended the clinic after 1, 3, 5, 9, 13, and 26 weeks at the same time of day after withholding β2 agonists for 6 hours. Subjects were seen first by the training coordinator who dealt with queries about the breathing exercises. They then saw the clinical assessor who assessed asthma control and measured lung function, including methacholine PD20 at 13 and 26 weeks. The assessor was not told which breathing technique subjects were using and subjects were asked not to mention it. Subjects completed the two quality of life questionnaires before randomisation and after 13 and 26 weeks, together with a postal feedback questionnaire at least 6 weeks after completing the study.
Subjects were asked to keep their dose of inhaled steroid constant throughout the first 6 months unless they had an asthma exacerbation. This was defined as a 20% fall in FEV1 or a 50% increase in β2 agonist use and >6 puffs on two of three successive days compared with the randomisation visit/run in period, or worsening asthma needing urgent medical care or rescue medication on two of three successive nights.
Steroid reduction phase
Steroid reduction was attempted 6 months after randomisation for subjects with stable asthma who agreed to take part. The dose was reduced by 25% every 3 weeks at a clinic visit until either the inhaled steroid had been discontinued, an asthma exacerbation occurred, or the doctor or subject felt that asthma control had deteriorated to an extent that merited reversal of steroid reduction.
Training
Training was given in small groups: numbers ranged from 3–8 in the Buteyko training sessions, 2–5 in the PCLE group, and 1–5 in the control group.
Buteyko group
The Eucapnic Buteyko technique, a western modification of the Russian Buteyko technique, was taught by a certified practitioner in five 2 hour sessions over a weekend or successive evenings. Subjects were taught exercises to reduce the frequency and depth of breathing and, as part of the technique, were asked to record pulse and breath holding time twice daily in a diary. They were instructed to use the breathing technique twice daily and to relieve asthma symptoms, and only to use their bronchodilator if that failed. Subjects were also asked to tape their mouth at night with hypoallergenic tape (Micropore) to prevent mouth breathing and were advised to avoid factors such as stress, exercise accompanied by deep breathing, oversleeping, and certain foods (for example, highly processed food and additives). Two weeks after the training the subjects were telephoned by the Buteyko practitioner to give encouragement and answer queries. Subjects could contact the practitioner for further advice if they felt it necessary.
Pink City Lung Exerciser (PCLE) group
Training took place in a single session. The PCLE consists of a mouthpiece attached to a disc containing six apertures 2–5 mm in diameter with one-way valves which halve the cross sectional area during expiration and thus impose a 1:2 ratio on the duration of inspiration compared with expiration.2 With the device set to the largest aperture, subjects were asked to breathe in and out from residual volume to total lung capacity at a rate at which they felt no resistance to breathing and could feel no cheek movement. If, after a week, they could do the exercises without feeling breathless, they were encouraged to decrease the aperture size gradually to reduce respiratory rate. They were told to use their β2 agonist only for relief of symptoms.
Control group
Training was identical to that for the PCLE group. The placebo device had an identical appearance to the PCLE but the apertures had no valve and a leak ensured no resistance to breathing.
Outcome measures
The primary efficacy variables were symptom scores and methacholine PD20. Secondary outcomes included FEV1, bronchodilator use, asthma exacerbation rates, quality of life assessments, and reduction in inhaled corticosteroid dose.
With 30 subjects in each group there was 90% power to detect a difference between treatments in change from baseline methacholine PD20 of 1.5 doubling doses using an α of 0.05 according to previous data.2,8
Analysis of data
All available data for the 89 patients who underwent training were analysed. When data were unavailable they were treated as missing. Codes were revealed after all data had been reviewed and entered. PD20 values were log transformed for analysis and expressed as change from the end of the run in period, as were FEV1, symptoms, and quality of life measures. Change in PD20 and FEV1 were compared between groups using analysis of variance, adjusting for baseline values as a covariate when there were baseline differences. The Kruskal-Wallis test was used to compare changes from baseline for steroid reduction, quality of life measures, median symptom scores, and bronchodilator use (for 7 days before each visit). We also carried out an analysis of the primary outcome measures, substituting missing data with the last recorded value before subjects withdrew. The results were virtually identical to those seen in our main analysis and are not presented.
RESULTS
Of 178 patients screened, 136 fulfilled the entry criteria, 90 were randomised, 89 underwent training, and 69 completed the 6 month study (fig 1). Data from one subject who became pregnant were excluded from the analysis before breaking the randomisation code. The number of participants failing to complete and the reasons given were similar in the three groups. Baseline characteristics were also similar except that those receiving the Buteyko training were younger, were taking slightly more inhaled corticosteroid, and had a lower PD20 methacholine (table 1). (Baseline quality of life data (table 1b) are available online at www.thoraxjnl.com/supplemental.)
Baseline characteristics of study patients

Summary of patients entered, randomised and withdrawn from trial.
Primary outcome measures
There was little change in PD20 from baseline during the study and no significant difference between the groups at 3 and 6 months (table 2).
Change from baseline PD20 methacholine at 3 and 6 months
Symptoms remained relatively stable in the PCLE and placebo groups but were reduced in the Buteyko group (fig 2). The median (interquartile range, IQR) change in daily symptom scores at 6 months was 0 (−1 to 1) in the placebo group, −1 (−2 to 0.75) in the PCLE group, and −3 (−4 to 0) in the Buteyko group; the difference between the three groups was significant (p=0.003).
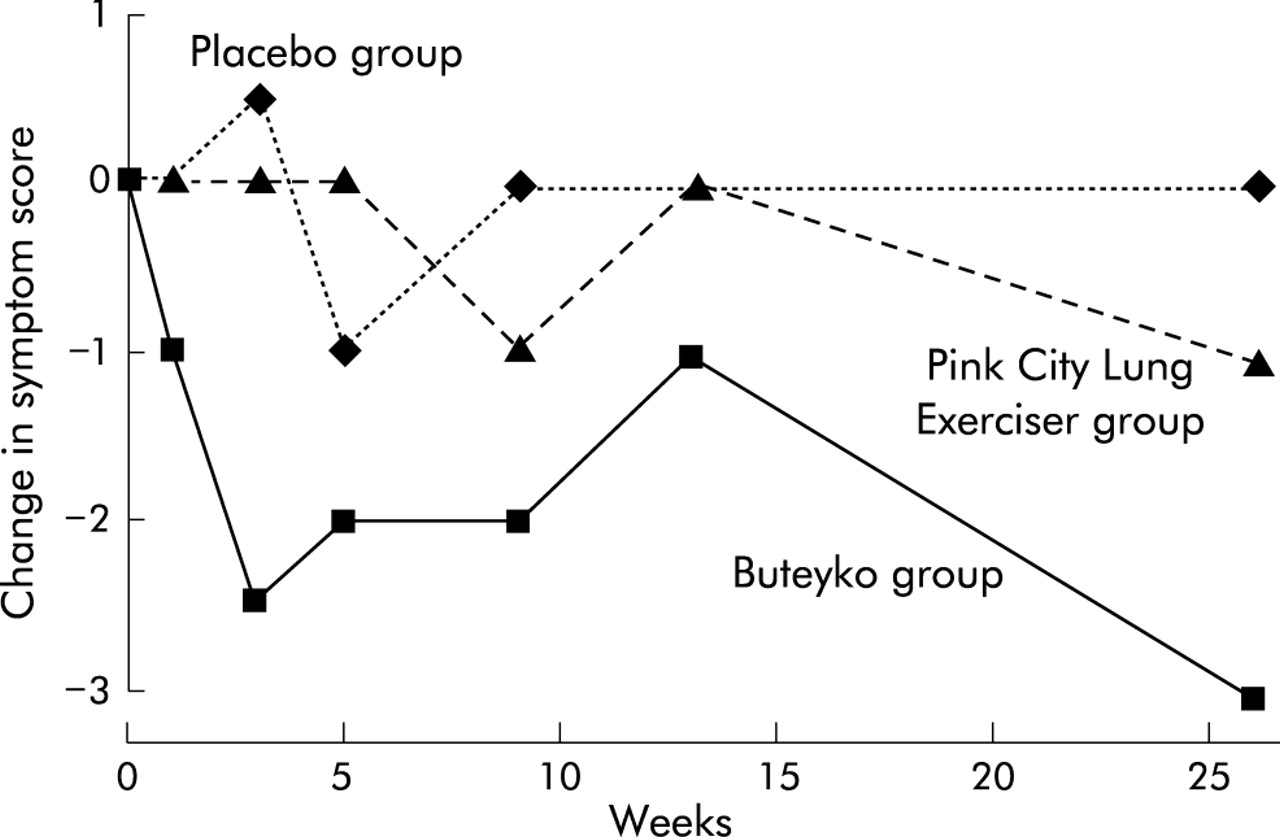
Median change in symptom scores during the 6 month study.
Secondary outcome measures
The use of β2 agonists was reduced in the Buteyko group throughout the study and unchanged in the other two groups: median (IQR) change at 6 months 0 (−2 to 0) puffs/day in the placebo group, 0 (−2 to 0) puffs/day in the PCLE group, and −2 (−4 to 0) puffs/day in the Buteyko group (difference between groups significant, p=0.005). There was no difference in change in FEV1, number of asthma exacerbations, days requiring an increase in inhaled corticosteroid dose or courses of prednisolone between the groups during the 6 month study period (table 3). Changes in quality of life, as measured by the SF-36 questionnaire, did not differ significantly apart from one of the eight dimensions (“Role limitation due to physical problems”) which improved more in the Buteyko group at both 3 and 6 months (both p<0.01). None of the Asthma Quality of Life questionnaire domains had changed significantly at 6 months (see table 4 online at www.thoraxjnl.com/supplemental for details)
Secondary end points over the 6 month study period
Steroid reduction phase
Of 69 subjects who completed the study, nine were unwilling to attempt steroid reduction leaving 60 in the analysis with similar numbers in each group (fig 1). The extent to which subjects could reduce their inhaled steroid did not differ significantly between groups (p=0.7; table 3, fig 3)

{kind=link}
{kind=link}
{kind=link}
Number of subjects able to reduce inhaled corticosteroids in the steroid reduction phase.
Feedback from subjects
At the end of the study more subjects in the Buteyko group thought that they had definitely or probably received active treatment (15 + 8 of 26 respondents) than subjects in the PCLE group (4 + 9 of 25) or the placebo PCLE group (4 + 10 of 25) (p<0.001).
There were 72 replies (81% response rate) to the postal questionnaire. Most subjects said they had been compliant with the breathing exercises during the study (see table 5 online at www.thoraxjnl.com/supplemental). Of 23 responders in the Buteyko group, 22 said they had practised the exercises twice a day while 14 in the PCLE group and 17 in the placebo PCLE group said they had practised for at least 10 minutes a day. Four subjects in the Buteyko group were unable to tape their mouth at night but 14 said they did it for at least five nights a week and eight did it every night. After completing the study 16 subjects in the Buteyko group had continued the exercises, at least on an occasional basis, compared with 12 and 9 in the PCLE and placebo PCLE groups.
DISCUSSION
In this randomised controlled trial subjects taught the Eucapnic Buteyko technique had reduced asthma symptoms and bronchodilator use compared with the other two groups but there was no difference in bronchial responsiveness or FEV1. No difference was seen between the PCLE and PCLE placebo device for any outcome measure.
A television programme in 1998 in the UK generated considerable media and patient interest in the Buteyko technique. The course used in this study, the Eucapnic Buteyko technique, was available to the general public. It includes breathing exercises, taping the mouth at night, strongly discouraging the use of β2 agonists except in emergencies, advice on lifestyle, and strong practitioner encouragement. Yoga breathing exercises (pranayama) involves mental concentration to cause a reduction in breathing frequency, a 1:2 ratio of inspiration to expiration, and a pause at the end of inspiration and expiration. The expiratory resistance in the PCLE imposes a reduction in breathing frequency and expiratory flow.
Over 90% of 100 000 patients who completed the Buteyko course in Russia are said to need no further asthma medication and a similar success rate has been claimed for 8000 patients in Australia.9 The results of the two controlled studies from Australia in 39 and 36 subjects are more modest.4,5 In one, which focused on patients taking high doses of short acting β2 agonists (median >800 μg salbutamol daily), Buteyko training resulted in a large reduction in β2 agonist use which correlated with a reduction in minute ventilation compared with the control group. There was a non-significant trend to reduced inhaled steroid use and better quality of life, but no change in lung function or end tidal CO2 pressure. In the second study subjects taught Buteyko breathing exercises by video had a reduction in bronchodilator use and improvement in quality of life but no change in peak flow rate.5
Our study was larger and longer than the previous studies, and looked for the first time at bronchial responsiveness and asthma exacerbations. Although only averaging two puffs of β2 agonist a day on entering the study, subjects in the Buteyko group were able to reduce their β2 agonist use. Despite this, symptoms were reduced and there was no increase in exacerbations or use of inhaled corticosteroids. There was also an improvement in one of the eight dimensions of the SF-36 questionnaire (“Role limitation due to physical problems”). The changes in asthma quality of life and reduction in inhaled corticosteroids favoured Buteyko, but the differences were small and non-significant. There was no change in bronchial responsiveness or FEV1 despite clear potential for improvement.
These findings support the suggestion10 that the Buteyko technique may help patients adapt to their asthma and feel more in control of their treatment. It does not appear to alter the underlying disease process, however. Since subjects in the Buteyko group were strongly discouraged from using β2 agonists, the extent to which the reduction in β2 agonist use was a cause or a consequence of a reduction in symptoms is uncertain.
Our findings should be generalisable to patients who are interested in breathing exercises. The study is not able, however, to determine which subjects benefited from the Buteyko technique. Patients with asthma who also have dysfunctional breathing11,12 or who take more β2 agonists than they need13 may obtain most benefit, but further studies are needed to determine this.
In a previous comparison of the PCLE and placebo device in subjects with mild asthma, the active PCLE caused a small reduction in bronchial responsiveness.2 We were unable to confirm this in the current study, perhaps because of differences in the populations studied or study duration. The PCLE involves only one aspect of yoga, and a 4 month trial of Sahaja yoga in asthma14 showed benefit over a control intervention.
The need for controlled studies of complementary medicine is widely recognised with recent endorsement from a presidential commission in the US15 and a House of Lords Select Committee in the UK.16 Such studies are difficult to carry out, however, and our study raises several issues. The choice of a suitable control is one difficulty; subjects in the Buteyko group were more likely to believe they were receiving active treatment resulting, perhaps, in greater psychological benefit. On the other hand, use of the placebo PCLE as a control involved subjects in some change from usual practice since they were asked to focus on breathing for 30 minutes a day. Some subjects may have benefited from this since nine continued to use the device after the study ended, despite being told it was the placebo device. Any benefit from the placebo device would reduce the ability of the study to detect an effect from the other interventions. Maintaining blindness is another potential problem. Asking subjects not to mention the technique to the assessor worked reasonably well, although one mentioned Buteyko and an occasional subject mentioned a device, but which device was not clear. A formal study may also interfere with usual practice. A previous study4 was criticised because the Buteyko group received more follow up visits than the control group so we only included one follow up telephone discussion with the Buteyko practitioner. Most subjects were happy with this but nine would have liked more contact.
A further problem is that advice from complementary medicine practitioners may differ from conventional advice and a few subjects found this difficult, particularly knowing whether to use a β2 agonist or the Buteyko technique to control worsening asthma. Finally, the success or failure of a treatment such as Buteyko relies heavily on the patient/practitioner relationship. The training sessions are long and patients need to be highly motivated to commit themselves fully to the training and need to practise daily. The success rate in a formal trial might therefore be less than that seen in everyday practice, since subjects did not specifically choose the Buteyko course and, because they were not paying, they may have felt less committed to seeing it through. Furthermore, subjects who may be considered unsuitable by Buteyko practitioners were not necessarily excluded by our entry criteria.
Despite these problems, which are inherent in all studies of complementary medicine, and the differences in study design between our study and the previous controlled studies, our findings are broadly similar. They suggest that the Buteyko technique produces some benefit by reducing symptoms and use of bronchodilators and it may improve some aspects of quality of life. None of the studies found any improvement in airway calibre, however, and we found no effect on bronchial responsiveness or asthma exacerbations. The Buteyko technique may be worth trying in patients who are sympathetic to the ethos and are willing to commit the time required.
Acknowledgments
The study was supported by The National Asthma Campaign. The authors thank Susan Mitchell and “Lifesource” for running the Buteyko classes and Dr Virendra Singh for supplying the Pink City Lung Exercisers and placebo devices. The authors are grateful to Tim Harrison for reviewing the manuscript and for providing medical cover and advice, along with Kate Phillips, and to Marie Cooper for help with the data entry.
REFERENCES
Supplementary materials
. Web-only Tables
The tables are available as downloadable PDFs (printer friendly files).If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [View PDF] - Mean (SD) quality of life baseline characteristics
- [View PDF] - Change in quality of life scores
- [View PDF] - Postal questionnaire sent to subjects at least 6 weeks after completing the study
Linked Articles
- Airwaves