Article Text

Abstract
Fibrinolytic enzymes, particularly streptokinase, are now widely used to treat empyema thoracis. Recent in vitro evidence suggests that streptokinase has no effect on pus viscosity but that deoxyribonuclease (DNase) reduces the viscosity of pus. We report the first use of human recombinant DNase given intrapleurally to treat an empyema which had not resolved after standard treatment with streptokinase.
- empyema thoracis
- deoxyribonuclease
- streptokinase
Statistics from Altmetric.com
Empyema thoracic is a serious condition with a significant mortality. The importance of drainage of the pleural space was recognised by Hippocrates.1 Simple percutaneous tube drainage may fail in over 50% of patients, most of whom will then require surgical procedures. The overall mortality of pleura empyema is 10%.2 The use of intrapleural enzymes to aid drainage was first described in 19493 using a mixture of streptokinase and streptococcal DNase. In recent years purified streptokinase has come into widespread use, but recent evidence4 suggests that it has no effect on pus viscosity but that DNase dramatically reduces pus viscosity and may be useful in treatment. We report the successful use of human recombinant DNase to treat empyema thoracis after failure of streptokinase therapy.
CASE REPORT
An 83 year white woman was admitted with a 4 day history of fevers and rigours with breathlessness and right sided pleurisy. On examination she was pyrexial and toxic with arterial desaturation (Spo2 89%) and signs of a right pleural effusion. She was in atrial fibrillation with a peripheral blood neutrophilia and mild renal impairment (white cell count 14.8 × 109/l, creatinine 0.24 mmol/1).
The patient was treated with intravenous erythromycin, ceftriaxone, and metronidazole. Blood cultures grew Streptococcus pneumoniae sensitive to penicillin and treatment was changed to roxithromycin orally and benzyl penicillin intravenously. Two days after admission the pleural effusion had increased and 900 ml of purulent fluid were aspirated. This had a protein content of 35 g/l, glucose <0.3 mmol/l, and lactate dehydrogenase (LDH) of 9412 units/l. Gram stain showed Gram positive cocci. Two days later the fluid had re-accumulated and an intercostal catheter was inserted. After 1 week of continuous drainage yielding 1.4 l the patient remained systemically unwell and toxic and the chest radiograph had not improved. The patient was then referred to the thoracic team.
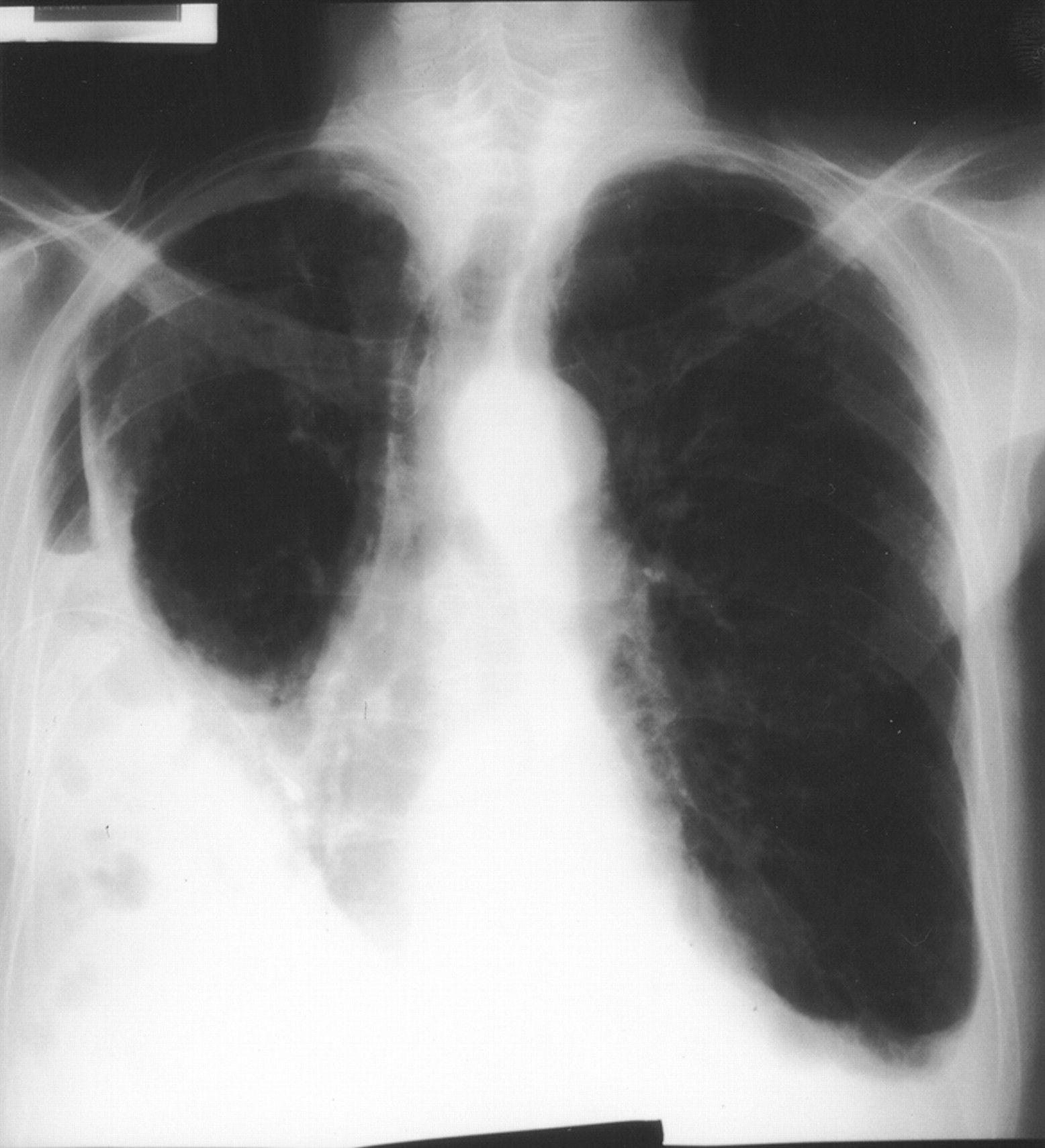
A second intercostal catheter was inserted lower down into the main body of the empyema and intrapleural streptokinase was given for 3 days at a daily dose of 250 000 units. There was further drainage of 330 ml on day 1, 110 ml on day 2, and 100 ml on day 3. At the end of this time the chest radiograph had improved, but there was still a substantial pleural collection and the patient remained unwell (fig 1).

Posteroanterior radiograph of patient following 3 days of treatment with intrapleural streptokinase.
The patient adamantly refused to consider thoracic surgical intervention and, after explanation of the experimental nature of the treatment, agreed to be treated with intrapleural human recombinant DNase (dornase alfa, Pulmozyme).
Five mg of dornase alfa and 50 ml of normal saline were thus instilled into the pleural space daily for 3 consecutive days with clamping of the tube for 4 hours after instillation. Suction at 20 cm H2O was applied as it had been throughout the period of intercostal drainage. On day 1 330 ml of thin pus drained, on day 2 a further 170 ml, and on day 3 300 ml drained with considerable improvement both in the radiograph (fig 2) and in the patient’s systemic symptoms. Her appetite and energy levels improved and she became afebrile. The chest drains were removed on day 25 of her admission.

{kind=link}
{kind=link}
Posteroanterior radiograph of patient after 3 days of treatment with intrapleural DNase showing marked reduction in the size of the right sided empyema.
The patient was discharged on oral clindamycin. Her chest radiograph 1 month after discharge had further improved. Antibiotics were discontinued and she remains well 3 years later with no systemic symptoms, no respiratory impairment, and a virtually normal chest radiograph.
DISCUSSION
Successful treatment of pleural empyema depends on adequate drainage of the pleural space. The two factors which seem likely to prevent successful drainage by intercostal tube are loculation of the fluid by formation of fibrinous strands within it and increasing viscosity and adherence of the pus to the pleural surfaces, possibly preventing lung expansion by coating the visceral pleura. It is over half a century since Tillett and Sherry3 demonstrated the beneficial effects of intrapleural enzyme treatment using fairly crude streptococcal extracts. A more refined version of the extracts was later marketed by Lederle & Co as Varidase and continued to be used, particularly in the UK, to treat empyema. Because of some worries regarding the antigenicity of this fairly crude preparation, there has been much interest in the use of highly purified streptokinase in this context. Results of controlled studies of this treatment have been mixed,5,6 and it was our clinical impression that the purified preparation was much less effective than the older preparation which contains a small proportion of streptococcal DNase. Subsequent studies showed that streptokinase alone has no effect on pus viscosity but that the inclusion of either streptococcal or human recombinant DNase reduced viscosity markedly.4 Similar results were obtained in an animal model using Varidase.7 DNase acts by depolymerisation of polymerised doexyribonucleoproteins and is a ubiquitous enzyme which will act on DNA of bacterial as well as mammalian origin, though the DNA in empyema pus is probably mainly derived from leucocytes.
In the case reported here fibrinolytic therapy failed and the patient was refusing surgical intervention. We believe this is the first reported use of human recombinant DNase to treat empyema thoracis and that the improvement in the patient’s condition was related to the reduction in viscosity and adherence of the pus by the DNase which thus aided drainage of the pleural cavity.
Human recombinant DNase seems to be extremely safe when given by nebulisation as it is in the treatment of cystic fibrosis. The experience with fibrinolytic agents suggests little absorption of enzymes from the pleural cavity when used to treat empyema.5 There were certainly no adverse reactions to the DNase used in this case. We would suggest that this clinical anecdote together with the in vitro evidence would support the inclusion of human recombinant DNase in future trials of intrapleural enzyme therapy in the treatment of empyema.
Footnotes
-
The authors received no financial support for this study.