Article Text

Abstract
Background: The synthetic vasoactive intestinal peptide (VIP) analogue Ro 25-1553 is a selective VIP-PACAP type 2 (VPAC2) receptor agonist that causes a bronchodilatory effect in guinea pigs in vivo. The effect of Ro 25-1553 given by inhalation to patients with asthma was studied and compared with that of a long acting β2 adrenoceptor agonist.
Methods: Twenty four patients with moderate stable asthma participated in a double blind, randomised, placebo controlled, crossover study. The primary variable was bronchodilatory effect (increase in forced expiratory volume in 1 second, FEV1) after inhalation of Ro 25-1553 (100 μg or 600 μg) and formoterol (4.5 μg), respectively. Putative side effects were characterised by monitoring sitting blood pressure, serum potassium, electrocardiography and echocardiography.
Results: Inhalation of 600 μg Ro 25-1553 caused a rapid bronchodilatory effect (geometric mean increase in FEV1 compared with placebo) within 3 minutes of 6% (95% CI 4 to 9), as did inhalation of formoterol (8% (95% CI 5 to 10)). The corresponding maximum bronchodilatory effect during 24 hours was similar for 600 μg Ro 25-1553 (7% (95% CI 4 to 10)) and the reference bronchodilator formoterol (10% (95% CI 7 to 12)). However, for both doses of Ro 25-1553 the bronchodilatory effect was attenuated 5 hours after inhalation whereas formoterol still had a bronchodilatory effect 12 hours after inhalation. Neither Ro 25-1553 nor formoterol produced any clinically relevant side effects. No drug related difference in adverse events was observed.
Conclusion: Inhalation of a synthetic selective VPAC2 receptor agonist constitutes a promising approach for bronchodilation in patients with asthma.
- asthma
- pituitary adenylate cyclase-activating peptide (PACAP)
- vasoactive intestinal peptide
- Ro 25-1553
Statistics from Altmetric.com
The endogenous neuropeptide vasoactive intestinal peptide (VIP) inhibits smooth muscle tone in guinea pig airways, both when administered in vitro and when given by inhalation in vivo.1–5 As shown in guinea pig airways in vitro, this effect is mediated via VIP-PACAP (VPAC) receptors because VIP and pituitary adenylate cyclase activating peptide (PACAP) display a similar potency.6,7 The activation of these VPAC receptors is followed by a subsequent increase in intracellular cyclic AMP.8 Based on its effects in guinea pig airways, it has been suggested that VIP possesses potential as a bronchodilator and, indeed, it has been shown that VIP can inhibit histamine induced smooth muscle tone in human bronchi in vitro.9 It has also been shown that VIP can cause a bronchodilatory effect when it is administered intravenously in asthmatic subjects, but not in healthy volunteers.10,11 In spite of these findings, the bronchodilator potential of VIP has been questioned mainly for two reasons. Firstly, it has been shown that inhaled VIP is degraded by endogenous proteases such as neutral endopeptidase (NEP) present on bronchial epithelial cells as well as chymase and tryptase derived from mast cells.12–19 Secondly, intravenous administration of VIP has been shown to cause cardiovascular side effects in asthmatic and healthy subjects.10,11 To reduce systemic side effects a VIP-like bronchodilator should probably be given by inhalation, but must then be resistant to degradation by proteases.
A synthetic VIP analogue Ro 25-1553 has recently been developed by Bolin and coworkers.20 This selective VPAC2 receptor agonist is more potent than original VIP and the β2 adrenoceptor agonist salbutamol in inhibiting histamine induced airway smooth muscle tone in guinea pig trachea and in human bronchi in vitro and when given by inhalation in guinea pigs in vivo.9,12,21,22 In vivo studies in guinea pigs have shown that the duration of the bronchodilatory effect tends to be longer for Ro 25-1553 than for salbutamol.9 In line with this, Ro 25-1553 displays a duration of action similar to that of formoterol in the guinea pig trachea in vitro.23
We have determined whether inhalation of the selective VPAC2 receptor agonist Ro 25-1553 causes a bronchodilatory effect in patients with moderate stable asthma using the long acting β2 adrenoceptor agonist formoterol as a reference bronchodilator.24,25
METHODS
Patients with asthma
Patients were recruited from patient files within the three centres involved in the study. The inclusion criteria were male sex, outpatient care, age 18–60 years of age, and a history of stable asthma as defined by the American Thoracic Society.26 Patients had to have a baseline FEV1 of ≥60% predicted and <100% predicted, and FEV1 reversibility of ≥15%. Only patients who, apart from their asthma, were judged healthy by physical examination, vital signs, electrocardiography and clinical laboratory tests were included. All included patients were able to use the inhalation devices. The exclusion criteria for the study were oral glucocorticoid treatment, β adrenoceptor blocker treatment, or a respiratory tract infection during the 4 weeks before the study, scheduled inpatient surgery during the study, hypersensitivity to β adrenoceptor agonists or lactose, tobacco smoking during the 6 months before the study, abnormal echocardiogram, blood donation during the 3 months before the study, known alcohol or other drug abuse, previous randomisation in the study, or participation in another clinical study within 4 weeks of the current one. Inhaled long acting β2 adrenoceptor agonists were not allowed during the study and had to be withdrawn at least 72 hours before visit 1.
The study was approved by the independent ethics committee at the Medical Faculties of Göteborg, Lund and Uppsala University, respectively, and was conducted in accordance with the Helsinki Declaration. All patients gave oral and written informed consent before participating in the study. Good clinical practice procedures were applied and the study was monitored by the sponsor (AstraZeneca R&D, Lund, Sweden).
Protocol
This was a placebo controlled study with a double blind, crossover, double dummy design, comprising a total of six study visits. Visit 1 constituted a screening visit for informed consent and enrolment, as well as standard physical examination, lung function and reversibility testing. All patients underwent supervised practice with the inhalation devices (specified below) at visit 1. Provided that the dose was kept constant for at least 4 weeks before the study, inhaled and nasal glucocorticoids, disodium cromoglycate and antihistamines were allowed during the study. Inhalation of short acting β2 adrenoceptor agonists and/or ipratropium bromide was allowed during the study, provided that dosing did not occur within 6 and 8 hours, respectively, before the administration of randomised treatment. Visit 2 constituted the first visit for randomised treatment and took place 1–14 days after visit 1. Visits 3–5 were also treatment visits and took place 3–14 days after the preceding visit. After receiving the randomised treatment in the morning at visits 2–5, the patient remained at the clinic for 12 hours and returned to the clinic for a 24 hour assessment during the following morning. Visit 6 was a follow up visit which took place 3–5 days later and included a physical examination.
Lung function
Forced expiratory volume in 1 second (FEV1) was the primary variable of the study and all other variables were regarded as secondary. FEV1 was assessed using a standard spirometer (Vitalograph Alpha, Vitalograph Ltd, Buckingham, UK) at visits 1–5. The reversibility test at visit 1 was conducted before and 15 minutes after one inhalation of terbutaline 0.5 mg (Bricanyl Turbuhaler, Astra Pharmaceutical Production, Sweden). For each FEV1 recording during visits 2–5, the best of three FEV1 measurements was used for evaluation. Throughout the study the FEV1 had to be within ±12% of the baseline FEV1 at visit 1. Patients were rescheduled up to two times if this criterion was not fulfilled. At visits 2–5 FEV1 was assessed 15 minutes before and 3, 15, 30, 45, 60, 90 minutes and hourly for up to 12 hours after treatment. A final FEV1 assessment was performed 24 hours after treatment.
Vital signs
The pulse rate, systolic and diastolic blood pressure assessments were performed at the same time points as FEV1 (see above). In addition, sitting blood pressure was assessed before and 30, 60 and 90 minutes and hourly for up to 12 hours after treatment.
Electrocardiography (ECG)
The following ECG parameters were collected at visits 1 and 6 as well as before and 60 minutes, 12 and 24 hours after each randomised treatment at visits 2–5: conduction, extra systoles, heart rate, QRS duration, QT interval, PR interval, sinus rhythm, and ST-T changes. These parameters, plus QTc and QTc dispersion, were finally evaluated after the completion of the study.
Echocardiography
Two dimensional echocardiography was carried out in accordance with standard clinical procedures by a skilled investigator for the evaluation of pericardial fluid (normal or abnormal) at visits 1 and 6 as well as before and 24 hours after each randomised treatment at visits 2–5. This was done because a preliminary safety study on primates (Cynomologous), conducted by other investigators, indicated an increased amount of pericardial fluid in some subjects after inhalation of Ro 25-1553 (unpublished data).
Clinical laboratory tests
Blood samples for control of serum potassium levels were collected at visits 1 and 6, as well as before and 12 hours after each randomised treatment at visits 2–5. Blood haemoglobin, haematocrit, red blood cells, platelets, white blood cells, differential blood cell count, serum levels of calcium, ASAT, ALAT, ALP, GT, bilirubin (total), albumin, sodium, creatinine, urea, glucose, chloride, and C reactive protein, and urinary protein, haemoglobin, erythrocytes, and glucose were also measured at these time points. All these samples were analysed using methods of standard clinical practice (Quintiles AB, Uppsala).
Adverse events
The adverse event profile was evaluated by means of open standardised questions at visits 2–6 and, when needed, by additional physical examination.
Study drugs
The study drugs were delivered at visits 2–5. The nebuliser solution of the synthetic VIP analogue Ro 25-1553 (trifluoroacetate salt) was manufactured by Pharmaceutical and Analytical R&D, AstraZeneca R&D, Lund, Sweden and was delivered for inhalation as an aerosol (100 μg or 600 μg delivered dose free peptide) using a nebuliser (HaloLite, Medic-Aid Ltd, UK). The corresponding placebo aerosol (2 ml of 9 mg/ml saline) was delivered using exactly the same conditions. The reference bronchodilator formoterol fumarate dihydrate was manufactured by Astra Pharmaceutical Production, Sweden and was delivered as inhalation powder (4.5 μg delivered dose) using a commercially available inhaler (Oxis Turbuhaler). The corresponding placebo powder (lactose) was delivered using exactly the same conditions.
Statistical analysis
The primary variable of this study was maximum change in FEV1 after each treatment. In addition, FEV1 at 3 minutes and 12 hours after treatment was analysed. The effect of each treatment on FEV1 was compared using a multiplicative (log tranformation of the dependent variable and covariate) analysis of variance model with patient, period, and treatment as fixed factors and the pretreatment FEV1 as a covariate. From this model, geometric mean treatment differences and corresponding 95% confidence intervals (CI) were calculated. A significance level of 5% was used—that is, differences were considered statistically significant when the 95% CI did not include a 0% increase.
The sample size was based on previous single dose studies with β2 agonists where the within patient coefficient of variation in 12 hour mean FEV1 had usually been around 6%. Assuming a similar variability in this study, 24 completed patients would give 80% power to detect a true increase of 5%. This assumed a significance level of 5% and a two sided alternative hypothesis.
RESULTS
Patients
Twenty four men (22 white and two of mixed race) with asthma were initially included in the study. However, one patient discontinued the study at day 10 because of exacerbation of asthma during the washout period after receiving only placebo (randomised treatment) and was not included in the analyses. Another patient received the incorrect treatment by mistake at two visits. Data from these two visits were excluded from analyses. The mean (SD) characteristics of the 23 patients included in the analyses at visit 1 were: FEV1 3.38 (0.47) l/s corresponding to 78 (7)% of predicted; reversibility 18.7 (3.9)% of FEV1; age 32 (9) years; weight 83 (11) kg; height 182 (8) cm; body mass index 25.1 (3.2) kg/m2; duration of asthma 18.8 (12.0) years. Fourteen of the 23 patients were receiving regular treatment with inhaled glucocorticoids.
Lung function
The mean (SD) baseline FEV1 was 3.40 (0.56) l/s for 100 μg Ro 25-1553, 3.39 (0.51) l/s for 600 μg Ro 25-1553, 3.40 (0.55) l/s for formoterol (4.5 μg), and 3.37 (0.47) l/s for placebo; there were therefore no substantial differences in this parameter before each treatment.
During the 24 hours of lung function monitoring after treatment, the geometric mean maximum increase in FEV1 was 16.2% for 100 μg Ro 25-1553, 18.2% for 600 μg Ro 25-1553, 21.5% for formoterol (4.5 μg), and 10.5% for placebo (as a percentage of baseline before treatment, n=22–23; see fig 1 for maximum CV). Compared with placebo, these differences were statistically significant (geometric mean (95% CI) difference: 5.1% (95% CI 2.8 to 7.6) for 100 μg Ro 25-1553, 7.0% (95% CI 4.5 to 9.5) for 600 μg Ro 25-1553, and 10.0% (95% CI 7.4 to 12.5) for formoterol 4.5 μg. There was no statistically significant difference between 600 μg and 100 μg Ro 25-1553 (geometric mean difference 1.7% (95% CI −0.6 to 4.1)). Formoterol 4.5 μg, however, produced a statistically significantly greater increase than 600 μg Ro 25-1553 (geometric mean difference 2.8% (95% CI 0.4 to 5.3)).
{kind=link}
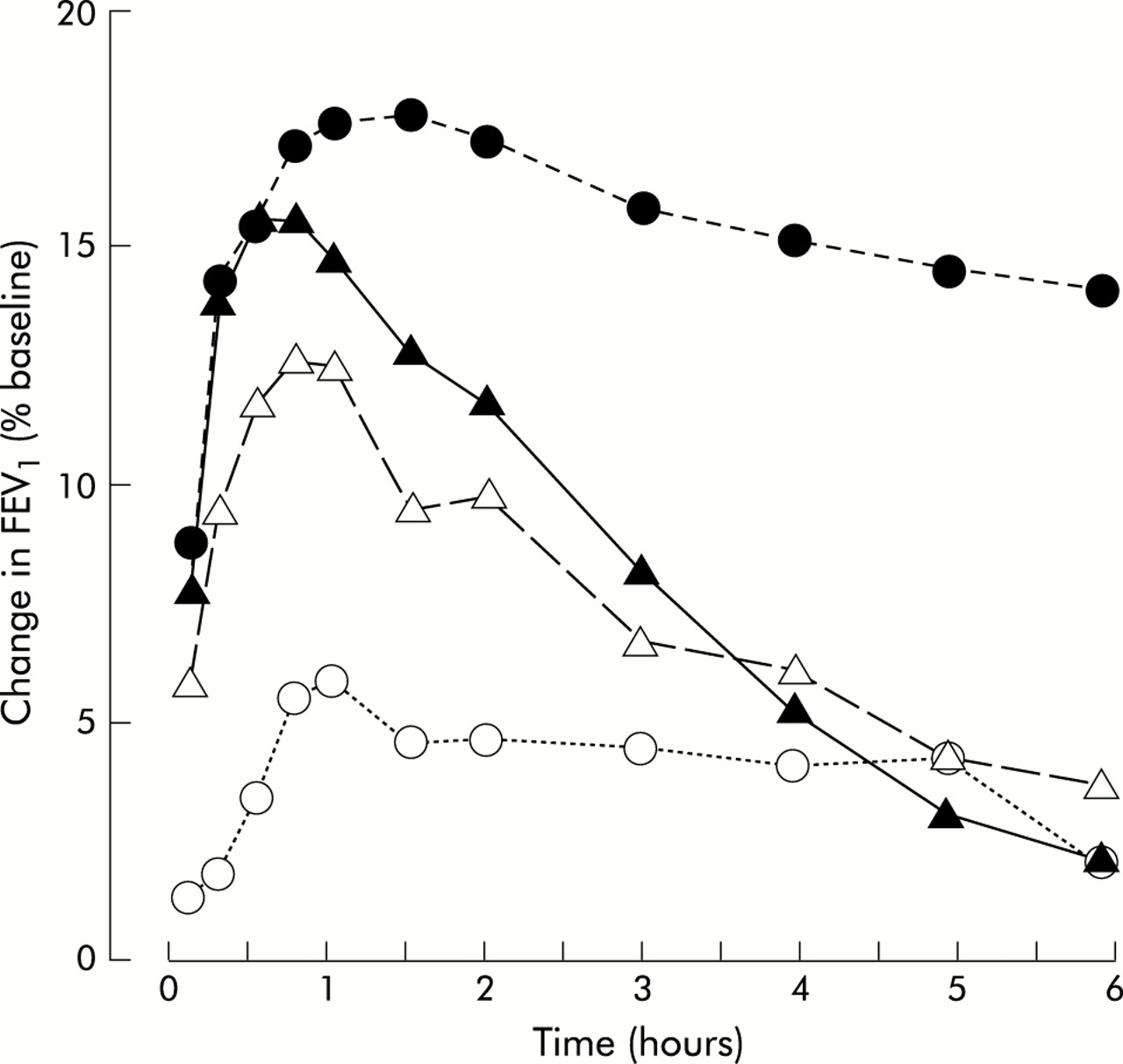
Forced expiratory volume in 1 second (FEV1, % of baseline before treatment) in patients with stable asthma after inhalation of the VPAC2 receptor agonist Ro 25-1553 (open triangles, 100 μg; closed triangles, 600 μg), the β2 adrenoceptor agonist formoterol 4.5 μg (closed circles) and placebo (open circles). Data are presented as geometric mean. The maximum between-patient coefficient of variation (CV) was 10.6%; n=22–23.
The time course of change in FEV1 during the first 6 hours after each treatment is shown in fig 1. Three minutes after inhalation Ro 25-1553 (100 μg and 600 μg) as well as formoterol (4.5 μg) had increased FEV1 more than placebo. At this time point the geometric mean difference (as a percentage of baseline before treatment) in FEV1 was 4.4% (95% CI 1.9 to 7.0) for 100 μg Ro 25-1553, 6.5% (95% CI 3.8 to 9.2) for 600 μg Ro 25-1553, and 7.8% (95% CI 5.1 to 10.5) for formoterol (4.5 μg) compared with placebo. Five hours after treatment the increasing effect on FEV1 of each dose of Ro 25-1553 was attenuated compared with placebo (fig 1). In contrast, the increasing effect of formoterol on FEV1 remained at 12 hours after treatment (9.7% v 0.3% for placebo); this difference was statistically significant (geometric mean difference 9.4% (95% CI 4.6 to 14.3)). Neither dose of Ro 25-1553 produced any increasing effect on FEV1 at 12 hours after treatment (100 μg 2.8%; 600 μg –2.5%). Neither treatment produced any increasing effect on FEV1 at 24 hours after treatment (100 μg Ro 25-1553 1.1%; 600 μg Ro 25-1553 −4.1 %; 4.5 μg formoterol 5.1%) compared with placebo (2.3%).
Vital signs
Overall, the maximum effect on systolic and diastolic blood pressure was small for all treatments (table 1). Similarly, the effect on pulse rate and sitting blood pressure of each respective treatment was small (data not shown).
Mean (SD) changes in systolic blood pressure, diastolic blood pressure, heart rate, QTc, and serum potassium levels 12 hours after inhalation of placebo, 100 μg Ro 25-1553 (Ro 100), 600 μg Ro 25-1553 (Ro 600), or 4.5 μg formoterol (Fo 4.5); n=22–23
Electrocardiography
The maximum effect of each treatment on heart rate and QTc was modest (table 1). Similarly, we were unable to detect any pronounced effect on either conduction, QRS duration, QT interval, PR interval, sinus rhythm, or ST-T changes (data not shown).
Echocardiography
The amount of pericardial fluid was within normal limits for all subjects before and 24 hours after each inhaled treatment (data not shown).
Clinical laboratory tests
The maximum effect of each treatment on serum potassium levels was small (table 1). Only very small changes or no change was seen in the other clinical laboratory tests during each treatment (data not shown).
Adverse events
There was no treatment related difference in reported adverse events (data not shown). No severe adverse events were reported throughout the course of the study.
DISCUSSION
Using the synthetic VIP analogue Ro 25-1553, this study is the first to show that inhalation of a selective VPAC2 receptor agonist can cause a clinically relevant bronchodilatory effect in patients with moderate stable asthma.
Ro 25-1553 was selected as a potential bronchodilator because of its advantageous combination of an aromatic amino acid sequence in the N-terminal domain, C-terminal helix, and its increased resistance to proteolytic degradation at key amino acid sites.12,20,27,28 In contrast to original VIP, the Ro 25-1553 molecule with its lactam ring inhibits airway smooth muscle tone not only in naive but also in inflamed airways. This has previously been shown by its effect on allergen induced smooth muscle tone in sensitised guinea pig airways in vivo, more recently in vitro in human bronchi from patients undergoing surgery for lung cancer (of whom the majority were tobacco smokers), and is now shown in patients with stable asthma.20,28,29 It is likely that the clearcut bronchodilatory effect in the airways of patients with asthma is facilitated by the ability of Ro 25-1553 to inhibit airway smooth muscle contraction caused by several pathogenetically relevant stimuli, as has been demonstrated in vitro and in vivo including histamine, leukotriene D4, and carbachol.9 The fact that the effect of Ro 25-1553 has been virtually unaffected by the β adrenoceptor blocker propranolol in tracheal smooth muscle from guinea pigs in vitro indicates a mechanism that is independent of the β2 adrenoceptor.9
When assessing the pharmacotherapeutic potential of Ro 25-1553, it should be emphasised that our study shows a longer duration of action for the reference bronchodilator formoterol than for Ro 25-1553 in the airways of patients with moderate stable asthma. This illustrates the limitation of the guinea pig airway model in which Ro 25-1553 was found to have a relatively long duration of action.9,23 Because of its limited duration of action, Ro 25-1553 will probably not be established as a bronchodilator for clinical use in asthma. Rather, the current results should prompt the development of new selective VPAC2 receptor agonists with an increased duration of action. Such synthetic analogues of VIP may provide a useful complement to β2 adrenoceptor agonists in the treatment of asthma.
Our study shows that inhalation of Ro 25-1553 at doses causing a bronchodilatory effect does not lead to any clinically substantial side effects on the cardiovascular system. No pronounced effects were seen on either blood pressure, heart rate, QTc, or pericardial fluid. Furthermore, no significant effects were seen on serum potassium and other clinical laboratory tests. There were no adverse events related to the inhalation of Ro 25-1553.
In addition to its bronchodilatory effect, Ro 25-1553 may exert anti-inflammatory effects. Thus, it has been shown that Ro 25-1553, but not original VIP, inhibits allergen induced thromboxane A2 release in sensitised lungs from guinea pigs perfused in vitro as well as allergen induced eosinophil recruitment in sensitised guinea pig airways in vivo.30 Ro 25-1553 also inhibits endotoxin induced release of the pro-inflammatory cytokines tumour necrosis factor (TNF)-α and interleukin (IL)-12 in human whole blood and in monocytes in vitro, presumably through activation of the VPAC2 receptor.31 It remains to be determined whether the bronchodilatory effect of inhaled Ro 25-1553 is parallelled by the anti-inflammatory effects in the airways of patients with asthma.
In conclusion, inhalation of the VPAC2 receptor agonist Ro 25-1553 in a single dose causes a rapid bronchodilatory effect in patients with moderate stable asthma without severe cardiovascular side effects. However, because of the limited duration of its bronchodilatory effect, longer acting VPAC2 receptor agonists should be developed and the bronchodilatory and anti-inflammatory effects evaluated in patients with asthma.
Acknowledgments
This work was funded by AstraZeneca R&D, Lund, Sweden and by the Swedish Research Council (project no K2001-71X-13492-02B). No funding, direct or indirect, was obtained from the tobacco industry. The authors thank the clinical staff of the Departments of Clinical Physiology at Sahlgrenska University Hospital, Göteborg, the Uppsala Academic Hospital and the Lund University Hospital for expert echocardiographic examination of the patients.