Article Text

Abstract
The Klippel-Trenaunay syndrome (KTS) is a rare syndrome characterised by the triad of varicose veins, bony and soft tissue hypertrophy, and cutaneous haemangioma. A 30 year old man with KTS with a right mediastinal mass which progressively enlarged over 5 years is described. Computed tomography, magnetic resonance imaging, and bronchial angiography revealed a vascular lesion in the azygous area. After complete excision of the mass, histological examination revealed cavernous haemangioma. To our knowledge, this is the first report of intrathoracic haemangioma in KTS.
- Klippel-Trenaunay syndrome
- haemangioma
- mediastinum
Statistics from Altmetric.com
Klippel-Trenaunay syndrome (KTS) is a rare congenital generalised mesodermal abnormality characterised by the triad of varicose veins, cutaneous haemangiomas, and hypertrophy of soft tissue and bone.1–3 It can be diagnosed on the basis of any two of the above three features. Since the first description of this syndrome in 1990 approximately 140 cases have been published in the literature, but its aetiology remains unknown.3
Previous reports of thoracic involvement in KTS were limited to pulmonary embolism, venous varicosity, and lymphatic obstruction.3 We present a 32 year old man with KTS with an unusual presentation of a mediastinal cavernous haemangioma in the azygous area. To our knowledge, this is the first report of intrathoracic haemangioma in KTS.
CASE REPORT
A 30 year old man presented at our outpatient clinic in July 2001 complaining of intermittent cough with scanty sputum for 1 year. There were no other respiratory symptoms such as chest pain, haemoptysis, or dyspnoea. He was a heavy smoker who had consumed one pack of cigarettes a day for 10 years. He was noted to have a haemangioma over his right back and hypertrophy of the right upper extremity 17 years before this admission. The diagnosis of KTS was made at that time and the haemangioma was surgically removed. A mass in the right scrotum was noted 13 years earlier and the surgical biopsy also revealed a haemangioma. A chest radiograph at a local hospital 5 years previously was normal.
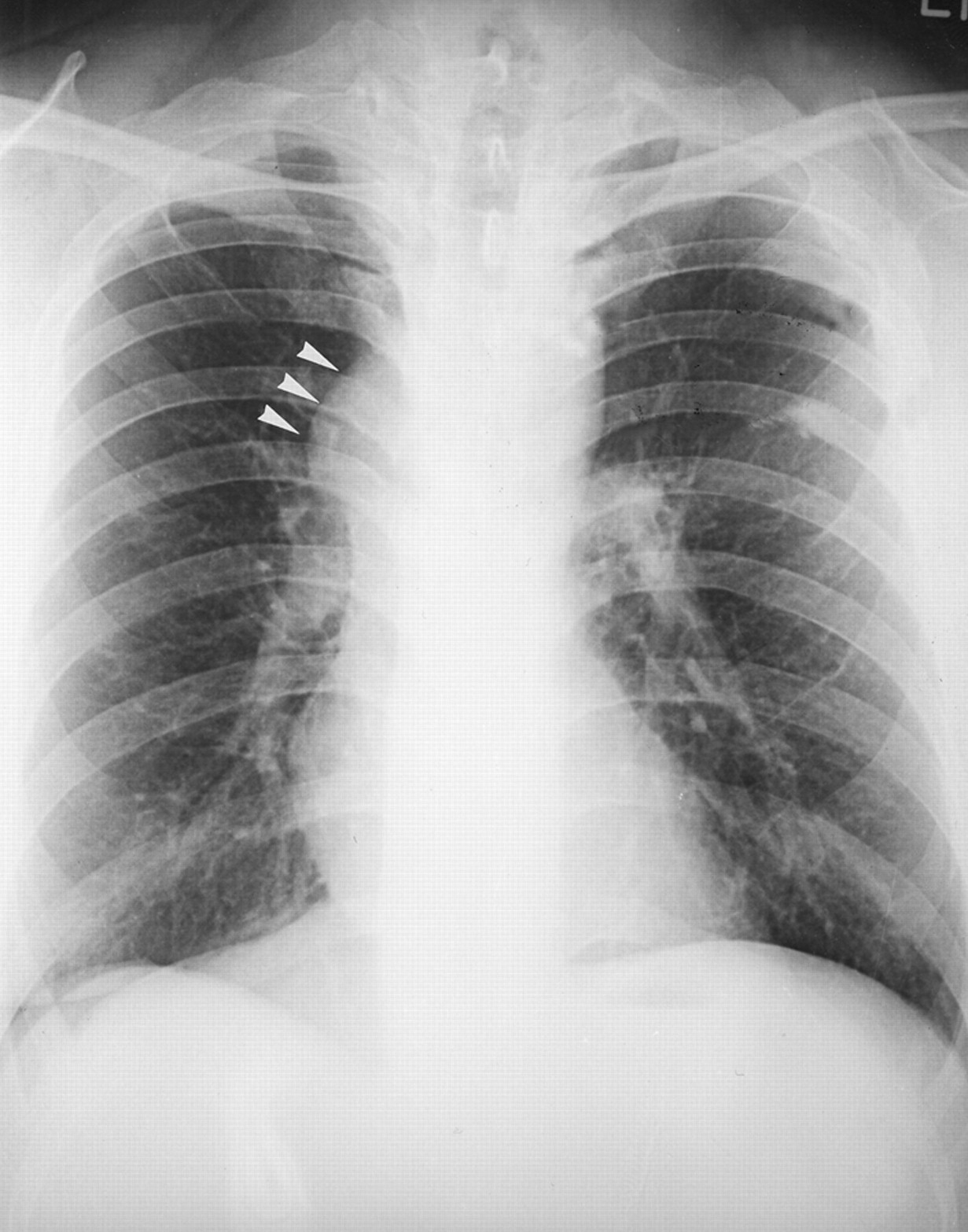
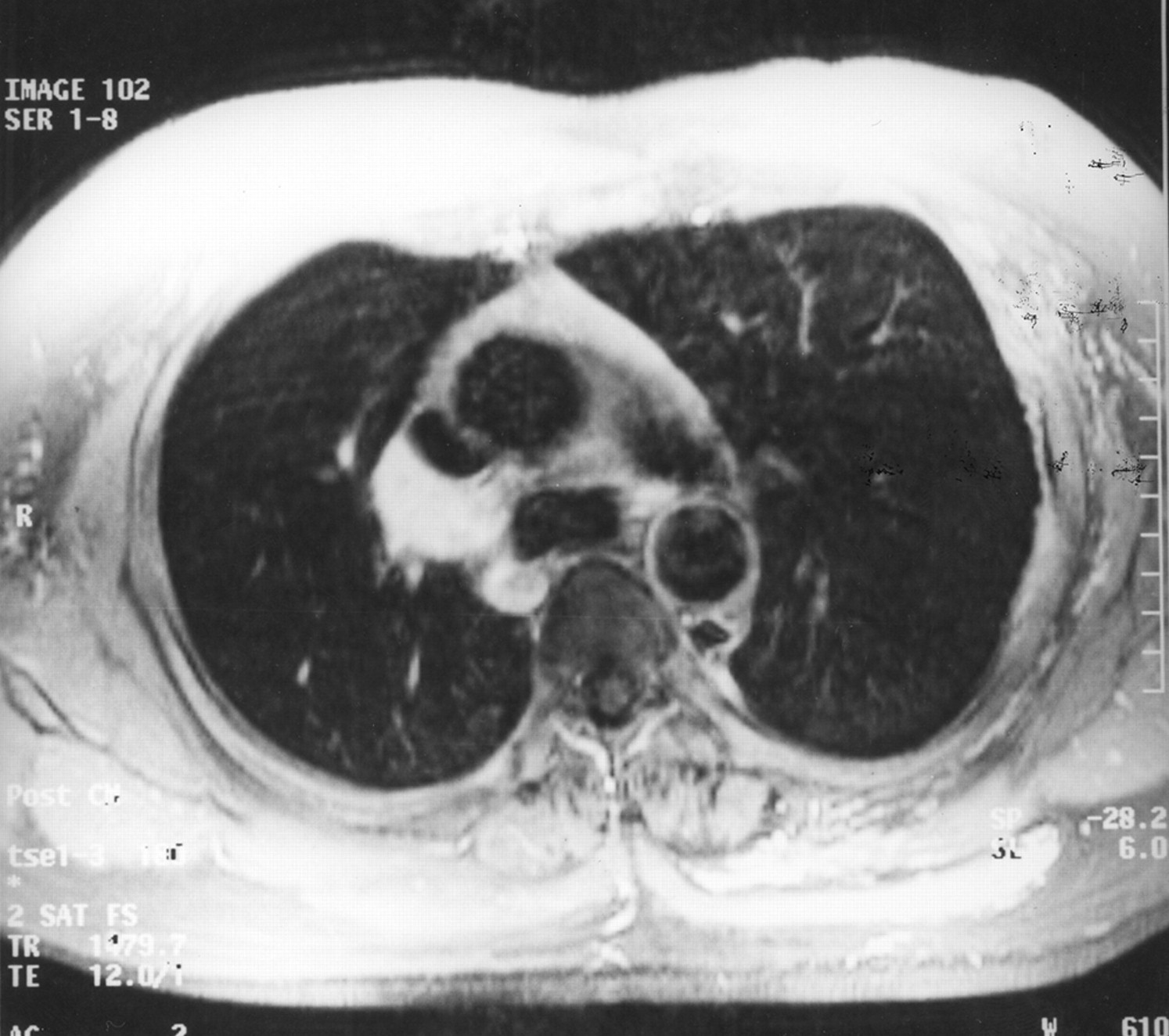
On examination the blood pressure was 130/90 mm Hg, his pulse rate was 90/min, and his respiration 25 breaths/min. There was hemihypertrophy of his right upper extremity. Chest auscultation did not reveal abnormal breathing sounds or bruits. There was no cyanosis of digital clubbing. A chest radiograph at this time showed a mediastinal lesion over the right perihilar area (fig 1); a computed tomography (CT) scan of the chest showed a mass with only partial enhancement located between the superior vena cava (SVC) and azygous vein (fig 2); and magnetic resonance (MR) imaging (fig 3) revealed a lesion low in signal intensity (SI) on the T1-weighted image and high in SI on the T2-weighted image, with intense enhancement after gadolinium diethylene-triamine penta-acetic acid (Gd-DTPA) injection. Angiography showed a hypervascular tumour in the right paratracheal area which was supplied by the right bronchial artery.

Chest radiograph showing a bulging lesion over the right mediastinal border (arrowheads).

CT scan of the chest revealing a mass with only partial enhancement located between the superior vena cava and the azygous vein.

{kind=link}
{kind=link}
{kind=link}
Magnetic resonance (MR) image showing a mass with intense enhancement after injection of gadolinium diethylene-triamine penta-acetic acid (Gd-DTPA).
The patient underwent a thoracotomy with en bloc excision of the vascular tumour. The tumour was found firmly adhered to the SVC, trachea, and azygous vein. The blood supply of the tumour came from the bronchial vessels, and the bridging arch between the azygous vein and SVC was obliterated by the tumour. The azygous vein was divided and part of the SVC was resected during the dissection of the tumour. Histological examination of the specimen revealed a well circumscribed vascular-proliferative lesion composed of large thick-walled vessels with prominent muscular wall and occasional cavernous spaces. Some lymphocytic aggregations were also present in the soft tissue. The findings were compatible with cavernous haemangioma. The postoperative course was smooth and the patient was discharged 1 week after the operation.
DISCUSSION
The vascular disorder in KTS is a combined capillary, venous, and lymphatic malformation with no evidence of substantial arteriovenous shunting.4 The capillary malformations are usually “port wine” stains which frequently are located laterally and may be found at sites other than the hypertrophied limb.5 The deep vein anomalies include atresia, hypoplasia, valvular incompetence, aneurysmal dilatation, duplication, external compression by fibrous bands or anomalous vessels, and arteriovenous microfistula.2 The popliteal and femoral veins are most commonly affected, although all the veins of the limbs, including the lower inferior vena cava, can be involved.
More than 20 patients with pulmonary embolism associated with KTS have been reported. The literature suggests that venous thromboembolism is common in KTS, with a frequency in larger series ranging from 8% to 22%.6 The precise mechanism for this increased risk of thromboembolism, however, remains unclear. Recurrent or unresolved pulmonary embolism can lead to the development of pulmonary hypertension or right ventricular failure in patients with KTS.7 Other reported pulmonary abnormalities in KTS include pulmonary vein varicosity in an infant8 and pleuropericardial effusion due to lymphatic obstruction in an adult.3 To our knowledge, no previous case of intrathoracic haemangioma has been described. Findings of the case presented here suggest that vascular abnormalities in this syndrome can be more generalised and deeply seated than previously thought. It is interesting to speculate whether a unifying angiogenic process may be involved in the pathogenesis of KTS.
Mediastinal haemangiomas are rare intrathoracic lesions that are grossly well circumscribed, cystic, haemorrhagic tumours ranging in diameter from 2 cm to 20 cm.9 Because of their solid appearance, large size, and often infiltrative growth, these tumours are easily mistaken radiologically for a malignancy. As in those described in soft tissue, mediastinal haemangiomas can be classified histologically into capillary and cavernous types. Capillary haemangiomas are characterised by a lobular and solid growth pattern featuring dilated small vessels and a solid proliferation of endothelial cells, while cavernous haemangiomas have large dilated vascular spaces with areas showing interstitial inflammatory changes, fibrosis, and smooth muscle proliferation.9 The capillary type closely resembles juvenile capillary haemangiomas of the skin. Unlike cutaneous and subcutaneous tumours in children and young adults, the lesions in the mediastinum did not show any sex or age predilection and occurred with equal frequency in children and adults. Such tumours have a sporadic tendency for multifocality and may simultaneously involve the mediastinum, skin, spleen, liver, and kidneys. One feature that may introduce difficulties in diagnosing these tumours is the presence of regressive or degenerative changes, including stromal hyalinisation, dystrophic ossification, and cystic and perivascular myxoid changes.
Other intrathoracic disorders that should be considered in the differential diagnosis of mediastinal haemangiomas include arteriovenous malformations seen in the Osler-Weber-Rendu syndrome, epithelioid haemangioendothelioma, sclerosing haemangioma, haemangiopericytomas, angiolipoma, lymphangioma, and thymolipoma (especially the fibrous variant).9
A cautious approach is warranted in children and young adults with mediastinal haemangiomas because some lesions have been known to regress spontaneously.10 CT scanning and MR imaging are helpful in identifying the extent of visceral and soft tissue involvement. For lesions that are symptomatic or that compromise vital structures, surgical excision remains the treatment of choice.
We have described an adult with KTS with a progressively enlarged cavernous haemangioma. Physicians should be aware of this rare disease entity. Close observation of patients with KTS for internal vascular anomalies is necessary to prevent life threatening complications such as pulmonary thromboembolism or compression of vital structures.