Article Text

Abstract
Background: The roles of matrix metalloproteinases (MMPs) in cancer metastasis have been studied. Macrophages are considered to release MMPs in the tissues of patients with lung cancer.
Methods: Intracellular collagenase activity was measured in CD14+ CD45+ cells from bronchial lavage fluid to establish a new diagnostic tool for lung cancer. Between August 2000 and November 2001 bronchoscopy and bronchial lavage were performed in 45 patients with abnormal shadows on the chest radiograph; 21 had lung cancer and 24 had non-malignant disease.
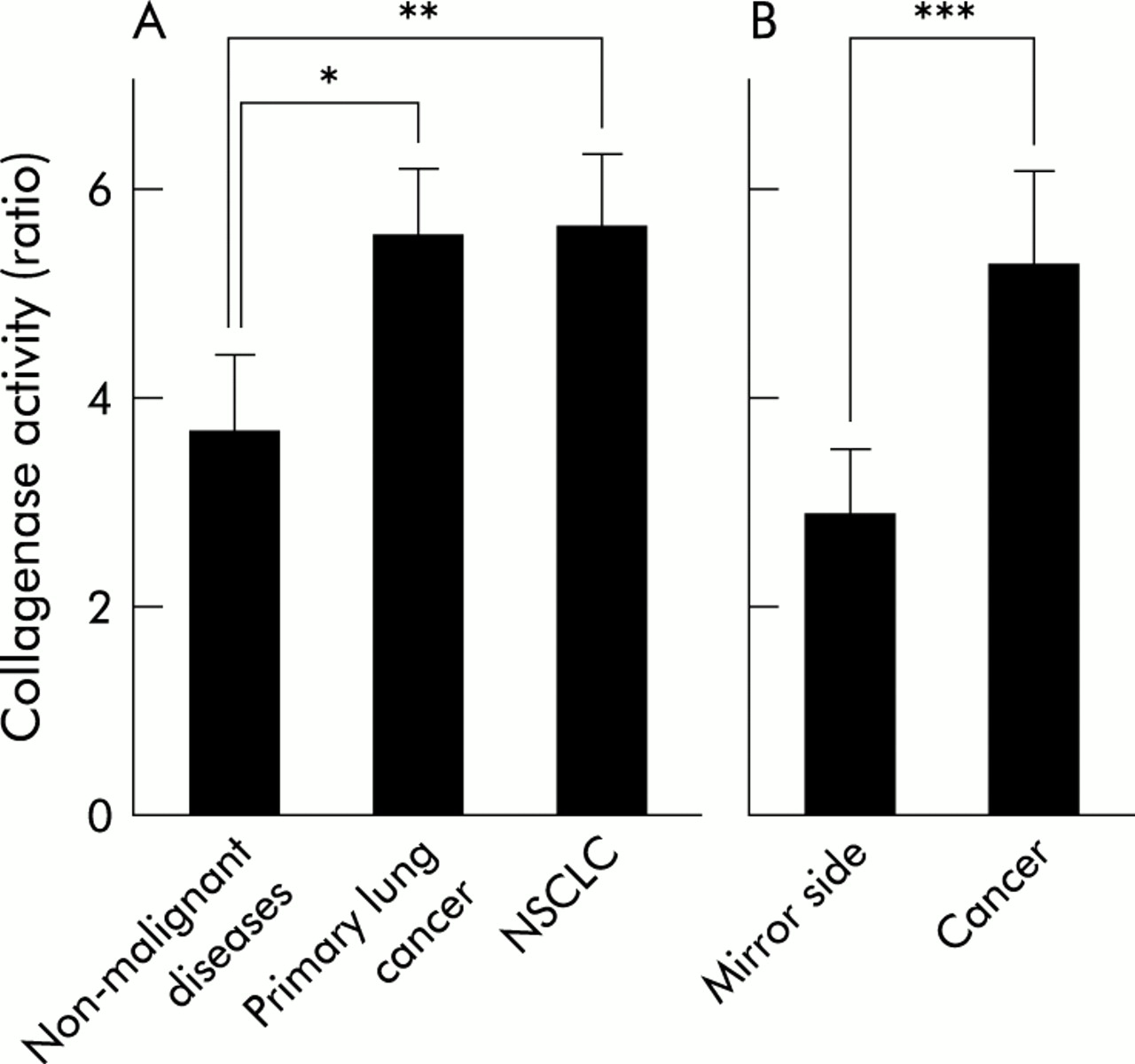
Results: Collagenase activity in patients with primary lung cancer (5.54 (0.65)) or non-small cell lung cancer (NSCLC) (5.62 (0.71)) was significantly higher than in those with non-malignant disease (3.63 (0.78), p=0.006 and p=0.008, respectively). Only three of 18 patients in the low activity group were diagnosed as having cancer compared with 18 of 27 in the high activity group (p=0.001). This significance was not seen in non-smokers but it was apparent in smokers/ex-smokers. Excluding non-smokers improved the specificity of collagenase activity in differentiating cancer and non-malignant disease from 62.5% to 80.0%. The sensitivity of the test was 85.7% in all patients and 88.2% in smokers/ex-smokers.
Conclusions: Measurement of intracellular collagenase activity in macrophages in bronchial lavage fluid is a useful diagnostic tool for distinguishing between cancer and non-malignant diseases, especially in smokers and ex-smokers.
- matrix metalloproteinase
- macrophage
- lung cancer
Statistics from Altmetric.com
Cancer progression has been shown to be correlated with the expression of extracellular proteinases such as matrix metalloproteinases (MMPs) and serine proteinases.1,2 MMPs might be involved in various processes of cancer progression such as destruction of the basement membrane, entry and exit of tumour cells from the circulation, local migration, creation of a microenvironment for tumour growth, and angiogenesis of tumours.3 The basement membrane is composed of type IV collagen, laminin, entactin, proteoglycans, and glycosaminoglycans.4 Among members of the MMP family, type IV collagenases were identified in the early 1980s as being involved in tumour invasion.5 Expression of mRNA of the type IV collagenases MMP-2 and MMP-9 has been detected in non-small cell lung cancer (NSCLC).6,7 Immunohistochemical study has also demonstrated expression of MMP-28,9 and MMP-910 in NSCLC. Increased plasma levels of MMP-211 and MMP-912 in patients with NSCLC have also been reported. The origins of the MMPs are still controversial. Although there has been a report that lung cancer cells themselves produce type IV collagenases,13 in situ hybridisation studies have shown that it is the stromal fibroblasts and inflammatory cells surrounding the cancer cells that are responsible for MMP expression.3,14 Macrophages may be involved in this release of MMP. Expression of MMPs—for example, MMP-12,15 MMP-2, MMP-9,16 and MMP-717—has been reported on human macrophages. Cancer cells are now considered to promote cancer progression by releasing cytokines or extracellular MMP inducers to induce the production of proteinases by stromal fibroblasts and inflammatory cells.18 These proteinases, localised on the surfaces of cancer cells, may play an important role in substrate degradation and cell migration.18 The infiltration of macrophages in NSCLC tumours has been demonstrated by immunohistochemistry. It has been suggested from the results of in vitro chemotaxis assays that this infiltration is accompanied by monocyte chemotactic activity that is higher in NSCLC homogenates than in normal lung tissue.19 There is now much evidence to support the role of macrophages in tissue destruction during cancer metastasis.20
Lung cancer remains the most common cause of cancer related deaths.21 The survival rate in advanced NSCLC remains poor.22 The use of MMP inhibitors in advanced cancers has not improved clinical outcomes,23 but the use of MMP inhibitors in the earlier stages of cancer may be beneficial. The diagnostic applications of MMPs have not yet been well established.
It has recently become possible to measure protease activity in single intact cells by using a CellProbe (Beckman Coulter, Fullerton, CA, USA). We have used this technique to demonstrate a significant correlation between susceptibility to infection and decreased antibiotic enzyme activity in neutrophils from patients with haematological disorders.24 In the present study we measured collagenase activity in macrophages collected from bronchial lavage fluid in an attempt to establish a new and useful diagnostic tool for lung cancer.
METHODS
Patients and cells
Between August 2000 and November 2001 bronchoscopy and bronchial lavage were performed in 45 patients with any type of abnormal shadow on chest radiography, including consolidation, infiltration, and reticular shadows in the lung field. Informed consent was obtained before bronchoscopy from all patients. There were 21 patients (16 men) of mean age 65.3 years (range 22–81) with lung cancer; 12 had adenocarcinoma, five squamous cell carcinoma, one mucoepidermoid carcinoma, two small cell carcinoma, and one metastasis from hepatoma. Twenty four patients (15 men) of mean age 60.0 years (range 22–83) with non-malignant lung disease were also examined. Of the NSCLC patients, three were stage I, none stage II, nine stage III, and six stage IV.
The fibreoptic bronchoscope was wedged at the point of division of the bronchus that showed abnormal shadows on the CT scan. 50 ml of saline was flushed into the bronchus and the cells in the lavage fluid were collected by bronchoscopy. In six patients with lung cancer, bronchial lavage was also performed on the healthy bronchus on the mirror side of that affected by cancer.
In our analysis of collagenase activity in patients according to their smoking status, smokers were defined as those with a current habitual experience of smoking or experience within the previous 6 months. Patients with past habitual experience of smoking more than 6 months previously were defined as ex-smokers, and those with no experience of habitual smoking were defined as non-smokers.
Agents
Phycoerythrin cyanin 5 (PC5) conjugated CD45 monoclonal antibody and RD1 conjugated CD14 monoclonal antibody were purchased from Beckman Coulter. GFGA-Collagenase (CellProbe) was also obtained from Beckman Coulter.
Macrophage intracellular enzyme activity
Measurement of intracellular enzyme activity was performed with a CellProbe.24,25 It included enzyme substrates labelled with fluorescent dyes. Fluorescence does not occur until the dyes are released from the substrates by these enzymes. The fluorescence intensity is related to the amount of products converted from the substrates.
Cell suspensions of about 1 × 107/ml were prepared from bronchial fluid. Each sample of 100 μl was mixed with 5 μl of anti-CD14 monoclonal antibody. After the samples had been kept for 10–15 minutes at room temperature, they were washed twice with phosphate buffered saline (PBS). Cells were kept for 10–15 minutes at room temperature again after addition of 5 μl anti-CD45 monoclonal antibody. The cell suspension was adjusted to 3 × 106/ml after the cells had been washed twice with PBS. A 50 μl sample was incubated for 7 minutes at 37°C; 25 μl of CellProbe was added before incubation for an additional 10 minutes at 37°C. The reaction was stopped on ice for 5 minutes and samples were treated with Q-Prep (Beckman Coulter) to lyse the erythrocytes. The emitted fluorescence was monitored with an EPICS XL flow cytometer (Beckman Coulter). Samples were analysed by three-colour patterns in the flow cytometer. CD14 positive and CD45 strongly positive cells were considered to be macrophages. The settings of the flow cytometer were adjusted by Flow-Check (Beckman Coulter) and the fluorescence intensity was standardised for each assay with Flow-Set (Beckman Coulter) to maintain reproducibility from day to day. Enzyme activity was quantitated as mean fluorescence intensity. Values were expressed as the ratio of fluorescence intensity between samples with and without CellProbe, as previously described.24
Statistical analysis
Data were expressed as mean (SE) values. Wilcoxon’s rank sum test and Fisher’s exact probability test were used, and a p value of 0.05 or less was considered significant.
RESULTS
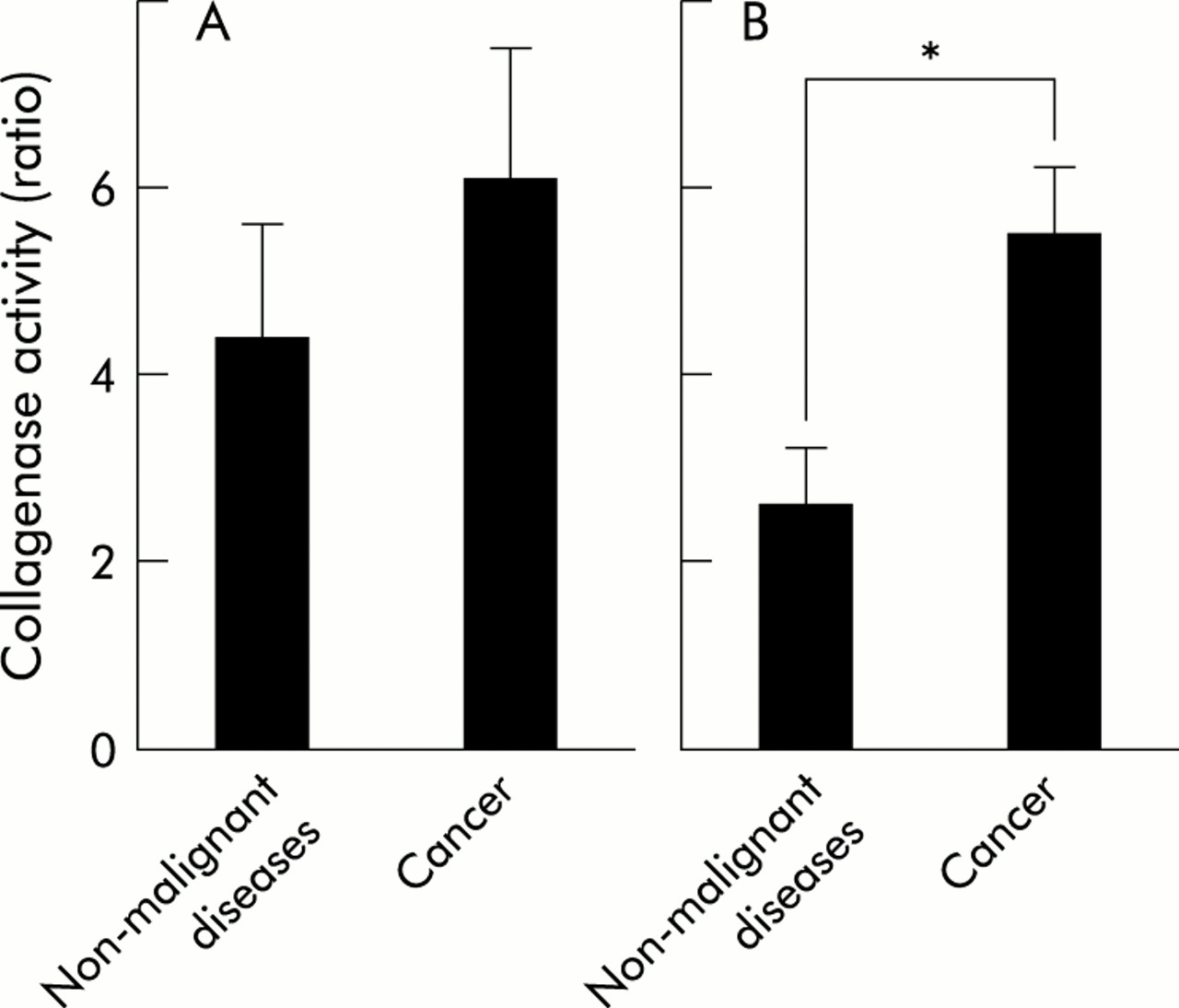
The collagenase activity inside macrophages from the bronchial lavage fluid of patients with lung cancer or non-malignant respiratory disease was measured, and was significantly higher in patients with primary lung cancer than in those with non-malignant disease (5.54 (0.65) v 3.63 (0.78); p=0.006, fig 1A). Patients with NSCLC had significantly higher levels of collagenase activity than those with non-malignant disease (5.62 (0.71) v 3.63 (0.78); p=0.008, fig 1A). In lung cancer patients, including those with metastatic cancer, samples taken from bronchi with abnormal shadows had significantly higher levels of collagenase activity than samples from the mirror side in the same patients (5.26 (0.92) v 2.89 (0.63); p=0.035, fig 1B).

(A) Collagenase activity in all patients with primary lung cancer (n=20) and patients with NSCLC (n=18) was significantly increased compared with that in subjects with non-malignant disease (n=24); *p=0.006, **p=0.008. (B) Samples from bronchi with abnormal shadows had significantly higher levels of collagenase activity than those from the mirror sides in the same patients with lung cancer, including metastatic cancer (n=6); ***p=0.035.
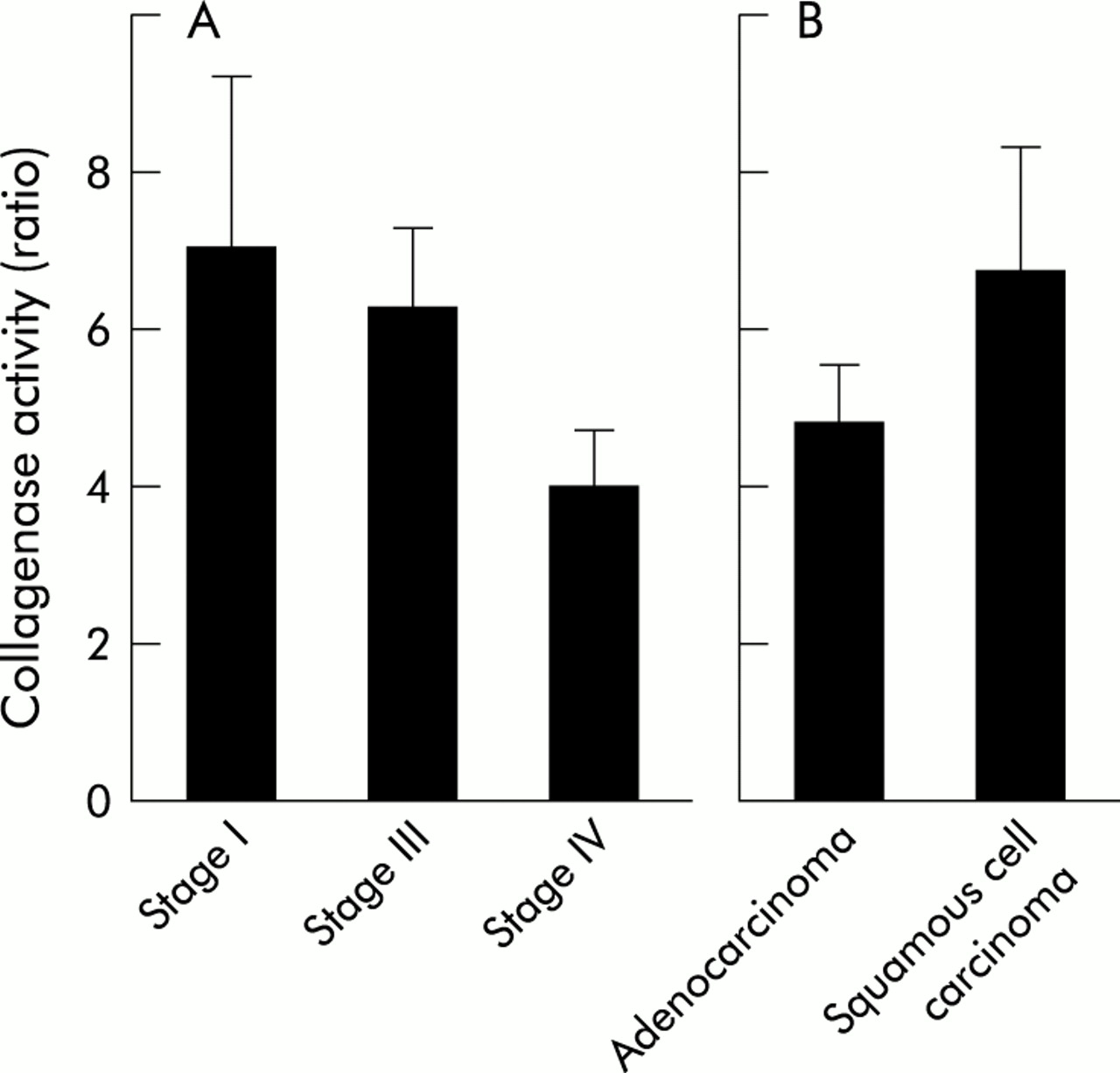
In patients with NSCLC we failed to show any significant differences in collagenase activity with clinical stage according to TNM criteria. Although there were no significant differences among clinical stages, collagenase activity was relatively high in earlier stage cancers (7.02 (2.27) in stage I, 6.26 (1.07) in stage III, 3.97 (0.76) in stage IV; fig 2A). Among three patients in stage I disease, collagenase activities in the two patients with stage IA were both relatively higher (9.95 and 8.54) than that of a patient in stage IB (2.56). No significant difference was observed in collagenase activity between patients with adenocarcinoma and squamous cell carcinoma (4.80 (0.74) v 6.74 (1.60); p=0.221, fig 2B).

Collagenase activity according to (A) clinical stage and (B) histology. No significant differences were seen between the groups.
We then analysed the correlations between collagenase activity and other factors such as smoking status (fig 3A), age (fig 3B), sex (Fig 3C), and C reactive protein (CRP) positivity (fig 3D). These values were calculated in patients with non-malignant disease (n=26) and in samples from the healthy mirror side bronchi of cancer patients (n=6). There were no significant differences between the groups in relation to either age or sex (figs 3B and 3C). Subjects with positive CRP activity (n=13) did not have significantly different levels of collagenase activity from those with negative CRP (n=15) (3.73 (1.28) v 2.40 (0.38), p=0.695, fig 3D). There were no differences between patients under 60 years of age (n=12) and those aged 60 years or more (n=16) (2.21 (0.42) v 3.51 (1.03), p=0.210, fig 3B). Female patients (n=9) had a mean collagenase activity of 4.50 (1.76) compared with 2.44 (0.37) in male subjects (n=20; p=0.322, fig 3C). Although we failed to demonstrate significant differences, the collagenase activity value of 3.59 (1.28) in non-smokers (n=13) was higher than the value of 2.87 (0.58) in smokers (n=11; p=0.582, fig 3A). The value of 2.20 (0.33) in ex-smokers (n=5) was lower (but not significantly so) than the value in non-smokers (p=0.313, fig 3A). The standard error was larger in non-smokers than in smokers or ex-smokers.

Collagenase activity in patients with non-malignant disease according to (A) smoking status, (B) age, (C) sex, and (D) C reactive protein (CRP).
Among non-smokers, the mean collagenase activity value of 6.06 (1.42) in patients with NSCLC (n=5) was not significantly different from the value of 4.35 (1.25) in patients with non-malignant disease (n=14; p=0.139, fig 4A). In contrast, there was a significant difference between the value of 5.45 (0.86) in patients with NSCLC (n=13) and the value of 2.64 (0.59) in patients with non-malignant disease (n=10) when smokers and ex-smokers were analysed together (p=0.016, fig 4B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Collagenase activity in (A) non-smokers and (B) smokers + ex-smokers. There was a significant difference between collagenase activity in 13 NSCLC patients and in 10 patients without malignant disease in group B (*p=0.016).
We also analysed these data using the Fisher’s exact probability test. Patients were divided according to their collagenase activity values into two groups: a “high” group with values of ⩾3.0 and a “low” group with values of <3.0. Only three of 18 patients in the low group were diagnosed with cancer, whereas 18 of 27 patients in the high group had cancer (p=0.001, table 1). When only patients with NSCLC were analysed, the results were also significant with 15 of 24 NSCLC patients in the high group but only three of 18 NSCLC patients in the low group (p=0.003). These trends were also analysed in non-smokers and smokers/ex-smokers. Among non-smokers, three cancer patients out of 10 were noted in the high group and one of eight in the low group (not significant: p=0.3824, table 1). In contrast, among the group of smokers/ex-smokers 15 of 17 in the high group and two of 10 in the low group were diagnosed as having cancer (p=0.0007, table 1).
Numbers of patients with high and low collagenase activity
We also analysed the sensitivities and specificities of collagenase activity values in the detection of cancer. In all patients a sensitivity of 85.7% and specificity of 62.5% were noted (table 2). In non-smokers both the sensitivity and specificity were lower at 75.0% and 50.0%, respectively (table 2), while in smokers/ex-smokers both were higher at 88.2% and 80.0%, respectively (table 2).
Sensitivities and specificities of collagenase activity detection in distinguishing cancer from non-malignant disease
No significant differences in survival were seen in any group of patients (data not shown).
DISCUSSION
Lung cancer is difficult to detect in the early stages and many cases are inoperable at diagnosis. Coin lesions, infiltrative shadows, and consolidation are commonly seen clinically on radiographs. A diagnosis of cancer requires pathological evidence, but an appropriate pathological diagnosis cannot always be obtained. We attempted to establish a new diagnostic method that could be used to verify the malignancy or non-malignancy of an abnormal shadow in the lung field by examination of bronchial lavage fluid. We also attempted to measure collagenase activity inside macrophages.
CD14 is an antigen specifically expressed on the surfaces of monocytes and macrophages, together with CD68 and CD163.26 CD14 is characterised as a receptor of lipopolysaccharide (LPS): LPS-binding protein (LBP) complex.27 It is also expressed on granulocytes and B lymphocytes.28 CD45 was originally cloned as a leucocyte cell surface molecule of high molecular weight; it has been extensively studied and found to have various roles.29 Among CD14+ cells, expression of CD45 is strong on the surfaces of monocytes/macrophages, whereas CD45 is weakly expressed on granulocytes. CD14+ and CD45 strongly positive cells (CD45++) are considered to be macrophages, and in this study we used CD14+ CD45++ cells. It is now possible to measure intracellular collagenase activity in intact individual cells.24,25 GFGA-collagenase (CellProbe) is responsive to type II and type IV collagenases. In human macrophages the type IV collagenases MMP-2, MMP-7, and MMP-9 have been reported to be present.15–17 This suggested that we would be able to measure the activity of MMP-2, MMP-7, and MMP-9 inside CD14+ CD45++ cells using this method.
Collagenase activity in macrophages in bronchial lavage fluids from patients with primary lung cancer was significantly higher than in those from patients with non-malignant disease (fig 1A). This result was strengthened by the significantly higher collagenase activity in bronchial lavage fluids from cancerous bronchi than in those from the presumably healthy mirror sides (fig 1B). These results suggest that macrophages around cancerous tissue are somehow activated to have increased potential to release collagenase. Although our result was not significant, the macrophages of patients in advanced clinical stages of cancer had lower intracellular collagenase activity than those of patients in less advanced stages (fig 2A). From these results, the hypothesis arises that collagenase is consumed as the stage of cancer progresses. This hypothesis is supported by studies that have used immunohistochemical and reverse transcriptase-polymerase chain reaction techniques to detect enhanced expression of MMP-2 and MMP-9 in lung cancer tissues.6–10 Serum levels of MMP-2 and MMP-9 are also increased in patients with NSCLC.11,12 Further, increased serum levels of MMP-2 are associated with metastasis and therapeutic response of lung cancer.11 In our study the relatively high activity of macrophage collagenase in the earlier stages increases the possibility that our technique may be of diagnostic use in the earlier stages of lung cancer.
We investigated factors other than cancer that may affect collagenase activity (fig 3). In the literature, high levels of plasma MMP-9 have been described in cigarette smokers.30 Production of collagenase by alveolar macrophages from patients with emphysema has also been reported as higher than in those from control subjects.16 We demonstrated that cigarette smoking might influence collagenase activity, although the result was not significant. Both current smokers and ex-smokers had relatively low intracellular collagenase activity compared with non-smokers (fig 3A). The reason for this is unclear. A plausible explanation is that consumption of collagenase after its release may cause the intracellular activity to be low. Since collagenase activity was low in smokers and ex-smokers (fig 3A), the power to distinguish patients with cancer would be enhanced in these groups. The specificity of collagenase activity values in differentiating malignancies in smokers and ex-smokers was 80% compared with 62.5% in all patients (table 2). The sensitivity was more than 80% in all patients and in smokers and ex-smokers (table 2). In contrast, the higher collagenase activity values and larger deviations in these values in non-smokers (fig 3A) make it more difficult to distinguish cancer and non-malignant disease in this group, as indicated by the significance values (fig 4A) and the marked reduction in sensitivity and specificity (table 2). These findings suggest that measurement of intracellular collagenase activity in macrophages in bronchial lavage fluid is a useful supportive diagnostic tool for distinguishing cancer and benign diseases, especially in smokers and ex-smokers. Since we have only two patients with small cell lung cancer, further investigation will be necessary for this type.
The method we usually use to distinguish between malignant and non-malignant diseases is cytology. Cytology generally has quite high specificity but the sensitivity is not always high. Among the patients we investigated, higher specificity and lower sensitivity were noted when we used cytology in bronchial lavage fluid (data not shown). The cases in which our method would be useful would be those in which there is a high index of suspicion of cancer but a negative cytological study. If intracellular collagenase activity was high in such cases, we would recommend a repeat bronchoscopic study. It is also important to point out that the results of intracellular collagenase activity measurements can be obtained a couple of hours after bronchoscopy, thus providing a clinical advantage.
Much attention has been focused on MMPs as contributors to metastasis or progression of malignant disease. The presence of an increased level of collagenase activity increases the possibility that lung cancer will be diagnosed. This report provides evidence that the measurement of collagenase activity in macrophages from patients with abnormal findings on chest radiography may have a clinical role and may be a useful diagnostic marker.
Acknowledgments
The authors thank Miss Ayako Hirota for her excellent technical assistance.