Article Text

Abstract
Background: The relationship between the clinical pattern of asthma and airway inflammation in childhood asthma is poorly characterised, yet underpins the treatment recommendations in current asthma guidelines. A study was undertaken to examine the relationship between airway inflammation and clinical asthma in children.
Methods: Children with asthma (n=146) and healthy controls (C, n=37) were recruited from primary and specialist clinics. Sputum induction and hypertonic saline challenge were performed.
Results: As the frequency of asthma episodes in the past 12 months increased, there were significant increases in sputum eosinophils (median; infrequent episodic (IE) 1.5%, frequent episodic (FE) 2.3%, persistent (P) 3.8%, control (C) 1.0%; p=0.002), sputum eosinophil cationic protein (ECP) (IE 113 ng/ml, FE 220, P 375, C 139; p=0.003), and desquamated bronchial epithelial cells (IE 2.0%, FE 6.0%, P 5.0%, C 2.5%; p=0.04). Treatment intensity was also associated with increased sputum eosinophils (p=0.005). The relationships between other severity markers (current symptoms, lung function) were less strong.
Conclusion: Children with more frequent episodes of clinical asthma exhibit increasing airway inflammation that is characterised by sputum eosinophilia and bronchial epithelial desquamation. The results support clinical assessment by frequency of wheezing episodes over the past 12 months when determining anti-inflammatory treatment requirements, and indicate that current symptoms are determined by mechanisms in addition to sputum eosinophilia.
- asthma
- children
- induced sputum
- eosinophil
Statistics from Altmetric.com
Asthma is a chronic inflammatory disorder of the airways in which the clinical pattern can be assessed based on the frequency of episodes.1 This classification is used to recommend the dose and type of anti-inflammatory treatment.1 The underlying assumption in this and other guidelines is that airway inflammation is linked to the clinical asthma pattern, and that airway inflammation increases as the clinical activity increases.
Studies which directly examine these assumptions have produced mixed results. In some studies, although sputum eosinophils were increased in children with asthma compared with healthy controls, inflammatory markers were not related to asthma severity.2–4 Other studies have found a weak relationship between symptoms and sputum eosinophils in patients with very mild asthma,5 and a non-significant trend for increasing sputum eosinophils with increasing current symptoms6,7 or asthma severity.8 These disparate results may relate to limited study sample size, selection of subjects from predominantly referral clinics, and the use of differing clinical classifications. We therefore sought to characterise the relationship between clinical asthma and airway inflammation in a large group of asthmatic children with a broad range of clinical disease recruited from both primary care and specialist clinics.
METHODS
Children with a diagnosis of asthma were recruited from respiratory clinics at John Hunter Children’s Hospital, from general paediatricians, and general practice. Children were eligible if they were at least 6 years of age, had a definite diagnosis of asthma, and were being reviewed on a routine basis for their asthma. Two general paediatricians and a GP with an interest in asthma were approached to refer children for study. In addition, the control children and other children with asthma were recruited from general practice as part of a project assessing the computer based diagnosis of asthma.9 Controls were randomly sampled and asthma was excluded on the basis of history, normal spirometric findings, and airways responsiveness, together with data review by a specialist. Following informed consent, a clinical asthma questionnaire was completed and spirometric tests were performed followed by hypertonic saline challenge and sputum induction.
Written informed consent was obtained from parents and children. The study was approved by the Hunter Area Research ethics committee and the University of Newcastle ethics committee.
Clinical classification of asthma
A diagnosis of asthma was made based on a history of current (past 12 months) episodic respiratory symptoms, a previous doctor’s diagnosis of asthma (ever), and the current (past 12 months) use of inhaled asthma treatment (β2 agonists, corticosteroids or cromolyn). A clinical asthma questionnaire6 was completed for each child by interviewing the parent.
The pattern of clinical asthma over the previous 12 months was categorised according to the frequency of symptomatic episodes,1,9 irrespective of treatment. Children with infrequent episodic asthma had <6 attacks per year, children with frequent episodic asthma had ⩾6 attacks in the past 12 months, and children with persistent asthma experienced asthma symptoms on most (⩾3) days each week. These cut off points were based on a prior analysis of questionnaire responses in comparison with respiratory paediatrician diagnosis of asthma.9
Asthma treatment was classified into three major groups: no preventative treatment, inhaled preventers (sodium cromoglycate and corticosteroids), and oral corticosteroid therapy. Asthma symptoms were also evaluated over the previous 2 weeks and classified as currently symptomatic based on the presence of wheeze, the presence of nocturnal waking due to asthma, a current exacerbation, or peak flow readings reduced from the subject’s best recordings.6
Spirometric tests
Children withheld short acting β2 agonists for 4 hours before testing. Height and weight were recorded and baseline spirometric tests performed (Med-Graphics AS-600 St Paul, MN, USA). Subjects performed three reproducible forced expiratory manoeuvres wearing nose clips to measure forced expiratory volume in 1 second (FEV1) and vital capacity (VC).
Saline challenge
Hypertonic saline (4.5%) challenge was performed as described previously.5 Briefly, 4.5% saline was inhaled for doubling time periods (30 seconds, 1, 2, and 4 minutes) from a DeVilbiss 2000 ultrasonic nebuliser (Oregon, Pike, PA, USA) and a Hans Rudolph 2700, two way non-rebreathing valve box (Hans Rudolph Inc, Kansas City, USA) with a rubber mouthpiece and nose clips.5 The nebuliser output was 1.8 ml/min and particle size (MMAD) <5 μm. FEV1 was measured 60 seconds after each saline dose. The test was stopped when the FEV1 had fallen by ⩾20% or 20 cumulative minutes of nebulisation time had elapsed. If FEV1 had fallen ⩾20% during the challenge, β2 agonist was administered using a metered dose inhaler. The dose of saline delivered to the patient was determined by weighing the nebuliser cup and tubing before and after the challenge.
Supplemental β2 agonist was administered if the FEV1 fell by more than 10% or if it fell to the exclusion level during the induction. Nebulisation was continued after there was clinical and lung function improvement.
Sputum induction
Sputum induction was conducted concurrently with the saline challenge as described previously.5 Before the hypertonic saline challenge was commenced the sputum induction procedure was explained to the subject. The technician demonstrated how to cough and clear the throat in order to propel mucus from the lungs into the mouth, and then to empty these contents into a sterile sputum container. Subjects were asked to rinse their mouth with water before the procedure to help eliminate squamous cell contamination of the sputum sample. They were asked to cough between each dose of nebulised saline to clear their throat and expectorate into the container. This procedure continued until an adequate sample containing >0.5 ml visible mucocellular material was obtained. If a satisfactory sputum sample was not obtained at the time the FEV1 had fallen ⩾20%, nebulisation with 4.5% saline was continued for 4 minute periods once the FEV1 had returned to within 10% of baseline.
Sputum processing
Sputum was selected from saliva and processed as described elsewhere.5–7 Briefly, sputum was treated by adding four volumes of 0.1% dithiothreitol (DTT-Sputolysin 10%; Calbiochem Corp, La Jolla, CA, USA) and mixed by rotating for 30 minutes at 37°C, followed by four volumes of phosphate buffered saline (PBS). The suspension was filtered through a 60 μm nylon gauze (Millipore, North Ryde, NSW Australia) and a total cell count of leucocytes and viability was determined. The cell suspension was centrifuged at 200g for 10 minutes and supernatant was aspirated and stored at −70°C. The cell pellet was resuspended in PBS to attain a concentration of 1 × 106 cells/ml and 70 μl placed into cups of a Shandon III cytocentrifuge (Shandon Cytospin, Sewickey, PA, USA) for slide preparation.
The quality of induced sputum samples was assessed based on the presence of an adequate number of cells for enumeration, the presence of pulmonary macrophages on the slide, and the proportion of squamous epithelial cells. This gave a quality score ranging from 0 (poor quality) to 6 (good quality sample).5
Cytochemistry
A differential cell count was obtained by counting 400 non-squamous cells on slides fixed with methanol and stained with May Grunwald Giemsa. Eosinophils were enumerated as the percentage of 400 cells on slides fixed with methanol and stained with Chromotrope 2R. Metachromatic cells were counted as the percentage of 1500 cells on slides fixed in Carnoy’s solution and stained with acidic toluidine blue. Cell counts were performed using coded slides by investigators blinded to the clinical characteristics of the subjects.
Fluid phase measurements
The concentration of ECP was determined in sputum supernatant by radioimmunoassay (ECP RIA; Kabi Pharmacia Diagnostics AB, Uppsala, Sweden) with standard curves based on dilutions of purified ECP. The limit of detection of the fluid phase ECP was 2 ng/ml.
Analysis of data
Data were analysed using STATA for Windows Version 5.0 (Stata Corp, College Station, Texas, US). Airways responsiveness was assessed as the dose-response slope and was log transformed for analysis with results presented as mean (SE). Cell counts were expressed as the median and interquartile range (IQR). Fluid phase measures were log transformed for analysis. Group comparisons were conducted using analysis of variance with Bonferonni post hoc testing for normally distributed variables and Kruskall-Wallis testing for non-parametric data. Associations between variables were examined using Pearson’s correlation coefficient. A multivariate analysis was performed using logistic regression with eosinophil count as the outcome variable. Eosinophil count was not normally distributed and was therefore categorised as <2.5% and ⩾2.5% based on previous normal values.6 Explanatory variables included clinical asthma pattern, treatment, age, and sex. A p value of <0.05 was considered significant.
RESULTS
The clinical characteristics of the children with asthma (n=146) and the healthy controls (n=37) are shown in table 1. The children were aged between 6 and 17 years; 49% reported having infrequent episodic symptoms in the past year, 27% had frequent episodic asthma, and 24% had persistent asthma symptoms. The children with persistent asthma were more symptomatic at the time of testing, with more children reporting night waking due to asthma (p=0.001) and morning waking with asthma (p=0.0003, table 1). The children with persistent asthma also had mildly reduced lung function (93% predicted; p=0.02, table 1). Airway responsiveness to 4.5% saline was assessed in 108 children (59%). There was a gradation in airway responsiveness to hypertonic saline, with a progressive and significant increase in dose-response slope as clinical severity increased (p=0.001, table 1).
Characteristics of children with asthma and healthy controls
Most children with persistent and frequent episodic asthma were taking inhaled corticosteroids (83% and 82%, respectively) compared with 58% children with infrequent episodic asthma (p=0.006, table 1).
Induced sputum
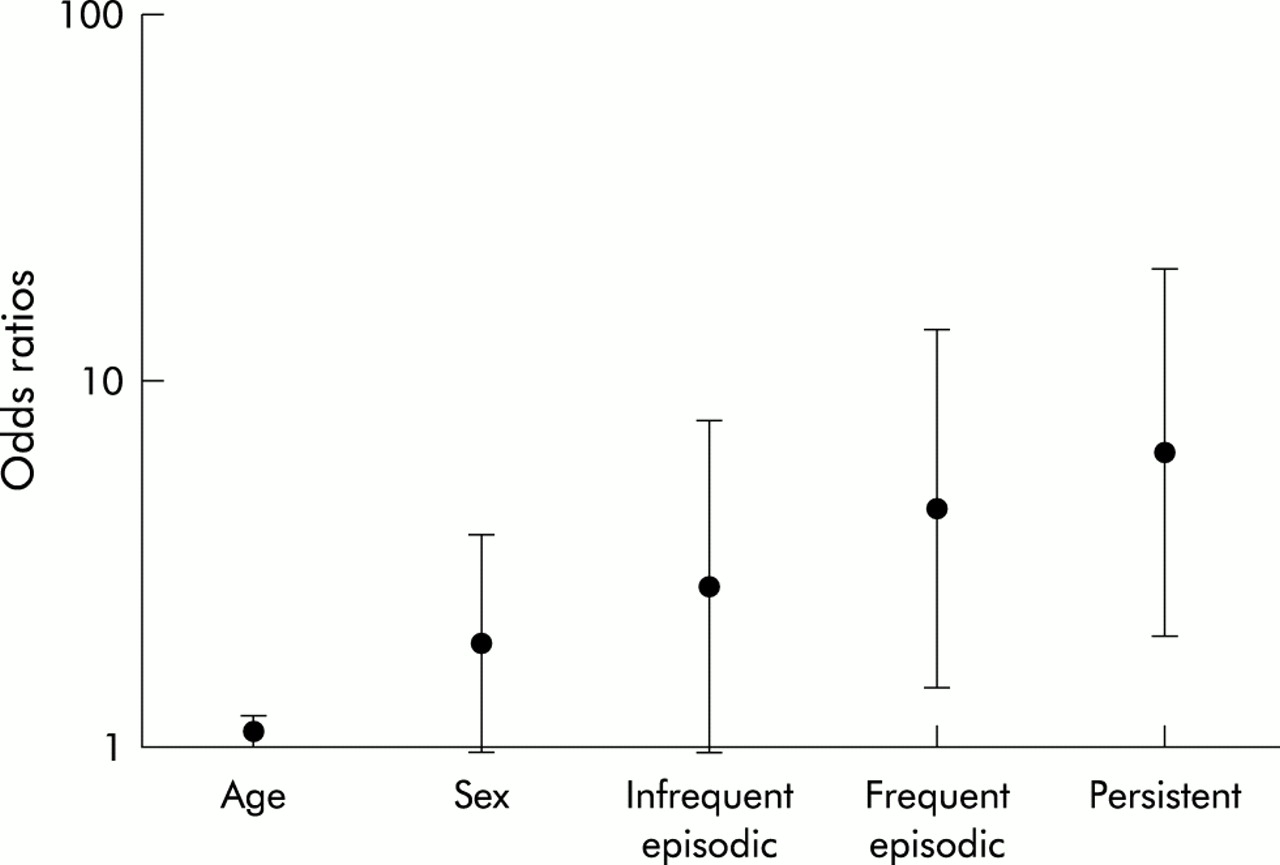
Adequate sputum samples were obtained from 78% of children. These samples were of good quality (quality score 6/6, IQR 5,6) and had minimal squamous contamination (median 16%, IQR 3,40) with no differences in these parameters between subject groups (table 2, p>0.05). Children with asthma had higher levels of eosinophils than controls (p<0.05). Other parameters were similar between asthmatic and control children. With increasing clinical asthma there was a significant increase in sputum eosinophils (fig 1, p=0.002) and sputum eosinophil cationic protein (ECP; p=0.003, table 2). Sputum eosinophils and ECP were also significantly increased in persistent asthma and frequent episodic asthma compared with controls. Children with persistent asthma had significantly increased levels of desquamated bronchial epithelial cells (table 2, p=0.04 v controls). Children with infrequent episodes of asthma had similar cell counts to healthy controls (p>0.05). Mast cells were uncommon, being present in 11% of children with asthma and 5% of healthy controls (p=0.66). Increasing treatment intensity was also associated with increasing airway inflammation, specifically an increase in sputum eosinophils and desquamated bronchial epithelial cells, (p<0.05, table 3). In a regression analysis to assess determinants of increased sputum eosinophils, the odds of sputum eosinophilia increased with increasing clinical asthma (odds ratio (OR) infrequent episodic asthma 2.72; frequent episodic OR 4.49; persistent asthma OR 6.35, fig 2) and with increasing treatment intensity (p=0.0005, table 4).
Induced sputum results and clinical asthma pattern
Induced sputum results and asthma treatment
Multiple logistic regression for determinants of sputum eosinophilia in childhood asthma (n=171)

Sputum eosinophils (%) for clinical asthma pattern. Bars are medians; *p<0.05 v persistent.
{kind=link}
{kind=link}
Log odds (95% CI) of increased eosinophils for asthma pattern.
Children with currently symptomatic asthma (n=64) had significantly increased eosinophils (p=0.05), ECP (p=0.011), and desquamated bronchial epithelial cells (p=0.04, table 5) compared with asymptomatic children, irrespective of clinical asthma grouping. Airway responsiveness and lung function were similar in symptomatic and asymptomatic children (p>0.05, table 5).
Asthma variables and current (past 2 weeks) asthma symptoms
There were no significant correlations between sputum eosinophils and FEV1 (r=−0.08) or degree of airway responsiveness (r=0.22).
DISCUSSION
In this study we have established that, as background clinical asthma increases, there is an increase in the degree of sputum eosinophilia, sputum ECP, and desquamation of bronchial epithelial cells. Airway hyperresponsiveness to hypertonic saline was both more common and more severe with increasing clinical asthma. In addition, the intensity of asthma treatment that was required showed a similar association with increasing sputum eosinophilia.
We undertook a number of measures to ensure a valid assessment of the relationship between clinical asthma and airway inflammation. Firstly, a large number of children were studied to allow sufficient numbers for multivariate analysis and to avoid the possibility of a type 2 error. Children were recruited from primary care as well as from specialist clinics in order to obtain a group with a range of asthma. Airway inflammation was assessed using the non-invasive but valid technique of sputum induction2,7,8,10 which was well tolerated and successful in this group of children. Airway hyperresponsiveness was assessed by hypertonic saline. This is an indirectly acting stimulus that correlates with the degree of airway epithelial inflammation in asthma,11 particularly airway mast cells.5,11 The nebulisation time varied, depending on the FEV1 response, and in each child was less than 8 minutes. Variations in nebulisation times over 15–20 minutes are reported to alter sputum neutrophils, but not eosinophils. The varying nebulisation time is unlikely to have influenced the results of this study since the primary outcome measure was sputum eosinophils, and we used shorter nebulisation times than are known to affect cell counts.
There are several different ways to assess clinical asthma.12 These include the frequency of wheezing episodes over the past 12 months, current (past week) symptom control, maintenance treatment requirements, lung function measures such as FEV1 or airway hyperresponsiveness, and composite measures as used in adult asthma guidelines. In this study the pattern of clinical asthma was assessed using the frequency of symptomatic episodes over the past 12 months. This classification corresponds with the current paediatric asthma management guidelines1 and other published reports.9,13 Studies in adults that have assessed asthma using similar methods also found that clinical asthma correlated with airway inflammation.14 No previous paediatric studies have used this assessment technique when relating clinical asthma to airway inflammation. In one study there was a tendency to a relationship between sputum eosinophils and clinical asthma assessed using a composite severity score.8
In adults several studies have reported a relationship between inflammatory cells and the degree of airflow obstruction measured by FEV1 or FEV/VC ratio.10,15–17 In children no such relationship was found (in this study or previously2). This may be because FEV1 is near normal in most children with asthma, except during an exacerbation. In the current study 94.5% of children with asthma had an FEV1 >80% predicted. When lung function is reduced, as occurs in a severe asthma exacerbation18 or in severe chronic asthma,4,8 then sputum eosinophils are correlated with the degree of airflow obstruction. Airway hyperresponsiveness has been found to be weakly associated with sputum inflammation in some5,10,16,17 but not all studies.15,19
The relationship between asthma treatment and airway inflammation has been assessed in three studies. Two studies which used type of treatment (inhaled corticosteroid (ICS) v no ICS) failed to find a relationship between treatment requirements and airway inflammation,2,4 whereas another study found that sputum eosinophil levels were lower in children taking ICS than in non-ICS users.20 In our study we included children with a range of treatment intensities, from none to ICS through to oral corticosteroids. Using this approach, we found that ICS use was positively associated with airway inflammation. Since the outcome variable (sputum eosinophils) was represented as a categorical variable, the regression model examined the association between ICS use and the presence of sputum eosinophilia. Children with more frequent episodes of asthma are more likely to be treated with ICS (table 1). While this improves clinical asthma and may reduce sputum eosinophils, it is not established that sputum eosinophils are reduced to the normal range by this treatment. Indeed, our earlier study found persistent sputum eosinophilia in children treated with high doses of ICS.6 The degree to which airway inflammation responds to corticosteroids, both within and between patients, is an important issue that needs to be addressed in future studies.
We have also examined the relationship between current symptoms and airway inflammation. Earlier we reported on the relationship between sputum eosinophils and current symptom control (past 2 weeks) in a group of children recruited from specialist clinics.6 These children had predominantly persistent asthma. Although there was a tendency for increased eosinophils with increasing symptom levels, the relationship failed to reach statistical significance. The results of the present study, in a larger group of children with episodic as well as persistent asthma, indicate that currently symptomatic children had significantly higher degrees of sputum eosinophils, ECP, and bronchial epithelial cells than asymptomatic children. However, there was a considerable overlap between the groups and, at an individual level, there is a poor relationship between symptom free days and sputum eosinophils in children recruited from a hospital based paediatric respiratory clinic.2,4 Other studies have also cautioned against using current symptoms to assess severity21 and adjust treatment.22 This suggests that, while airway inflammation is a determinant of current symptomatic asthma, the relationship is less strong than for the pattern of asthma over the previous 12 months. An important corollary of this that needs prospective study is the possibility that suppression of eosinophilic inflammation may be required to achieve current symptom control.
In addition to eosinophilic inflammation, we observed that the proportion of bronchial epithelial cells in the sputum of children with asthma increased as clinical asthma status increased. Bronchial epithelial desquamation is classically recognised as the presence of Creola bodies in sputum.23 The epithelium is now considered a major focus of airway damage in asthma. Epithelial loss occurs when the desmosomal connections between basal and columnar epithelial cells are disrupted,24,25 and this can be induced by eosinophil granule proteins.26 Increased bronchial epithelial cells have been reported in persistent asthma,6 with environmental exposure to mite allergen,27 with late asthmatic responses during allergen challenge,23,28 and during acute severe exacerbations of asthma.18 This is the first study to relate epithelial desquamation to the pattern of asthma in children. Boulet has previously correlated epithelial loss with the degree of airway remodelling (subepithelial fibrosis) in asthma.29 Our observations of increasing eosinophilic inflammation and ECP with increasing clinical asthma provide a mechanism for the increased sputum epithelial cells in frequent and persistent asthma, and indicate ongoing airway damage in these conditions.
In conclusion, we have shown that the clinical pattern of asthma is related to the degree of airway inflammation and that, as background clinical asthma status increases, there is increasing airway inflammation that is characterised by sputum eosinophilia and bronchial epithelial desquamation. The results support the assessment of asthma by frequency of wheezing episodes over the past 12 months when determining anti-inflammatory treatment requirements, and indicate that current symptoms are less closely related to sputum eosinophilia. These observations validate the severity assessment recommended in current asthma guidelines and identify an opportunity for the use of induced sputum when currently symptomatic patients are not controlled by initial treatment.
Acknowledgments
This study was funded by the National Health and Medical Research Council of Australia.