Article Text

Abstract
Background: Malignant pleural mesothelioma is an aggressive neoplasm with a highly variable course. This pilot study evaluated the significance of the pattern, intensity and kinetics of 18F-FDG uptake in mesothelioma in the context of histopathology and surgical staging.
Methods: Sixteen consecutive patients with pleural disease on CT scan underwent 18F-FDG imaging. Imaging was performed with a dual detector gamma camera operating in coincidence mode. Semiquantitative image analysis was performed by obtaining lesion-to-background ratios (18F-FDG uptake index) and calculating the increment of 18F-FDG lesion uptake over time (malignant metabolic potential index (MMPi)).
Results: Twelve patients had histologically proven malignant mesotheliomas (10 epithelial, two sarcomatoid). Thirty two lesions were positive for tumour. Patterns of uptake matched the extent of pleural and parenchymal involvement observed on CT scanning and surgery. Mean (SD) 18F-FDG uptake index for malignant lesions was 3.99 (1.92), range 1.5–9.46. Extrathoracic spread and metastases had higher 18F-FDG uptake indices (5.17 (2)) than primary (3.42 (1.52)) or nodal lesions (2.99 (1)). No correlation was found between histological grade and stage. The intensity of lesion uptake had poor correlation with histological grade but good correlation with surgical stage. 18F-FDG lesion uptake increased over time at a higher rate in patients with more advanced disease. The MMPi was a better predictor of disease aggressiveness than the histological grade.
Conclusions: This pilot study suggests that the pattern, intensity, and kinetics of 18F-FDG uptake in mesothelioma are good indicators of tumour aggressiveness and are superior to the histological grade in this regard.
- Keywords: mesothelioma
- 18F-fluorodeoxyglucose
Statistics from Altmetric.com
Malignant pleural mesothelioma is an aggressive primary neoplasm of mesothelial cell origin with an estimated annual incidence of approximately 2000 newly diagnosed cases in the United States,1,2 and a median survival rate of 4–12 months.3
A limited number of reports have been published addressing the use of 18F-fluorodeoxyglucose (18F-FDG) and full ring positron emission tomography (PET) for the metabolic assessment of malignant pleural mesothelioma.4–718F-FDG-PET has been shown to accurately differentiate benign pleural based lesions from malignant mesothelioma, and to be useful in the staging and preoperative evaluation of disease extent.5 We have recently demonstrated the high sensitivity, specificity, and accuracy of 18F-FDG dual detector gamma camera coincidence imaging (18F-FDG-CI) for the detection and assessment of disease extent in malignant pleural mesothelioma.8
Malignant pleural mesothelioma is characterised by local invasion of the pleural space followed by spread to intrathoracic and extrathoracic organs. The natural course of the disease is highly variable. Sarcomatoid variants tend to have a worse prognosis than the epithelial subtype.9–11 We have observed that 18F-FDG lesion uptake tends to be higher in those patients with more advanced locoregional disease and extrathoracic spread, regardless of the histological subtype. We therefore sought to study the metabolic significance of 18F-FDG uptake as it relates to tumour aggressiveness through correlation between the pattern, intensity and kinetics of 18F-FDG uptake with histopathological grade and surgical stage in patients with malignant pleural mesothelioma.
METHODS
Patients
Sixteen consecutive patients (12 men) of median age 60 years (range 37–74) with CT scan evidence of malignant pleural mesothelioma (pleural thickening, fluid, plaques or calcification) underwent 18F-FDG imaging as part of their diagnostic workup. In nine of these patients the 18F-FDG-CI scan was obtained during their initial clinical evaluation to determine the presence of malignancy and the extent of disease. In the other seven patients scanning was performed to evaluate tumour recurrence.
18F-FDG coincidence imaging
Imaging was performed with a dual detector gamma camera (ECAM Duet, Siemens Medical Systems Inc, IL, USA) equipped with 2.54 cm thick sodium iodide crystals and two-dimensional axial shields operating in coincidence mode. The axial field of view was 38 cm. The analyser was set with a single 30% window centred around the 511 keV photopeak for 18F. Images were acquired for 64 projections (with a 128 × 128 matrix) at 25 seconds per stop through a circular orbit of 180° per detector. The total acquisition time per bed position was approximately 27 minutes and decay correction was applied. The intrinsic resolution was ⩽5.3 mm full width half maximum (FWHM) at the centre and the reconstructed resolution was 4.7 mm FWHM. The sensitivity of the system with two-dimensional axial shields was in the order of 30 kcps/37 kBq/ml (30 kcps/μCi/ml) (where kcps = kilocounts per second). The maximum single counting rate per detector was 2.0 Mcps.
After fasting for at least 6 hours, capillary blood glucose levels were measured on all patients. Mean serum glucose levels were 107 (21) mg/dl (range 90–159). Eleven patients were imaged 1.5–2 hours after the intravenous administration of 370 MBq 18F-FDG. All patients were encouraged to void the bladder before imaging and scans were obtained from the proximal thighs to the base of the skull in two bed positions. The remaining five patients underwent serial imaging. Initial chest and upper abdomen scans were acquired at 45 minutes (42–65) after the injection and then repositioned for whole body imaging starting at the pelvis. In this protocol the second image of the chest and upper abdomen was acquired at approximately 2 hours (104–131 minutes) after radiotracer administration.
Images were reconstructed using an ordered subset expectation maximisation iterative algorithm.12 Reconstruction involved an order subset of four with six iterations followed by three-dimensional smooth filtering. Random subtraction and axial normalisation were performed. The system did not have the capability to correct for attenuation. Processed data were then displayed in the transaxial, sagittal, and coronal planes and displayed in the computer screen for interpretation. The results of 18F-FDG scans were then compared with conventional imaging, histopathological diagnosis, and with surgical staging.
Image analysis
Image interpretation was visual and semiquantitative. A scan was considered positive if a focal or linear, diffuse or heterogeneous pattern of increased 18F-FDG uptake was present compared with the normal surrounding background.
The degree of 18F-FDG activity in each lesion (18F-FDG uptake index) was analysed semiquantitatively by obtaining lesion-to-background ratios. Tumour average counts per pixel were obtained from regions of interest (ROI) drawn on the slice in which the lesion had the highest radioactivity concentration. Background average counts per pixel were obtained from a mirrored ROI drawn on the contralateral normal lung field.
Semiquantitative assessment of 18F-FDG kinetics was performed by calculating the tumoural 18F-FDG uptake index at 45 minutes and at 2 hours after the injection. The relative increment of 18F-FDG uptake over time in a given lesion was defined as the tumoural malignant metabolic potential index (MMPi) and was calculated as follows:

Histopathology
Within 1 week of the completion of the imaging studies, specimens were obtained from needle biopsy, thoracoscopy, pleuroscopy, cytological examination of pleural fluid, or mediastinoscopy. Tissue samples were also collected during pleurectomy or extrapleural pneumonectomy procedures. The following criteria were used to diagnose histological subtypes of diffuse mesotheliomas:13 (a) epithelial type: characterised by tubulopapillary, tubuloglandular, lace-like, cleft-like, or cord-like patterns and loss of cellular cohesion with polygonal or round cells distributed on a myxoid stroma or on the surface of mucinous pools; (b) fibrous or sarcomatoid type: a diffuse and pleomorphic spindle cell pattern with occasional giant cells in areas of necrosis, hyalinisation, and fibrosis; and (c) mixed or biphasic type: consisting of a mixture of sarcomatoid and epithelial components. Differentiation from adenocarcinoma or from other primary or metastatic epithelial neoplasms relied upon a typical staining pattern: (alcian blue +; periodic acid-Schiff-diastase −) and immunohistochemical characteristics (cytokeratins: AE1/AE3 +; calretinin +; and carcinoembryonic antigen, Leu-M1, and TTF-1 −).
Histological grading of lesions was based on the following criteria:
-
well differentiated (H1): uniform cells with low nuclear/cytoplasmic ratio and rare mitotic figures;
-
moderately differentiated (H2): moderately increased nuclear/cytoplasmic ratio, occasional mitotic figures;
-
poorly differentiated (H3): solid sheet-like pattern, high nuclear/cytoplasmic ratio, moderate nuclear pleomorphism with prominent nucleoli, frequent mitotic figures;
-
very poorly differentiated (H4): solid sheet-like pattern or small clusters or cords, high nuclear/cytoplasmic ratio, marked nuclear pleomorphism with prominent nucleoli, frequent mitotic figures with occasional abnormal mitoses.
Surgical staging
Patients were staged based on the revised Brigham and Women’s Hospital surgical staging system for malignant pleural mesothelioma.10,14 This system considers resectability, tumour histology, and nodal status, and includes four stages as follows:
-
Stage I: disease confined within the capsule of the ipsilateral parietal pleura without adenopathy, lung, pericardium, diaphragm, or chest wall disease limited to previous biopsy sites.
-
Stage II: same as stage I with positive resection margins and/or positive intrapleural lymph nodes.
-
Stage III: local extension of disease into chest wall or mediastinum; heart, or through the diaphragm, peritoneum; with or without extrapleural lymph node involvement.
-
Stage IV: distant metastatic disease.
Stage III and IV tumours were considered unresectable.
Statistical analysis
Data are presented as mean (SD). Statistical correlation between 18F-FDG uptake index, histological grade, MMPi, and surgical stage were performed using Spearman rho rank correlation (rs) analysis. p values of <0.05 were used to define statistical significance.
RESULTS
Twelve out of 16 patients had histologically proven malignant mesotheliomas (10 epithelial and two sarcomatoid). Biopsy specimens were taken from 37 lesions and, of these, 32 were found to be positive for tumour (28 epithelial and four sarcomatoid). 18F-FDG imaging was positive in all 12 patients with the disease, and the absence of disease was confirmed in the four patients who were tumour free (with histological diagnoses of chronic fibrosing pleuritis in two, chronic inflammatory response to talc pleurodesis in one, and foreign body cell reaction in one patient with a history of asbestosis).
Patterns of lesion uptake
Different patterns of 18F-FDG uptake were observed: focal/linear, diffuse and heterogeneous (fig 1). Patterns of uptake closely matched the extent of pleural and parenchymal involvement observed in CT scanning and surgery. Tumours with focal or linear patterns of uptake tended to be at an earlier stage than those with diffuse and/or heterogeneous 18F-FDG distributions, regardless of histological type or grade. In patients with advanced pleural involvement the pattern of uptake was usually diffuse, involving one or more aspects of the pleura, or heterogeneous, encasing the lung with or without extension to the lung parenchyma.

Patterns of 18F-FDG uptake in malignant pleural mesothelioma: (A) focal, (B) linear, (C) diffuse, and (D) heterogeneous.
Intensity of lesion uptake
The mean (SD) 18F-FDG uptake indices in malignant lesions and in normal lung were 3.99 (1.92), range 1.5–9.46 and 1.09 (0.04), range 1.06–1.12, respectively. The intensity of lesion uptake correlated poorly with histological grade (rs = 0.56, p = 0.035) but had a good correlation with disease extent as defined by the surgical stage (rs = 0.78, p = 0.002; fig 2A and B). No correlation was found between histological grade and surgical stage (rs = 0.10, p = 0.80).

(A) Relationship between the FDG uptake index and the histological grade. (B) Correlation between the highest FDG uptake index per patient and surgical stage.
Extrathoracic spread and metastatic lesions had significantly higher 18F-FDG uptake indices (5.17 (2)) than primary (3.42 (1.52)) or nodal lesions (2.99 (1); p = 0.02).
Primary lesions were more 18F-FDG avid in patients with distant spread than in those without extensive disease, although considerable overlap of uptake values was observed. Recurrent lesions were more 18F-FDG avid (5.25 (2.65)) than lesions detected during initial staging (2.05 (0.88); p = 0.05, fig 3).

Distribution of 18F-FDG indices in recurrent and early stage lesions.
18F-FDG kinetics
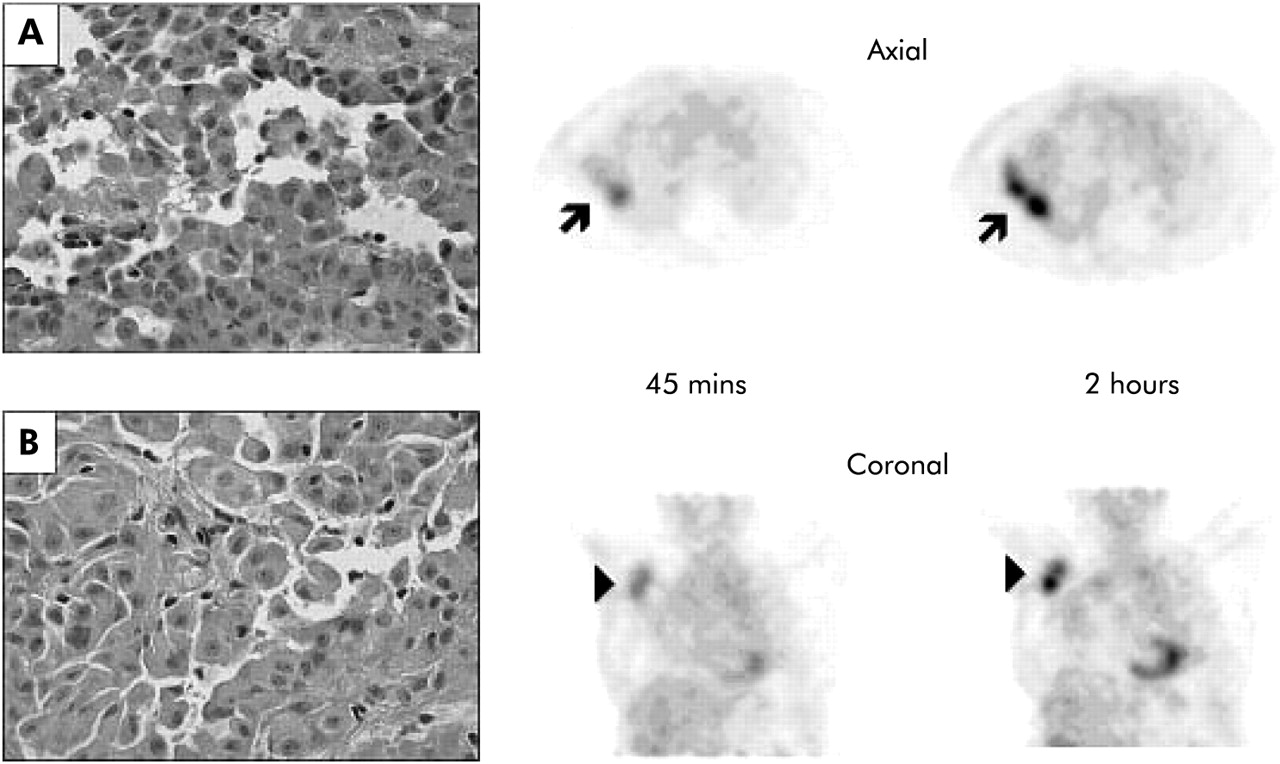
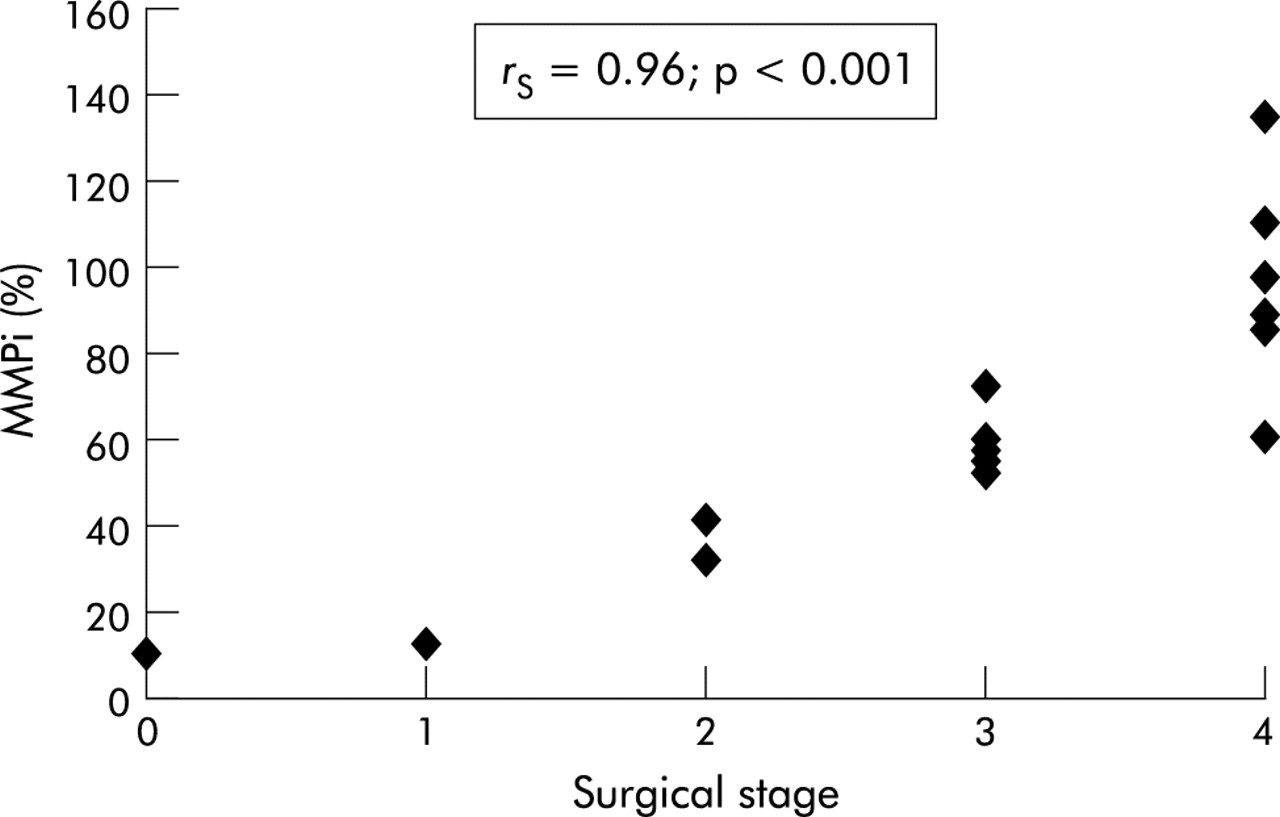
Semiquantitative analysis of serial images showed that 18F-FDG uptake increased minimally in normal tissue over time, but had a much larger increase in malignant lesions. In normal lung the mean (SD) increment in FDG uptake was 6 (4)% between early and late images. The increment of 18F-FDG uptake in malignant lesions (malignant metabolic potential index, MMPi) was highest in stage IV patients (97 (25)%) compared with patients with stage I (13 (1)%), stage II (34 (2)%), and stage III (57 (3)%) disease (fig 4). There was a positive exponential relationship between the MMPi and the surgical stage (rs = 0.96, p<0.001), with extrathoracic spread and metastases invariably more metabolically active than primaries (fig 5).

(A) Poorly differentiated right pleural mesothelioma and (B) very poorly differentiated axillary metastasis from a patient with surgically confirmed stage IV disease. Axial and coronal 18F-FDG images show increased glycolytic activity over time in both the right pleural primary (arrow) and in the axillary metastasis (arrow head) with malignant metabolic potential indices (MMPi) of 90% and 135%, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Increment of FDG uptake as a function of time (MMPi) and surgical stage.
DISCUSSION
The findings of this pilot study were as follows:
-
The patterns of 18F-FDG uptake matched the extent of pleural and parenchymal disease observed in conventional imaging and correlated well with the overall tumour burden observed during surgery.
-
The intensity of 18F-FDG uptake proved to be a better marker of disease aggressiveness than the histological grade of the tumour.
-
Transdiaphragmatic spread and metastases were more 18F-FDG avid than primary lesions regardless of the histological grade.
-
Primary lesion uptake tended to be higher in those patients with more extensive disease.
-
Most recurrent lesions were more 18F-FDG avid than lesions detected during earlier stages.
-
The increment of 18F-FDG uptake as a function of time was a good estimate of the aggressiveness of the lesions as defined by the surgical stage.
There was good agreement between 18F-FDG images and surgical findings. The metabolic images correctly predicted unresectability by showing the presence and extent of tumour invasion of the mediastinal organs, transdiaphragmatic spread, and distant metastatic disease. The use of 18F-FDG imaging also proved to be of value for the selection of the most metabolically active site for needle or thoracoscopic biopsy. This approach, when combined with conventional imaging techniques, increased the yield of positive biopsy specimens. The main limitation of the 18F-FDG images was the imprecise anatomical detail. It was not feasible to differentiate uptake in the parietal pleura from that in the visceral pleura in the absence of a pleural effusion. Similarly, uptake in the basal pleura could not be distinguished from diaphragmatic uptake. Diaphragmatic involvement could be unequivocally diagnosed only when transdiaphragmatic spread was evident. Focal chest wall uptake was difficult to differentiate from pleural uptake. Chest wall involvement could be unequivocally ascertained only when 18F-FDG uptake was intense and caused distortion of the thoracic contour in the images. Intrapleural node (N1) uptake had to be very intense to be differentiated from pleural uptake, especially in those patients with bulky invasive tumour affecting the hilum or mediastinum. In cases in whom the tumour invaded mediastinal organs, 18F-FDG uptake was rather diffuse and all inclusive. It was not possible to resolve uptake in individual structures.
The highest intensity of lesion uptake in any given patient had a poor correlation with histological grade but a good correlation with the surgical stage. A certain degree of overlap of 18F-FDG uptake indices was evident between disease stages, probably due to the underestimation of recovered counts arising from smaller lesions. Nevertheless, while the degree of cellular differentiation correlated poorly with the extent of tumour burden, aggressive and heterogeneous proliferation seemed to be more dependent on and directly related to glucose utilisation as measured by 18F-FDG uptake. These results are similar to those reported by Bénard and colleagues7 who found a wide variability in standardised uptake value (SUV) measurements in patients with malignant disease and showed that high levels of 18F-FDG uptake in mesothelioma were associated with an unfavourable prognosis. The mean SUV of survivors was 3.2 (1.6) compared with 6.6 (2.9) for non-survivors.
Sites of extrathoracic spread and metastases had higher 18F-FDG uptake than primary lesions with only fair correlation with the histological grade. Interestingly, uptake in primary lesions of patients with extensive disease was usually higher than in patients at lower stages. However, considerable overlap of uptake values was observed. Histopathology revealed different degrees of necrosis, acute and chronic inflammation in these lesions, all of which are known to affect 18F-FDG uptake.15,16 It is generally accepted that tumours with high metastatic potential have higher energy requirements. Our data suggest that increased glycolytic rates, reflected in increased radiotracer uptake and kinetics, may be a necessary precondition for the acquisition of metastatic potential. The degree of histological differentiation of the primary tumour did not always give a reliable estimation of tumour aggressiveness. In most cases high 18F-FDG uptake was a more reliable indicator of disease extent.
Recurrent lesions had higher 18F-FDG avidity than lesions detected during initial staging. All patients with relapse had stage IV disease and their lesions invariably had a high histological grade. The rationale behind these observations cannot be elucidated by the results of this study; but the increased use of 18F-FDG by these lesions could indicate the emergence of new and more aggressive clones with higher energy requirements.
Visual inspection and MMPi obtained from dual phase images revealed that 18F-FDG uptake increased in all malignant lesions over time, regardless of the histological type, cellular differentiation, blood glucose levels, and pretreatment or post treatment status. All lesions were better visualised with higher contrast in the late images. Some lesions that appeared equivocal in the early images became clearly evident in the late images. These findings confirm those of Kubota et al17 who showed that the tumour to background ratio dramatically improved 2 hours after injection in lung cancer lesions, as well as in mediastinal and upper abdominal malignancies.
The MMPi correlated better with the surgical stage and was a better predictor of disease extent and aggressiveness than the late 18F-FDG index alone or the histological grade. Unlike the 18F-FDG uptake index, the increment of 18F-FDG uptake as a function of time was independent of lesion size. Small lesions with low initial and late 18F-FDG uptake indices in patients with advanced disease were better categorised as metabolically active based on a considerable increase in uptake over time. The number of counts recovered from these small lesions is underestimated due to volume averaging on both scans, so their FDG indices tend to overlap with those arising from lesions at lower stages of the disease. The MMPi, on the other hand, increased at a higher rate in aggressive lesions, with each lesion serving as its own standard regardless of size. This finding is similar to that reported by Matthies et al18 in the evaluation of pulmonary nodules with dual time point 18F-FDG imaging and full ring PET technology where small lesions (1.5–2 cm) with low initial SUV could be detected on the basis of an increase in SUV over time.
In addition, as shown in fig 5, the range of MMPi values was wider at higher stages of disease. 18F-FDG uptake is a function of blood flow, facilitated transport across the plasma membrane, and the differential ratio of intracellular phosphorylation and dephosphorylation of the tracer.19–23 Thus, this difference in lesion MMPi values could represent distinct metabolic stages with lower or higher tumour glycolytic rates in patients whose anatomical staging is similar. Younes et al24 studied 289 patients with stage I non-small cell lung carcinoma and showed that tumours which overexpressed glucose transporters (Glut-1 and Glut-3) were associated with aggressive biological behaviour. Survival analysis showed that stage I patients with tumours overexpressing both transporters had worse overall survival than those patients with Glut-negative tumours. Based on these data, well and moderately differentiated tumours could be further stratified into different prognostic groups based on glucose transporter immunoreactivity. Cellular mutation, selection, and clonal expansion are responsible for the heterogeneous properties of tumour cells. Our results showed that, in malignant pleural mesothelioma, this heterogeneity could extend not only to morphology and grade but also to its metabolic properties. The clinical implications of this metabolic stage as a complement to the surgical stage and as a predictor of outcome should be fully explored, not only in mesothelioma but also in other tumour types.
Our preliminary findings provide an interesting insight into the metabolic behaviour of malignant pleural mesothelioma, but statistical power might be affected by the small sample size. We did not have the opportunity to evaluate the behaviour of 18F-FDG uptake over time in benign pleural lesions such as parapneumonic effusions and tuberculous pleuritis which have been described as moderately 18F-FDG avid and could become a source of false positive results.25 The lack of attenuation correction in our images is also a potential limitation since lesions observed in attenuation uncorrected images are subject to a certain degree of distortion, and tumour to background ratios in uncorrected images tend to be higher than those obtained in attenuation corrected images.26 However, it has been shown that there is a strong linear correlation between tumour to background ratios calculated on both sets of images (r = 0.98, p<0.001) and that the diagnostic efficacy is similar.27,28
More extensive prospective trials are needed to verify the reproducibility of our findings in this small study and to elucidate the role that metabolic staging, as defined by 18F-FDG kinetics, might play in the prediction and assessment of response to multimodality treatment and survival.
This pilot study suggests that the pattern, intensity, and kinetics of 18F-FDG uptake in malignant pleural mesothelioma are good metabolic indicators of tumour aggressiveness as measured by the surgical stage, and are superior to histological grading in this regard.