Article Text

Abstract
Background: Obesity may be associated with an increase in asthma and atopy in children. If so, the effect could be due to an effect of obesity on lung volume and thus airway hyperresponsiveness.
Methods: Data from 5993 caucasian children aged 7–12 years from seven epidemiological studies performed in NSW were analysed. Subjects were included if data were available for height, weight, age, skin prick test results to a common panel of aeroallergens, and a measure of airway responsiveness. History of doctor diagnosed asthma, wheeze, cough, and medication use was obtained by questionnaire. Recent asthma was defined as a doctor diagnosis of asthma ever and wheeze in the last 12 months. Body mass index (BMI) percentiles, divided into quintiles per year age, were used as a measure of standardised weight. Dose response ratio (DRR) was used as a measure of airway responsiveness. Airway hyperresponsiveness was defined as a DRR of ⩾8.1. Adjusted odds ratios were obtained by logistic regression.
Results: After adjusting for atopy, sex, age, smoking and family history, BMI was a significant risk factor for wheeze ever (OR = 1.06, p = 0.007) and cough (OR = 1.08, p = 0.001), but not for recent asthma (OR = 1.02, p = 0.43) or airway hyperresponsiveness (OR = 0.97 p = 0.17). In girls a higher BMI was significantly associated with higher prevalence of atopy (χ2 trend 7.9, p = 0.005), wheeze ever (χ2 trend 10.4, p = 0.001), and cough (χ2 trend 12.3, p<0.001). These were not significant in boys.
Conclusions: Higher BMI is a risk factor for atopy, wheeze ever, and cough in girls only. Higher BMI is not a risk factor for asthma or airway hyperresponsiveness in either boys or girls.
- obesity
- asthma
- children
- atopy
Statistics from Altmetric.com
In the past two decades there has been a significant increase in the prevalence of asthma, atopy, and obesity in children worldwide.1 It is possible that these events are linked.2–4
In adults, large random population studies have shown an increase in the incidence5 and prevalence6 of wheezing and diagnosed asthma in obese subjects. Furthermore, in randomised controlled trials, weight loss has been associated with improvements in asthma symptoms and peak expiratory flow rate (PEFR).7,8 While these findings strongly suggest that obesity is associated with an increase in asthma-like symptoms, it has not be established that this is due to an increase in the prevalence of asthma in obese subjects. We have shown previously that adults with severe obesity reported more wheeze and shortness of breath but that this was not associated with a higher prevalence of atopy, airway hyperresponsiveness, or airway obstruction, suggesting that the prevalence of asthma is not higher in this group.6 Other studies have shown an increase in airway responsiveness in men9 and adolescent girls,3 but these results have not been consistent.
In children, cross sectional studies of large random population samples have also shown that excess body weight is associated with a higher rate of both symptoms and diagnosed asthma.2,3,10 However, in Taiwanese teenagers obesity was associated with an increase in airway hyperresponsiveness, atopy, and atopic symptoms in girls but not boys.3 This suggests that the association between asthma and excess body weight may differ between adults and children and between boys and girls.
The association between obesity and atopy has also rarely been explored. It is possible that obesity could cause atopy or inflammation or that there is some common factor that predisposes to both obesity and atopy. The results from previous studies tend to be confusing, with one study showing that obesity was associated with an increase in atopy in girls but not in boys,3 while another study showed no association with atopy, allergic symptoms, or IgE levels in more than 15 000 young adults.11
In this paper we report an analysis of cross sectional data in a large population of caucasian Australian children. The aim was to determine if increased body weight, as measured by body mass index, is associated with a higher prevalence of asthma or atopy or with an increase in airway obstruction or airway responsiveness to histamine. We also examined whether the association between body weight, atopy, and symptoms of asthma was different between girls and boys.
METHODS
Data from seven large epidemiological studies of children aged 7–12 years conducted in seven regions of NSW, Australia between 1991 and 1993 were pooled. Details of the populations, response rates, and non-responders have been published elsewhere.11,12 Data from less than 5% of children who were non-caucasian were excluded. Children for whom height, weight, age, and airway responsiveness were measured were included.
Information on symptoms, family history, and diagnoses were collected by a parent completed questionnaire.14 Recent wheeze was defined as the presence of wheeze in the previous 12 months. Recent asthma was defined as recent wheeze plus a doctor diagnosis of asthma ever.
Lung function was recorded before and after saline inhalation using Mijnhardt VRS dry rolling seal spirometers (Mijnhardt BV, Bunnik, The Netherlands) and Scientific and Medical (S&M) data acquisition software. Forced expiratory manoeuvres were repeated until two measurements of forced expiratory volume in 1 second (FEV1) within 100 ml were obtained. The largest FEV1 was used in the analyses. Children were tested after withholding β agonist for at least 6 hours. Percentage predicted FEV1, forced vital capacity (FVC), and PEFR were calculated.15
Airway responsiveness was measured by the rapid histamine inhalation test.16 The dose of histamine that caused a 20% fall in FEV1 (PD20FEV1) and the dose response ratio (DRR; percentage change in final FEV1 from baseline divided by the total dose of histamine administered) were calculated. Because many children had an FEV1 that remained stable or improved slightly during the study, a constant of 3 was added to all DRR values to return a positive value for logarithmic conversion. Participants with a fall in FEV1 of 20% or more at ⩽3.9 μmol histamine were defined as having airway hyperresponsiveness, which is equivalent to a DRR of >8.1.
BMI was calculated by dividing weight (kg) by the square of the height (m) (kg/m2). There is no standard for weight distribution in children so we used BMI percentiles per sex per age as a measure of standardised weight.17,18 NHANES I was used as the reference population for the BMI percentiles19 as there are no reference data available for Australian children. No studies have compared distribution of overweight and obese Australian children in this age group with those in the USA. We present results as BMI percentiles corrected for age and sex. BMI percentiles divided into quintiles were used to assess the relationship between standardised weight, symptoms, and lung function. Analyses were also performed with BMI as a continuous variable and divided into overweight (BMI 85–95th percentile) and obese (BMI >95th percentile).
Statistical analysis
Data were analysed using the statistical package SPSS (Chicago, IL). Geometric mean values are reported for DRR values, which were converted to base 10 logarithms before analysis. For all analyses p values of <0.05 were regarded as significant. Pearson’s chi square (χ2) statistic and chi square trend were used to determine the significance of differences in prevalence between different BMI groups.
Logistic regression was used to compute odds ratio for outcomes in the presence of higher BMI and adjusted for family history of asthma, age, sex, atopy status, and exposure to cigarette smoke. Partial correlation and logistic regression was used to assess correlation between BMI and airway responsiveness adjusting for airway size using FVC% predicted and FEV1/FVC%.20
Linear regression was used to assess the relation between lung function and BMI percentile. One way ANOVA was used to analyse means of grouped data with Duncan’s post hoc test to limit the number of multiple comparisons.
Tests for homogeneity were performed (Meta-view in Review Manager (RevMan), Version 4.2, Update Software) between the seven regions for the prevalence of wheeze, cough and airway hyperresponsiveness.
RESULTS
Complete data were available for 5993 children. The response rates were: Belmont 82.7%, Lismore 76.8%, Sydney 76.8%, Western Sydney 75.9%, Moree 74.2%, Wagga Wagga 82.7%, and Broken Hill 80%. The proportion of participants in each group, classified according to quintiles of BMI percentile, is shown in table 1. Tests for homogeneity were performed between the seven regions and there were no significant differences in the prevalence of wheeze (χ2 = 8.42, p = 0.21), cough (χ2 = 2.99, p = 0.81), or airway hyperresponsiveness (χ2 = 4.33, p = 0.63).
Characteristics of subjects included in the study
Table 1 shows that a higher BMI was associated with a higher prevalence of atopy in girls but not boys. There was no significant association with family history of asthma for either girls or boys. Exposure to cigarette smoke had a highly significant association with a higher BMI in both girls and boys.
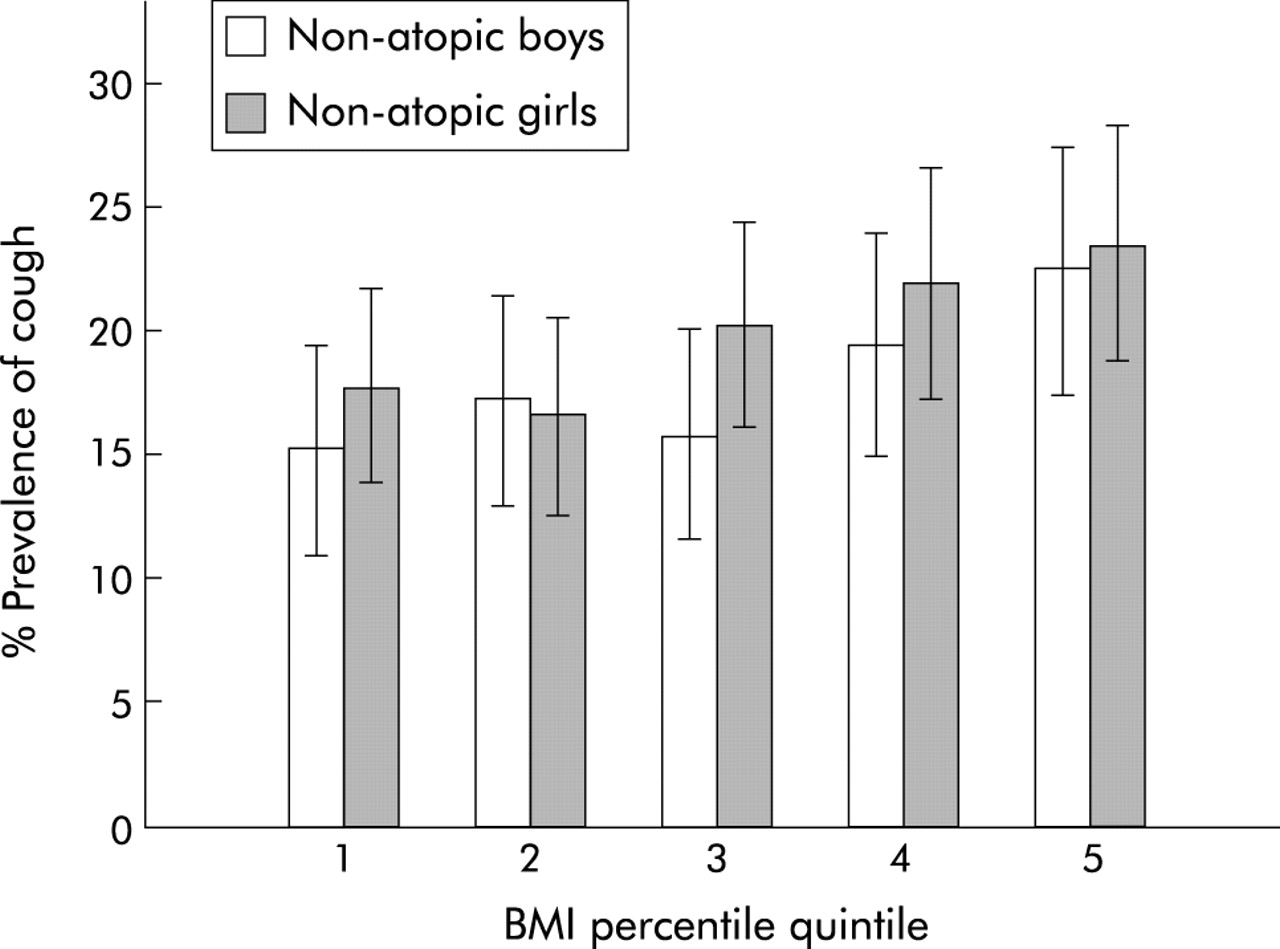
In separate analyses of data from girls and boys (table 2), a higher BMI was significantly associated with a higher prevalence of atopy, wheeze in the last 12 months, wheeze ever, cough, and the use of medication for asthma in girls but not in boys. However, there was no significant association between BMI and the prevalence of diagnosed asthma or recent asthma in either boys or girls. The association between higher BMI and cough was significant in both atopic and non-atopic boys and girls (fig 1).
Symptoms according to BMI quintile
{kind=link}
Prevalence of cough in the last 12 months in non-atopic girls and boys by BMI quintile. There was a significant increase in the presence of cough with higher BMI quintile in both non-atopic girls (p = 0.02) and boys (p = 0.02).
After adjusting for atopy, family history of asthma and exposure to cigarette smoke, a higher BMI was associated with a higher prevalence of wheeze ever, cough, and medication use for asthma (table 3). However, there was no significant association between a higher BMI and the prevalence of diagnosed asthma, recent asthma, or airway hyperresponsiveness (table 3).
Adjusted odds ratio for symptoms and airway hyperresponsiveness in comparison with the normal weight group
Table 4 shows spirometric function and airway responsiveness for girls and boys in each of the BMI quintiles. For all spirometric variables, mean values were within the predicted normal range for all of the BMI groups. In both girls and boys there were significant differences between BMI quintiles in FEV1 % predicted and FVC % predicted. Post hoc comparison showed that FEV1 % predicted and FVC % predicted were significantly reduced in the lowest quintile compared with the rest of the population measured. However, there were no differences in FEV1/FVC ratio, suggesting that low BMI was not associated with an increase in airway obstruction in girls or boys. This observation was supported in boys by the finding that there was also no difference between BMI quintiles in flow rates as measured by PEF % predicted or FEF25–75 % predicted. However, in girls there was a significant reduction in PEF % predicted and FEF25–75 % predicted between the lowest BMI quintile compared with the highest quintile. There was no significant association between BMI and either the prevalence of airway hyperresponsiveness or the severity of airway responsiveness, measured by DRR, in either boys or girls. This remained true after adjusting DRR for airway size using FVC % predicted and FEV1/FVC % (standardised coefficient β = −0.002, p = 0.89).20
Lung function according to BMI quintile
All analyses were repeated using BMI as a continuous variable, or with children categorised as normal (BMI <85th percentile), overweight (BMI 85–95th percentile), or obese (BMI >95th percentile).21–23 The results of these analyses did not differ from the original analyses.
DISCUSSION
This study confirms the findings of previous studies that a higher BMI is associated with a higher prevalence of symptoms of wheeze and cough in children. This association was stronger in girls than in boys. However, the association was independent of atopic status and there was no association between higher BMI and the presence of either airway obstruction or airway hyperresponsiveness. Neither diagnosed asthma nor the combination of diagnosed asthma and recent symptoms were associated with higher body weight.
These findings suggest that a higher BMI in children is associated with a higher prevalence of symptoms that are often attributed to asthma, but not with a higher prevalence of asthma. We found that a higher BMI in children was not associated with a higher prevalence of diagnosis of asthma, but was associated with a higher prevalence of atopy in girls but not in boys.
The distribution of BMI in these samples is similar to the general population in Australia.24 The methods and the IUATLD questionnaire were similar to those used in other large epidemiological studies and were well validated.14
This study has several potential limitations inherent in a large cross sectional group of children from seven different regions across New South Wales. Also, BMI percentiles were calculated from USA data as this information is not available currently for Australia. This is unlikely to have invalidated the study outcomes, since the trend for the increase in obesity in children in Australia is closely following the USA trend.24 Although BMI may not be the best measure of obesity in children, it is widely used and we do not have other information on which to base an alternative definition.17
The association between a higher BMI and symptoms of wheeze and cough in children has been observed in previous studies.5,6 However, wheeze and cough are non-specific symptoms which may be attributed to a number of different causes, including asthma. To confirm a diagnosis of asthma in children presenting with a history of wheeze or cough, it would usually be necessary to find evidence of variable airway obstruction. In this population the increased prevalence of wheeze and cough associated with increased BMI was not associated with any higher prevalence of airway obstruction or airway hyperresponsiveness. This suggests that the excess symptoms among overweight children may be due to causes other than asthma. Increased BMI is associated with an increase in the occurrence of both gastro-oesophageal reflux25 and sleep apnoea,26 and both of these conditions may be a cause of symptoms of wheeze or cough without changes in lung function or airway responsiveness.
Alternatively, increased BMI may be associated with a number of changes to the mechanical function of the lungs and airways that could lead to symptoms of wheeze and cough. Other studies have shown that a higher BMI is associated with a higher rate of wheeze with exercise.10 In this study we did not collect information that allowed us to differentiate between wheeze at rest and wheeze with exertion, so we cannot determine the extent to which the excess wheezing in our overweight subjects was due to wheeze during exercise. Exertional wheeze in overweight subjects may be due to an increase in the work of breathing, with upper airway collapse or changes in lung mechanics increasing the load on the upper airway. Other studies have shown an increase in airway resistance in obese subjects,27 and wheeze may be due to changes in airway calibre, collapsibility, or inability to overcome airway hysteresis.
Changes in compliance or elastic recoil resulting from low lung volume could decrease the tidal fluctuations of airway smooth muscle and enhance contractility,28 and thus shift the dose response curve or increase the level of the maximal response.29 We found no evidence of lower flow rates or higher airway hyperresponsiveness in the highest quintile. Although we have shown previously that FVC is reduced in obese adults,6 we did not find a significant reduction in FVC in children in the highest BMI quintile. We did not measure lung volumes and therefore it is not clear whether the effects of obesity on lung volume are not as prevalent in children as in adults or are less prominent if a higher body weight is present before puberty. Further studies are required to look at lung volumes in obese children and changes with puberty.
Although inhaled corticosteroid medication can normalise lung function and airway responsiveness,30 it is unlikely that the use of such medication could account for the absence of any association between a higher BMI and increased airway obstruction or airway hyperresponsiveness since there was only a slight trend to a higher rate of medication use with higher weight. Furthermore, it is unlikely that symptoms would persist during inhaled corticosteroid medication treatment if airway hyperresponsiveness or airway obstruction had been normalised.
A previous study found that increased BMI is associated with a higher prevalence of atopy and symptoms of wheeze in girls but not in boys, which our study confirms.3 The cause for this is unknown and may relate to differences in hormonal levels, inflammatory markers, or body fat distribution. A correlation between BMI and airway hyperresponsiveness was found in Taiwanese girls,3 whereas another large study showed this association in men only.9 Our study does not confirm this since we found that BMI was not correlated with airway responsiveness, measured by DRR, nor was higher BMI associated with increased prevalence of airway hyperresponsiveness in either boys or girls.
Our study has significant clinical implications. Previous studies have shown higher rates of diagnosed asthma in obese children.2,3,10,31–33 However, without evidence of airway obstruction or airway responsiveness, it is unlikely that these children truly have asthma. It is important to elucidate the true aetiology of symptoms in overweight children. Increasing symptoms with higher weight may be the result of being unfit, worsening asthma, gastro-oesophageal reflux, or sleep disordered breathing. The treatment options for these aetiologies vary markedly. Some may require inhaled or even oral corticosteroids which, if used indiscriminately, may exacerbate the weight problem. Others may be more likely to benefit from a weight loss programme, H2 blockers, or even nasal continuous positive airway pressure.
It is unlikely that a higher BMI is a risk factor for asthma or airway hyperresponsiveness in children, and it is likely that the prevalence of asthma in obese children is the same as in the rest of the population. Obesity and asthma are both significant health problems and must be addressed in both children and adults to optimise lung function and quality of life.
REFERENCES
Linked Articles
- airwaves