Article Text

Abstract
Background: Until now, care provided by asthma nurses has been additional to care provided by paediatricians. A study was undertaken to compare nurse led outpatient management of childhood asthma with follow up by a paediatrician.
Methods: Seventy four children referred because of insufficient control of persistent asthma were randomly allocated to 1 year follow up by a paediatrician or asthma nurse. The main outcome measure was the percentage of symptom-free days. Additional outcome measures were airway hyperresponsiveness, lung function, daily dose of inhaled corticosteroids (ICS), number of exacerbations, number of additional visits to the general practitioner, absence from school, functional health status, and disease specific quality of life.
Results: There were no significant differences at the end of the 1 year study period between the two treatment groups in percentage of symptom-free days (mean difference 2.5%; 95% CI −8.8 to 13.8), airway hyperresponsiveness (log10 PD20 0.06; −0.19 to 0.32), functional health status (10.1; −0.3 to 19.8), disease specific quality of life of patients (0.08; −0.9 to 0.7), and disease specific quality of life of caregivers (0.09; −0.2 to 0.3), nor in any other outcome parameters. Most outcome parameters improved considerably over the 1 year study period. These improvements were achieved although the daily dose of ICS was reduced by a mean of 26% compared with the dose received by children at referral. All parents were satisfied with the asthma care received.
Conclusions: After initial assessment in a multidisciplinary clinic, childhood asthma can be successfully managed by an asthma nurse in close cooperation with a paediatrician. During close follow up by paediatrician or asthma nurse, asthma control improved despite a reduction in ICS dose.
- asthma
- children
- outpatient management
- paediatricians
- asthma nurses
Statistics from Altmetric.com
According to international guidelines, education of patients and their parents is important in the long term management of childhood asthma.1,2 Comprehensive education not only reduces morbidity, emergency visits, and hospital admissions,3–9 but also improves quality of life.3,10,11 Asthma nurses are commonly employed to provide this important time consuming task.12–15
Follow up in asthma management consists, to a considerable degree, of reinforcement of the patient’s and parents’ knowledge of the disease, ensuring adherence to the management plan, checking the inhalation technique, and adjustment of the medication according to symptoms of asthma. In principle, all these tasks can be performed by asthma nurses.
Until now, care provided by asthma nurses has been additional to medical care by physicians. Recent evidence suggests that adults with selected chronic diseases can be managed successfully by nurses alone.16–20 We designed a randomised trial to establish whether there are differences in efficacy between outpatient management of childhood asthma by paediatricians or by asthma nurses.
METHODS
Patients
Patients aged 2–16 years newly referred by their general practitioners to the outpatient clinic of the Isala Klinieken (a 1100 bed district general hospital) by general practitioners for chronic persistent asthma were asked to participate in the trial. The patients were categorised as having mild, moderate, or severe asthma based on international guidelines.1 We chose to exclude patients under 2 years of age because many patients in this age group wheeze recurrently without having a definite diagnosis of asthma.21
All patients were prescribed inhaled fluticasone propionate as maintenance therapy and inhaled salbutamol as needed. The initial dose of fluticasone chosen was dependent on the dose prescribed by the general practitioner and the reported response to it. These drugs were prescribed by dry powder inhaler (Diskus, GlaxoSmithKline) or by metered dose inhaler plus spacer (Volumatic, GlaxoSmithKline), depending on their age.22
Patients were not eligible to enter the study if the daily dose of fluticasone propionate required to control their asthma exceeded 500 µg (or equivalent doses of beclomethasone or budesonide), if maintenance oral steroids were needed, or if they suffered from a concomitant disease that warranted follow up by a paediatrician. Written informed consent was obtained from patients (>12 years of age) and from all parents. The study was approved by the ethics committee of the Isala Klinieken.
Initial work up
The initial diagnostic work up for all patients included a full medical history and physical examination by one of the two consultant paediatric pulmonologists (PLPB and RJR). Spirometric tests for children ⩾5 years of age were performed according to European Respiratory Society guidelines23 with a Jaeger Masterlab pneumotachograph (Jaeger Toennies, Breda, The Netherlands). Expiratory flow-volume curves were recorded and the forced expiratory volume in 1 second (FEV1) was taken from the best of three reproducible manoeuvres and expressed as a percentage of the predicted value (FEV1%pred).24 The bronchodilator response (BDR) was expressed as the difference between FEV1%pred measured before and 20 minutes after inhaling 800 µg salbutamol via a metered dose inhaler plus spacer device (Volumatic spacer). Methacholine challenge was performed using a dosimeter method as published previously and expressed as PD20 (dose of methacholine at which FEV1 falls 20% from baseline).25
In all children allergy to common inhalant allergens was assessed by radioallergosorbent test (RAST) or skin prick test unless this had been performed in the 6 months before inclusion in the study.
Education session
An asthma nurse conducted a detailed education session with the patient and his or her parents, discussing information about the mechanisms and triggers of the disease, use of controller and reliever medication, management of acute symptoms, when to seek medical advice, and advice on environmental avoidance. Proper inhalation technique was instructed carefully and checked repeatedly until the asthma nurse was satisfied with the patient’s inhalation technique.
Randomisation
Patients were randomly assigned to follow up by either a paediatrician or an asthma nurse. Randomisation was performed using random number tables. Patients were followed up by the same healthcare provider throughout the study.
Follow up
Patients were seen at regular intervals (1, 3, 6, and 12 months after the start of the study). Additional follow up visits were planned individually if needed according to the judgement of the paediatrician or the asthma nurse. The educational issues described above were addressed at each follow up visit according to a checklist. The duration of the follow up visits was recorded. At the end of the study all patients were seen by the paediatrician.
The nurse led asthma care was provided by two experienced, board certified asthma nurses (AO and LvH). The asthma nurse was able to consult the paediatrician at all times to discuss medical issues of patients under her care.
Adjustment of medication
At each visit, after evaluation of the level of asthma control, predefined adjustments of medication were made according to a protocol. The initial dose of fluticasone was maintained during the first 3 months of the study if adequate control (few symptoms, minimal use of rescue medication (⩽3 times per week according to the diary), and no exacerbation of asthma in the last month) of the patient’s asthma was achieved. At subsequent visits the dose was tapered off to the lowest effective dose required to maintain control. If the patient’s asthma was considered to be inadequately controlled (frequent use of rescue medication, frequent or severe exacerbations of asthma), the dose of fluticasone was doubled. In the remaining cases the dose of fluticasone was continued. No long acting β2 agonists were applied following Dutch guidelines for maintenance therapy of asthma valid at the time of the study.26
If asthma control could not be achieved with fluticasone 500 µg/day for patients treated by an asthma nurse, the patient was withdrawn from the study.
Data collection
Spirometric tests were performed at each regular follow up visit and methacholine challenge at the end of the study period. Patients (or their parents) were asked to record symptoms on a 4-point scale (0=no symptoms, 1=mild symptoms, 2=moderate symptoms, 3=severe symptoms) and use of rescue medication in a diary for 2 weeks preceding each visit. Information about asthma related absence from school (patients ⩾4 years) and extra visits to the general practitioner because of respiratory symptoms was also obtained from the patient’s diary and double checked at each follow up visit. At the end of the study parents completed a short questionnaire on their satisfaction with the asthma care received.
Outcome measures
The primary outcome measure was the difference in percentage of symptom free days between the two treatment groups. Secondary outcome measures were lung function, airway hyperresponsiveness, dose of inhaled corticosteroids, use of rescue medication, absence from school, extra visits to the general practitioner, disease specific quality of life, and functional health status.
Functional health status
The functional health status of the children was assessed at baseline, after 6 months, and at the end of the study. Two validated questionnaires were used—namely, the Dutch parental versions of the Functional Status II (FSII) and the RAND general health rating index.27,28 The FSII generic questionnaire consists of 14 questions about the child’s behaviour during the previous 2 weeks and the effect of disease on it. The cumulative score lies between 0 and 100, with 100 indicating no behavioural problems. The RAND general health rating index is a 7 item questionnaire. The cumulative score of the items is between 7 and 32. A higher score indicates a better health status.
As a reference group for functional health status, caregivers of healthy classmates of children participating in the study were asked to complete both the FSII and RAND questionnaire.
Disease specific quality of life
Disease specific QOL was measured, both for patients and their caregivers, at baseline and 6 and 12 months after the start of the study. The Dutch version of the Paediatric Asthma Quality of Life questionnaire (PAQLQ) was used, including 23 items on activity limitation, symptoms, and emotional function.29 The Paediatric Asthma Caregiver’s Quality of Life questionnaire (PACQLQ) consists of 13 items on the emotional responses of caregivers and interference with family activities.30 Answers are expressed on a 7-point scale, a higher score reflecting a better quality of life.
Statistical analyses
Power calculation was based on the aim to be able to detect a difference of 15% between groups in the percentage of symptom-free days. Assuming standard deviations of 20% and a two tailed alpha of 0.05, a sample size of 70 patients was needed to achieve a power of at least 85%.
Variables were checked for normal distributions. Normally distributed variables are presented as mean (SD) and not normally distributed variables as median (range). PD20 results were logarithmically transformed (log10 PD20) to normalise the data and presented as the geometric mean (range). The mean daily dose of fluticasone during the study was calculated for each patient. From the diary, median symptom scores, mean percentage of symptom-free days, and percentage of rescue medication-free days were calculated for each patient and extrapolated over each follow up period. Differences within and between groups were analysed using parametric and non-parametric tests depending on the distribution of continuous data, and χ2 tests for proportions. The mean differences between groups in level of PD20, functional health status, and disease specific QOL at the end of the study were adjusted for baseline values (analysis of covariance). SPSS for Windows was used to analyse the data.
RESULTS
Clinical outcome
Between December 1999 and December 2000, 74 patients (out of 75 referred) were randomly assigned to follow up by either a paediatrician or asthma nurse. The mother of one patient declined to participate because she was pregnant. Seventy three (99%) of the patients completed the study. One patient followed up by an asthma nurse was diagnosed with tracheomalacia during the study period and excluded from the study. The baseline demographic and clinical characteristics of patients in both groups were comparable (table 1).
Baseline characteristics of patients treated by paediatrician or asthma nurse*
The mean percentage of symptom-free days throughout the study was comparable between the two treatment groups (table 2).
Results at end of study for patients treated by paediatrician or asthma nurse*
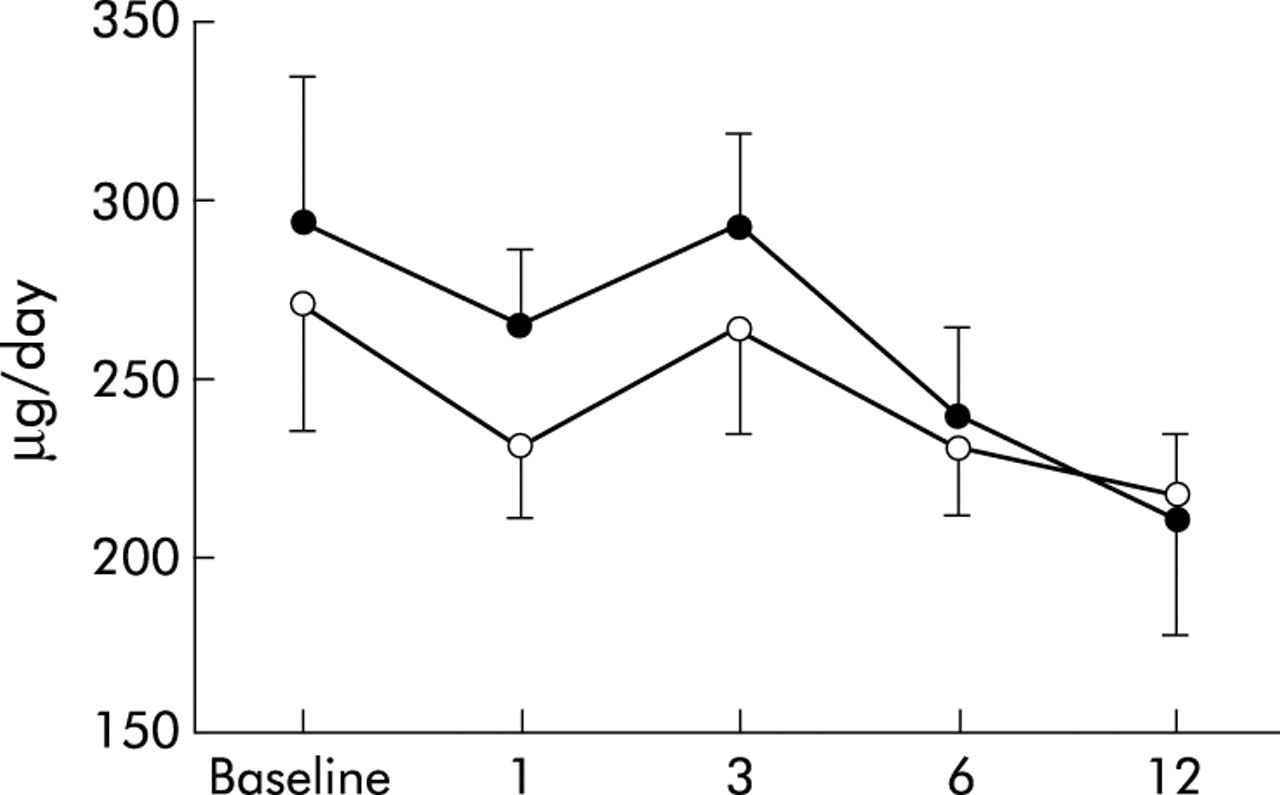
Fifty eight (78%) of the patients had already been prescribed ICS by their general practitioner before referral (table 1). For these 58 patients the mean dose of ICS at the end of the study was significantly lower than at baseline (215 (168) v 289 (207) µg/day; p=0.03, fig 1). The maximum dose of fluticasone prescribed during the study was ⩽500 µg/day for 99% of the patients. Only one patient, 16 years of age and followed up by an asthma nurse, was prescribed 1000 µg/day after the initial assessment by the paediatrician. At the next visit after 1 month, asthma control was achieved and the dose of fluticasone tapered off to 500 µg/day.

Mean (SE) dose of inhaled corticosteroids (ICS) during the study for patients followed up by paediatrician (○, n=28) and asthma nurse (•, n=30) in patients who had already been prescribed ICS by their general practitioner.
The percentage of patients who demonstrated a correct inhalation technique significantly increased from 65% to 95% at the end of the study (p<0.0001), without a significant difference between the two treatment groups.
PD20 improved significantly during the study and to a comparable level in both groups (p=0.001, table 2). There were no significant differences between groups in any of the other clinical end points (table 2). There were no emergency room visits or hospital admissions due to asthma.
Functional health status
Mean (SD) FSII score of all patients improved significantly from baseline (75.0 (17.4)) to the end of the study (87.8 (14.0); mean difference 12.8; 95% CI 4.5 to 18.5, p=0.002). The mean difference in FSII score between the two treatment groups at the end of the study was 10.1 (95% CI −0.3 to 19.8). For the RAND general health rating index the mean (SD) score also significantly improved from 21.3 (4.8) to 24.0 (4.1) (mean difference 2.7; 95% CI 1.1 to 4.5, p=0.003) The mean difference in RAND score between both groups at the end of the study was 0.1 (95% CI −2.8 to 2.7).
To put the FSII scores of our study population into perspective, we compared them with the scores of a healthy reference population (n=57). At baseline the mean FSII score of the asthmatic children was significantly lower than that of healthy children (75.0 v 91.0; p<0.001), but scores were comparable at the end of the study (87.8 v 91.0; p=0.06, fig 2).
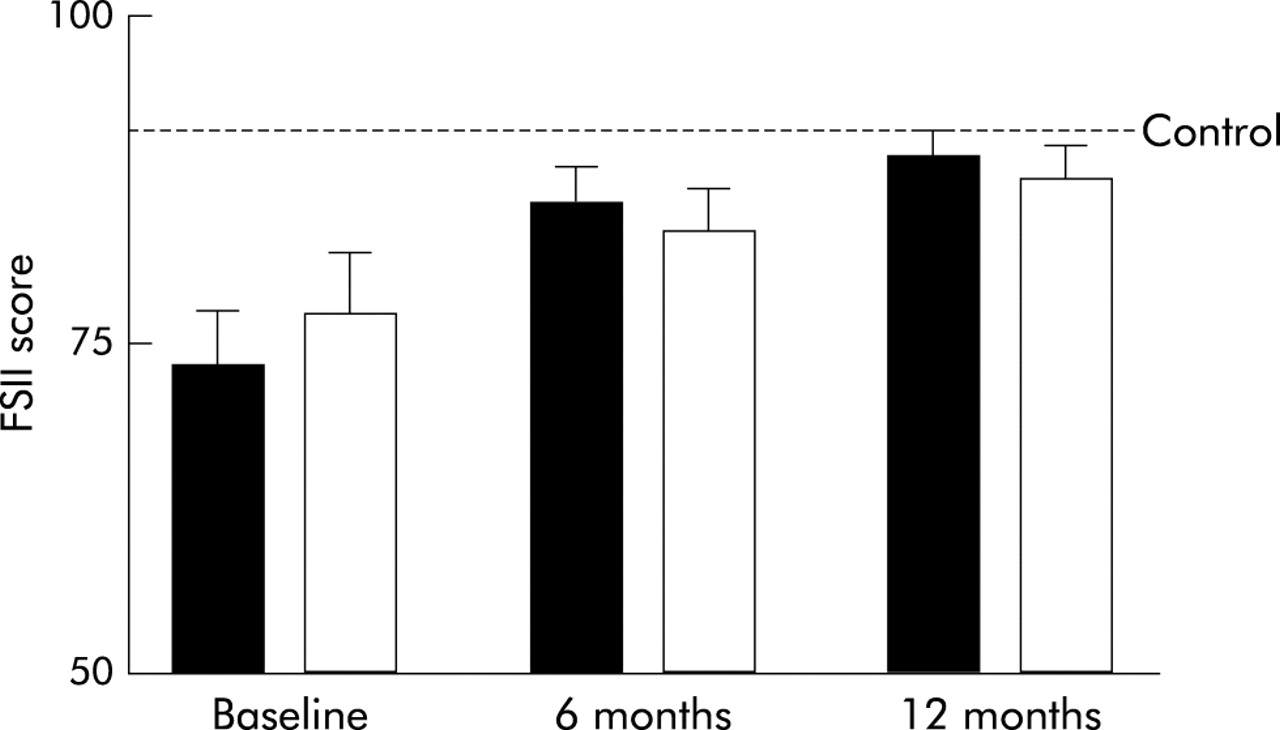
Mean (SE) FSII score for both treatment groups (closed bars=paediatrician, open bars=asthma nurse) at baseline and after 6 and 12 months of follow up. Dashed line represents the mean FSII score of the control group.
At the start of the study patients had significantly lower mean RAND scores than healthy children (21.3 v 27.9; p<0.001). RAND scores improved significantly in patients, but never reached the level of healthy children (24.0 v 27.9; p<0.001).
Disease specific quality of life
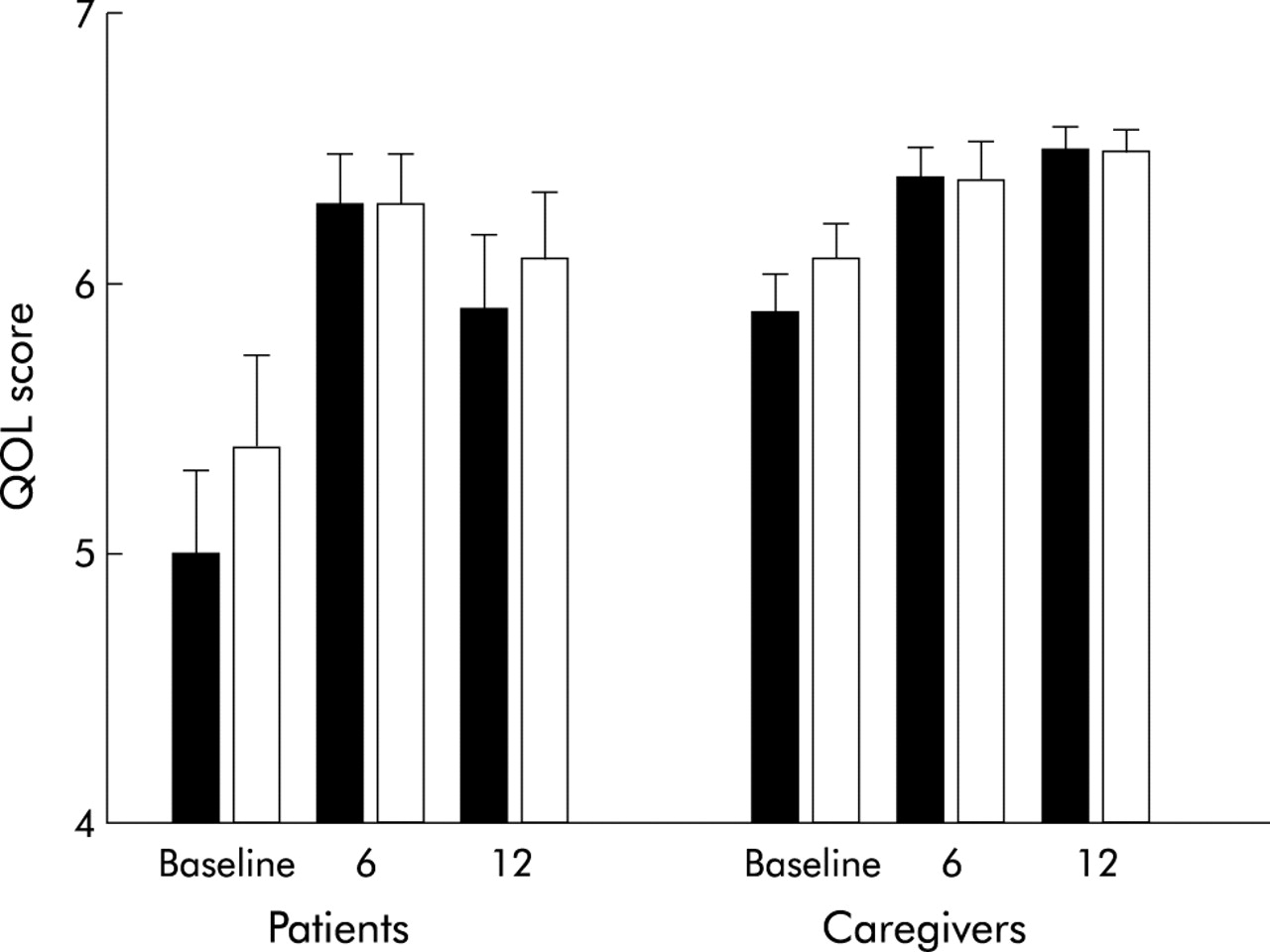
The mean overall disease specific QOL score significantly improved throughout the study for both patients (mean difference 0.8; 95% CI 0.4 to 1.3, p=0.001) and their caregivers (mean difference 0.5; 9% CI 0.4 to 0.7, p<0.0001). These improvements in QOL were not significantly different between groups (fig 3). At the end of the study the mean differences in disease specific QOL for patients and caregivers were 0.08 (95% CI −0.9 to 0.7) and 0.09 (95% CI −0.2 to 0.3), respectively. The improvements in the subdomains were also statistically significant and comparable between the two groups (data not shown).

{kind=link}
{kind=link}
{kind=link}
Mean (SE) overall disease specific quality of life score of patients and caregivers at baseline and after 6 and 12 months follow up (closed bars=paediatrician, open bars=asthma nurse).
Time investment of paediatrician and asthma nurse
The mean (SD) time spent on patient contact was 136 (14) and 187 (41) minutes for paediatricians and asthma nurses, respectively (p<0.001). During the study period the asthma nurses consulted the paediatrician 22 times for 16 patients representing 43% of all patients and 8.7% of all patients’ visits to an asthma nurse. This was most commonly for a physical examination in cases of inadequate asthma control.
Parental satisfaction with asthma care
All parents were satisfied with the asthma care received. In retrospect, 6% and 3% of the parents whose child was randomised to follow up by an asthma nurse or paediatrician, respectively, had the desire to have their child seen by a paediatrician more often (p=0.51). Of the parents whose child was treated by an asthma nurse or paediatrician, 94% and 82%, respectively, would not object to asthma nurse led management of their child’s asthma in the future (p=0.28).
DISCUSSION
This study shows no differences between outpatient management of children with asthma by a hospital based asthma nurse and traditional management by a paediatrician. No significant differences were found between groups in any of the outcome measures. The study was powered as a comparative trial, not as an equivalence study. The power was sufficient to show that the difference in percentage of symptom-free days between the two treatment groups was unlikely to be larger than 15%. All primary and secondary end points were comparable between groups at the end of the study (table 2); there was no trend in the data to suggest that an increase in power (for example, as an equivalence study) would have yielded different results.
During the study statistically and clinically relevant improvements in airway hyperresponsiveness, functional health status, and disease specific quality of life were seen. In accordance with earlier studies, children with asthma had poorer functional health status at the beginning of the study than their healthy peers,27–28,31 but by the end of the study they had reached a comparable functional health status. Our study did not have a placebo control group because this was considered to be ethically unjustified. Strictly speaking, therefore, it is possible that the improvements observed in airway hyperresponsiveness, functional health status, and disease specific quality of life are an expression of the natural history of asthma in this cohort, rather than the result of the medical and educational interventions applied. However, the improvements in airway hyperresponsiveness, functional health status, and disease specific quality of life observed in our study are comparable to those found in controlled studies on the effects of education3,10–11,32 and inhaled fluticasone.33,34
Most of the children in our study had already been treated with ICS but had been referred by their general practitioner because of insufficient control of symptoms. After the comprehensive education provided, the percentage of patients with correct inhalation technique increased considerably. This finding confirms our earlier observations that many asthmatic children, even when they have received inhalation instruction in primary care, have poor inhalation technique.35 We believe that this improved inhalation technique is an important contributing factor to the improved disease stability experienced by the patients during the study. Importantly, this improvement was achieved without increasing the dose of ICS, which strongly suggests that comprehensive patient education and close follow up is very important in the management of childhood asthma.
Many of the children we studied could well be managed in primary care once their asthma is controlled. However, our results emphasise that comprehensive patient education and regular follow up are prerequisites to maintain good asthma control. In our clinic, newly referred patients diagnosed with asthma are asked to visit the outpatient clinic 4–5 times during the first year.
Apart from the expertise of the asthma nurses, we believe that two factors in our study design were important in determining the success of asthma management by asthma nurses. Firstly, the asthma nurse could consult the paediatrician for medical advice, physical examination, or other queries at all times throughout the study. Although this was not a frequent event, the availability of low threshold paediatrician consultation helped to build confidence in the reliability of the nurse led follow up in patients, nurses, and physicians. Secondly, the treatment protocol gave clear guidelines when to increase, reduce, or maintain the dose of ICS, allowing the asthma nurses to adjust treatment independently within certain limits.
Until now, the contribution of the asthma nurse has been complementary to that of the physician.12–15 The results of our study clearly show that asthma nurses can take over large parts of long term management of mild to moderate childhood asthma from physicians without compromising quality of care or control of disease. This is in accordance with findings in adults with stable chronic disease in primary and secondary care.16–20
Because our study was conducted in a hospital based asthma clinic, our results cannot be extrapolated to a primary care setting. Further studies are needed to evaluate whether asthma management can be performed safely and effectively by asthma nurses alone in primary care. Similarly, the extent to which the results of this study can be extrapolated to other secondary care clinics deserves discussion. In this study, the efficacy of childhood asthma management by a paediatric pulmonologist was compared with care provided by an experienced asthma nurse. In many hospitals routine asthma follow up is provided by general paediatricians or junior doctors. Because it has been shown that specialist care results in better asthma control than management by general paediatricians,36 nurse led care may even be superior to doctor led care in such settings. This emphasises the need to train junior doctors adequately in the management of childhood asthma. Finally, because patients with mild intermittent and most severe asthma were not represented in our study population, further studies are needed to assess the efficacy of nurse led asthma care in the extremes of the asthma severity spectrum in children.
In conclusion, we have shown that the efficacy of nurse led outpatient management of childhood asthma was not different from traditional management by a paediatrician. Patients improved considerably despite using a lower dose of ICS, emphasising the importance of comprehensive education and regular follow up. Implementation of such nurse led asthma care will have a considerable impact on the use of healthcare resources.
Acknowledgments
This study was sponsored by Isala Klinieken (innovation of care project) and GlaxoSmithKline (unrestricted educational grant for A Kamps).
REFERENCES
Footnotes
-
Sponsored by GlaxoSmithKline.
-
A Kamps was supported by an unrestricted educational grant from GlaxoSmithKline. Both P Brand and RJ Roorda have been involved in clinical trials sponsored by GlaxoSmithKline. None of the other authors has any conflict of interest.
-
A Kamps was the overall study coordinator and was involved in the protocol design, data analysis and interpretation, and in writing the report. P Brand and RJ Roorda were involved in protocol design, data analysis and interpretation, and in writing and editing the report. RJ Roorda and P Brand were also responsible for clinical care and patient recruitment. A Overgoor and L van Helsdingen-Peek provided clinical care and were involved in editing the report. J Kimpen contributed to the protocol design and was involved in editing the report. A R Maillé was involved in analysis of quality of life data and interpretation, and in editing the manuscript.