Article Text

Abstract
Background: The pathophysiology of chronic obstructive pulmonary disease (COPD) features pulmonary inflammation with a predominant alveolar macrophage involvement. Bronchoalveolar macrophages from patients with COPD release increased amounts of inflammatory cytokines in vitro, an effect that is not inhibited by the glucocorticosteroid dexamethasone. Resveratrol (3,5,4′-trihydroxystilbene) is a component of red wine extract that has anti-inflammatory and antioxidant properties. A study was undertaken to determine whether or not resveratrol would inhibit cytokine release in vitro by alveolar macrophages from patients with COPD.
Methods: Alveolar macrophages were isolated from bronchoalveolar lavage (BAL) fluid from cigarette smokers and from patients with COPD (n=15 per group). The macrophages were stimulated with either interleukin (IL)-1β or cigarette smoke media (CSM) to release IL-8 and granulocyte macrophage-colony stimulating factor (GM-CSF). The effect of resveratrol was examined on both basal and stimulated cytokine release.
Results: Resveratrol inhibited basal release of IL-8 in smokers and patients with COPD by 94% and 88% respectively, and inhibited GM-CSF release by 79% and 76% respectively. Resveratrol also inhibited stimulated cytokine release. Resveratrol reduced IL-1β stimulated IL-8 and GM-CSF release in both smokers and COPD patients to below basal levels. In addition, resveratrol inhibited CSM stimulated IL-8 release by 61% and 51% respectively in smokers and COPD patients, and inhibited GM-CSF release by 49% for both subject groups.
Conclusions: Resveratrol inhibits inflammatory cytokine release from alveolar macrophages in COPD. Resveratrol or similar compounds may be effective pharmacotherapy for macrophage pathophysiology in COPD.
- chronic obstructive pulmonary disease
- interleukin 8
- red wine extract
- resveratrol
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory disease of the lung that is characterised by progressive and irreversible airflow limitation.1 The major risk factor for development of COPD is cigarette smoking, and the only intervention that slows disease progression is smoking cessation.2,3 The inflammatory cell profile in COPD includes macrophages, neutrophils, and T lymphocytes.4
Macrophages are implicated as coordinators of the pulmonary inflammation and parenchymal damage of COPD.1 For example, numbers of alveolar macrophages are increased in the lungs of patients with COPD,5,6 and macrophages from these patients release increased levels of cytokines7 and proteases8,9 compared with macrophages from control subjects. The macrophages contribute to airway inflammation in smokers and COPD patients by secreting neutrophil and macrophage chemotactic factors such as interleukin 8 (IL-8),10,11 cell survival factors such as granulocyte macrophage-colony stimulating factor (GM-CSF),7 and by the generation of reactive oxygen species.12
Current treatment for COPD is, for the most part, palliative and does not appear to inhibit disease progression.3,13 Although corticosteroids are an effective treatment for asthma,14 their efficacy in stable COPD is controversial.15,16 Consequently, alternative therapeutic approaches are being sought.17 Resveratrol (3,5,4′-trihydroxystilbene) is a polyphenolic molecule found in the skins of red fruits such as grapes, and is one of the compounds in red wine extract that exhibits a range of biological activities.18 It has antioxidant, antineoplastic, and anti-inflammatory properties.19–21 For these reasons, resveratrol is thought to contribute to the health benefits ascribed to the consumption of red wine.22
The aim of the present study was to examine the effect of resveratrol on cytokine release by alveolar macrophages from patients with COPD. We therefore determined whether or not resveratrol would inhibit basal and IL-1β or cigarette smoke medium (CSM) stimulated release of IL-8 and GM-CSF by macrophages from cigarette smokers and patients with COPD. We used IL-1β as an inflammatory stimulant because it is increased in bronchoalveolar lavage (BAL) fluid of cigarette smokers.23 CSM was used because of the association between cigarette smoking and development of COPD,2 and because CSM induces release of cytokines7 and proteases8 by BAL fluid alveolar macrophages.
METHODS
Patients
The 15 patients with COPD and 15 cigarette smoking control subjects reported here are the same as those described elsewhere.7 The COPD patients fulfilled the criteria of the British Thoracic Society24 with forced expiratory volume in 1 second (FEV1) % predicted less than 70% and a ratio of FEV1 to forced vital capacity (FVC) of less than 0.7 (table 1). The smokers were without airway obstruction (FEV1 >80% predicted, table 1). All subjects were current smokers and had a smoking history of >20 pack years. The subjects with COPD maintained their medication (β2 agonists, n=14; anticholinergics, n=15; inhaled corticosteroids, n=6). Smokers were unmedicated. The study was approved by the Riverside ethics committee and the ethics committee of the Royal Brompton and Harefield NHS Trust. Subjects gave informed written consent.
Clinical characteristics of healthy smokers and patients with COPD
Bronchoalveolar lavage
All subjects were asked to refrain from smoking from the night before BAL fluid sampling (approximately 12 hours). BAL fluid was collected as described previously7 by sequential instillation and aspiration of 60 ml warmed 0.9% (w/v) normal saline, up to a maximum of 240 ml. Subjects were monitored with digital oximetry.
Isolation and culture of alveolar macrophages
Alveolar macrophages were isolated from the BAL fluid as described previously.7 The macrophages were resuspended in RPMI-1640 medium containing 10% (v/v) fetal calf serum, 2 mM l-glutamine, 100 iu/ml penicillin, 100 μg/ml streptomycin, and 0.25 μg/ml amphotericin. Cells were seeded in 24-well Falcon cell culture plates (Becton Dickinson, Cowley, Oxfordshire, UK) at a density of 250 000 cells/well and incubated (37°C, 5% CO2, humidified air) for 2 hours to allow macrophage adherence. The medium was replaced and non-adherent cells removed by aspiration. The macrophages were cultured for 24 hours, after which the medium was replaced and cells cultured for a further 24 hours under experimental conditions. Resveratrol and the stimulants were co-administered at time zero. Ten μg/ml IL-1β was used because we have found previously that this concentration gives a consistent stimulation of both IL-8 and GM-CSF release.7 Cell viability was determined following experimental treatments using trypan blue dye exclusion.
Production of CSM and measurement of endotoxin
CSM was produced as described previously.7 Smoke from two cigarettes (12 mg tar, 0.9 mg nicotine) was bubbled through 20 ml culture medium and, to ensure standardisation between experiments and batches of CSM, the absorbance was adjusted by dilution to 0.15 at 320 nm using the method of Wirtz and Schmidt.25 This concentration (nominally 1) is not cytotoxic (see Results below) and was serially diluted with untreated media (0.001- to 1-fold) and applied to the macrophages. The concentration of endotoxin in a 1-fold dilution of CSM was measured using a QCL-1000 endotoxin kit (BioWhittaker, Walkersville, MD, USA) according to the manufacturer’s instructions. The limit of detection of the assay was 0.1 endotoxin unit (EU)/ml.
Cytokine measurements
IL-8 and GM-CSF were measured in macrophage culture supernatants using paired antibody quantitative ELISAs (R&D Systems, Abingdon, Oxfordshire, UK).7 The lower limit of detection was 15.6 pg/ml for both assays, with a coefficient of variation of 24% for the IL-8 assay and of 17% for the GM-CSF assay. In order to determine whether or not resveratrol affected the cytokine ELISAs, standard curves were constructed in the absence and presence of resveratrol (100 μM).
Statistical analysis
Concentrations of macrophage cytokines between treatment and controls and between COPD patients and smokers were compared using repeated measures analysis of variance (ANOVA). Where differences were found, the minimum value following treatment was taken as a summary measurement. The concentration of resveratrol causing 50% inhibition of stimulated cytokine release (IC50 value) was calculated using GraphPad Prism software (GraphPad Software Inc, San Diego, CA, USA). Data are presented as means with 95% confidence intervals (CI) unless stated otherwise.
RESULTS
We have previously reported that there was no difference in the number of inflammatory cells recovered or macrophage number in BAL fluid between the two groups.7 None of the experimental interventions affected the viability of the macrophages. Resveratrol did not affect the ELISA cytokine measurements; slopes of standard curves for IL-8 were 0.00085 (SE 0.00011) in the absence of resveratrol and 0.00083 (SE 0.00010) in the presence of resveratrol, and for GM-CSF the values were 0.0011 (SE 0.0001) and 0.0012 (SE 0.0001), respectively.
Effect of resveratrol on basal cytokine release
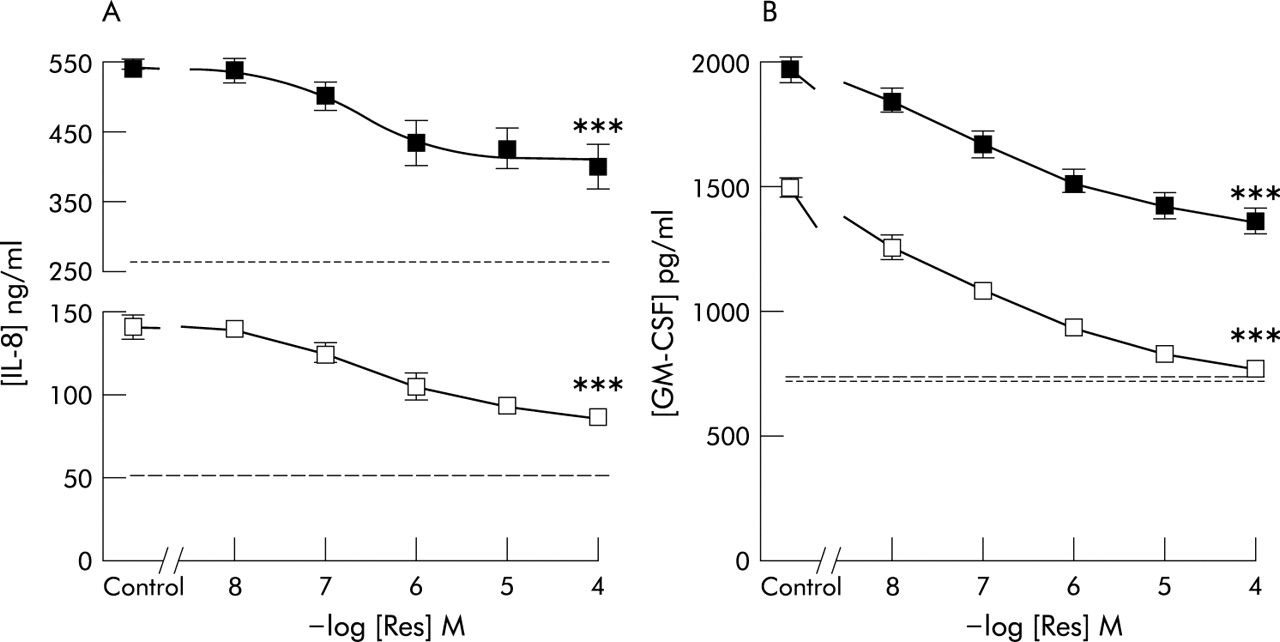
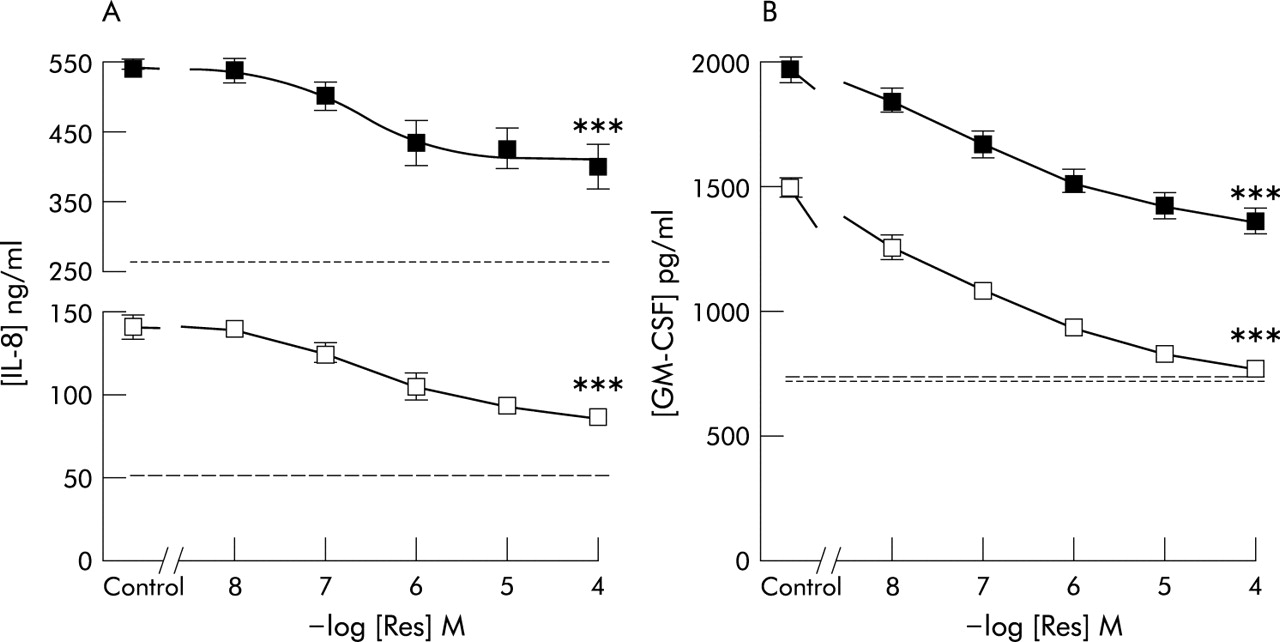
Basal IL-8 release from macrophages was approximately five times greater in patients with COPD than in smokers (262 pg/ml (95% CI 235 to 290) v 50 pg/ml (95% CI 45 to 57), fig 1A). Resveratrol inhibited basal IL-8 release by macrophages from both smokers (by 94% at 100 μM) and patients with COPD (by 88%, fig 1A). In contrast to IL-8 release, basal release of GM-CSF was similar in the two groups (724 pg/ml (95% CI 686 to 763) v 737 pg/ml (95% CI 697 to 777), fig 1B). Resveratrol inhibited GM-CSF release by macrophages from smokers and patients with COPD by 79% and 76%, respectively, at 100 μM (fig 1B). There was no significant difference between the IC50 values for inhibition by resveratrol of basal IL-8 or GM-CSF release by macrophages from smokers or patients with COPD (table 2).
Inhibition by resveratrol of basal or stimulated cytokine release from alveolar macrophages

Effect of resveratrol on basal cytokine release by alveolar macrophages from cigarette smokers (□) and patients with COPD (▪). Data are presented as mean (SE) concentrations of (A) IL-8 and (B) GM-CSF for 15 subjects in each group. For some data points SE values are within the symbol. ***p<0.001 versus control.
Effect of resveratrol on cytokine release induced by IL-1β
Exposure of macrophages from smokers or COPD patients to IL-1β (10 ng/ml) increased IL-8 release by 1.8-fold (50 pg/ml (95% CI 45 to 57) v 87 pg/ml (95% CI 83 to 91)) and 1.3-fold (262 pg/ml (95% CI 235 to 290) v 328 pg/ml (95% CI 306 to 351)), respectively, above basal values (fig 2A). Similarly, IL-1β increased GM-CSF release by approximately 1.8-fold above basal values in both groups (737 pg/ml (95% CI 697 to 777) v 1327 pg/ml (95% CI 1223 to 1431) and 724 pg/ml (95% CI 686 to 763) v 1348 pg/ml (95% CI 1148 to 1547), respectively; fig 2B). Resveratrol inhibited IL-1β stimulated IL-8 release and GM-CSF release by macrophages from both smokers and patients with COPD to below their respective basal levels (fig 2A and B). There was no significant difference in IC50 values for inhibition by resveratrol of IL-1β stimulated IL-8 or GM-CSF release by macrophages from smokers and patients with COPD (table 2).

Effect of resveratrol on IL-1β stimulated cytokine release by alveolar macrophages from smokers (□) and patients with COPD (▪). Data are mean (SE) concentrations of (A) IL-8 or (B) GM-CSF for 15 subjects in each group. For some data points SE values are within the symbol. ***p<0.001 versus control (IL-1β stimulated, 10 ng/ml); ordinate is split in panel A. The dashed line is the basal value for smokers and the dotted line is the basal value for patients with COPD.
Effect of resveratrol on cytokine release induced by CSM
Exposure of macrophages from smokers or patients with COPD to CSM (1 fold dilution) increased IL-8 release by ∼3-fold (50 pg/ml (95% CI 45 to 57) v 141 pg/ml (95% CI 128 to 154)) and ∼2-fold (262 pg/ml (95% CI 235 to 290) v 542 pg/ml (95% CI 518 to 265)), respectively, above basal values (fig 3A). Similarly, CSM increased GM-CSF release by ∼2-fold (737 pg/ml (95% CI 697 to 777) v 1493 pg/ml (95% CI 1398 to 1587)) and 2.7-fold (724 pg/ml (95% CI 686 to 763) v 1977 pg/ml (95% CI 1873 to 2081)) above basal values in smokers and COPD patients, respectively (fig 3B). The concentration of endotoxin in the CSM was below the level of detection of the assay (<0.1 EU/ml).
{kind=link}
{kind=link}
{kind=link}
Effect of resveratrol on cigarette smoke medium (CSM) stimulated cytokine release by alveolar macrophages from smokers (□) and patients with COPD (▪). Data are mean (SE) concentrations of (A) IL-8 and (B) GM-CSF for 15 subjects in each group. For some data points SE values are within the symbol. ***p<0.001 versus control (CSM stimulated, 1×dilution); ordinate is split in panel A. The dashed line is the basal value for smokers and the dotted line is the basal value for patients with COPD.
Resveratrol inhibited CSM stimulated IL-8 release by macrophages from smokers and patients with COPD by 61% and 51%, respectively (fig 3A). Similarly, resveratrol inhibited GM-CSF release by macrophages from smokers to basal levels and by macrophages from COPD patients by 49% (fig 3B). There was no significant difference between the IC50 values for inhibition by resveratrol of CSM stimulated IL-8 and GM-CSF release by macrophages from smokers and patients with COPD (table 2).
DISCUSSION
IL-1β or CSM stimulated cytokine release by BAL fluid alveolar macrophages from cigarette smokers and COPD patients, effects which have been described previously by us7 and by others.26 The increased basal levels of IL-8 release by macrophages from patients with COPD seen here are unlikely to be due to inhaled bronchodilator medication because β2 adrenoceptor agonists inhibit rather than stimulate cytokine release from differentiated U937 human macrophage-like cells,27 while acetylcholine stimulates cytokine release from bovine alveolar macrophages,28 an effect that would be counteracted by ipratropium bromide, leading to decreased cytokine levels. CSM stimulation of cytokine release is unlikely to be due to the presence of endotoxin in the CSM because endotoxin was not detected in the media. With reference to the validity of comparison of the effects of CSM in vitro to in vivo cigarette smoke exposure, the relationship between CSM and exposure of macrophages to cigarette smoke in vivo is not known. However, in rats CSM and cigarette smoke in vivo induce similar patterns of DNA damage.29 Although not measured specifically in the present study, differences in BAL fluid cytokine and inflammatory mediator concentrations between patients with COPD and smoking controls may influence subsequent macrophage responses.
We found that resveratrol inhibited both basal and stimulated cytokine release by BAL fluid macrophages from cigarette smokers and patients with COPD. This is consistent with the inhibitory effects of resveratrol in a variety of cell preparations, including macrophages. For example, resveratrol inhibited IL-12 and TNFα release30 and IL-6 release31 by murine peritoneal macrophages. It is noteworthy that, in the present study, the inhibition of cytokine release by resveratrol was similar for both IL-8 and GM-CSF and for both subject groups, as evidenced by the IC50 values (table 2). The mechanism of the inhibition by resveratrol of cytokine release is not explored in the present study. However, inhibition of cytokine release may be due to suppression of NF-κB and AP-1 activation,32 with a consequent reduction in inflammatory cytokine expression. Suppression of NF-κB may involve a decrease in the phosphorylation and, hence, degradation of I-κBα.33,34 For the inhibition of CSM induced cytokine release, resveratrol is an antioxidant18 and an antagonist for the receptor for aryl hydrocarbons which are found in cigarette smoke.35 These properties would both be consistent with inhibition of CSM induced responses.
We have previously found that the glucocorticosteroid dexamethasone did not inhibit IL-8 release by BAL fluid macrophages from patients with COPD.7 This is in contrast to the marked inhibition observed in the present study by resveratrol in these same patient groups. In particular, resveratrol inhibited CSM stimulated GM-CSF release from both patient groups, whereas dexamethasone had no inhibitory effect except at a high concentration (10 μM) in smokers. The reasons underlying these apparent differential inhibitory effects of resveratrol and dexamethasone are unclear, but may be due to the antioxidant properties of resveratrol in addition to its anti-inflammatory activity.
Current treatment for the lung inflammation in stable COPD is suboptimal, with clinical use of glucocorticosteroids being controversial.15,16 Any lack of corticosteroid efficacy could be the result of reduced steroid sensitivity by pulmonary macrophages.7 In the present study we found that resveratrol inhibits basal and stimulated cytokine release by BAL macrophages in COPD patients. Specifically, resveratrol inhibited release of the neutrophil chemotactic factor IL-8 and the cell survival cytokine GM-CSF. This could lead to inhibition of neutrophilia and decreased levels of inflammatory cytokines in the airways of patients with COPD. Thus, resveratrol or related compounds may be more effective pharmacotherapeutic compounds than corticosteroids for the treatment of chronic stable COPD. A possible clinical disadvantage of resveratrol is its low bioavailability. Consequently, resveratrol analogues such as piceatannol are under investigation.36
Acknowledgments
This study was supported by a Training Fellowship from the Medical Research Council, UK (SVC), Bayer plc, Stoke Poges, UK (CDM), and the British Lung Foundation (REKR).
REFERENCES
Linked Articles
- Airwaves