Article Text

Abstract
Background: Chronic obstructive pulmonary disease (COPD) is a syndrome of chronic progressive airflow limitation which occurs as a result of chronic inflammation of the airways and lung parenchyma. However, the role of inhaled corticosteroids in the treatment of COPD is controversial. We hypothesised that inhaled corticosteroids reduce the progression of airflow limitation in COPD.
Methods: A comprehensive literature search was conducted and data were analysed using random effects methodology. The effect of inhaled steroids on annual change in forced expiratory volume in 1 second (FEV1) was determined for all trials, for trials with high dose treatment regimens, and for trials in subjects with moderate to severe airflow limitation.
Results: Data from eight controlled clinical trials of ⩾2 years were included (n=3715 subjects). Meta-analysis of all study data revealed that inhaled corticosteroids reduce the rate of FEV1 decline by 7.7 ml/year (95% confidence interval (CI) 1.3 to 14.2, p=0.02). Meta-analysis of studies with high dose regimens revealed a greater effect of 9.9 ml/year (95% CI 2.3 to 17.5, p=0.01) compared with the meta-analysis of all studies.
Conclusions: Inhaled corticosteroid treatment for ⩾2 years slows the rate of lung function decline in COPD. The effect observed with high dose regimens is greater than that with all regimens combined. These data suggest a potential role for inhaled corticosteroids in modifying the long term natural history of COPD.
- inhaled corticosteroids
- chronic obstructive pulmonary disease
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a syndrome of chronic and progressive airflow limitation which occurs as a result of chronic inflammation of the airways and lung parenchyma.1 Chronic inflammation leads to a progressive deterioration of airflow which is manifested by an accelerated annual rate of decline in the forced expiratory volume in 1 second (FEV1) of approximately 60 ml/year.2 In comparison, non-smokers experience a rate of decline in FEV1 of approximately 30 ml/year.2 This physiological deterioration provides the substrate for the clinical manifestations of COPD, which include cough, sputum production and dyspnoea. Therapeutic options to modify disease progression in COPD are limited and, although pharmacological interventions such as inhaled bronchodilators effectively treat symptoms, they have not been shown to modify the long term progression of airflow limitation.
Inhaled corticosteroids reduce airway inflammation, airflow limitation, and symptoms in asthma and are the mainstay of treatment for patients with persistent asthma.3 In COPD, however, the role of inhaled corticosteroids is controversial, as the inflammatory phenotype differs from that seen in asthma1 and has been reported to respond less favourably in the short term to inhaled corticosteroids.4 There is also ongoing debate surrounding the importance of the physiological versus the clinical response to inhaled corticosteroids. Individual controlled clinical trials comparing inhaled corticosteroids with placebo for treatment periods of 12 months or more have failed to show a significant effect on the rate of decline in FEV1. However, these same trials have shown that medium to high dose3 inhaled corticosteroids have beneficial effects on clinical outcomes such as symptoms,5 exacerbation rate, and health status.6,7 The fact that these drugs have a significant clinical effect even though their physiological effects are negligible may explain why inhaled corticosteroids are prescribed frequently for the treatment of COPD.8
We hypothesised that inhaled corticosteroids reduce the progression of airflow limitation in COPD, but that the ability of previous trials to detect a numerically small long term effect on FEV1 has been limited by design considerations including sample size and duration of follow up. To minimise the effect of the early increase in FEV1 seen in many trials of inhaled steroids in COPD, this meta-analysis focused on trials with a duration of ⩾2 years. The primary outcome measure for this meta-analysis was progression of airflow limitation as reflected by annual decline in FEV1.
METHODS
Data sources and study selection
A comprehensive search of the published literature was conducted using the medical subject headings chronic obstructive pulmonary disease, chronic bronchitis, pulmonary emphysema, steroids, beclomethasone, budesonide, and triamcinolone and the supplementary terms flunisolide and fluticasone. The search was restricted to clinical trials and MEDLINE (1966–February 2003 (week 2)), CINAHL (1982–February 2003 (week 2)), International Pharmaceutical Abstracts (1970–February 2003 (week 2)), and the Cochrane controlled trials register (fourth quarter, 2002) were queried. Reference lists from retrieved articles were reviewed to identify additional candidates for inclusion. Attempts were made to identify additional data or unpublished studies of inhaled corticosteroids in COPD through discussions with experts in the area of COPD pharmacotherapy at the 2002 American Thoracic Society international meeting.
Included studies met the following criteria: (1) design: randomised controlled clinical trial of an inhaled corticosteroid in subjects with COPD; (2) follow up: minimum of 1 year; (3) primary outcome variable: change in FEV1 over time; (4) disease-specific factors: subjects with asthma were excluded and subjects were studied when the disease was stable; and (5) publication type: not published solely in abstract form.
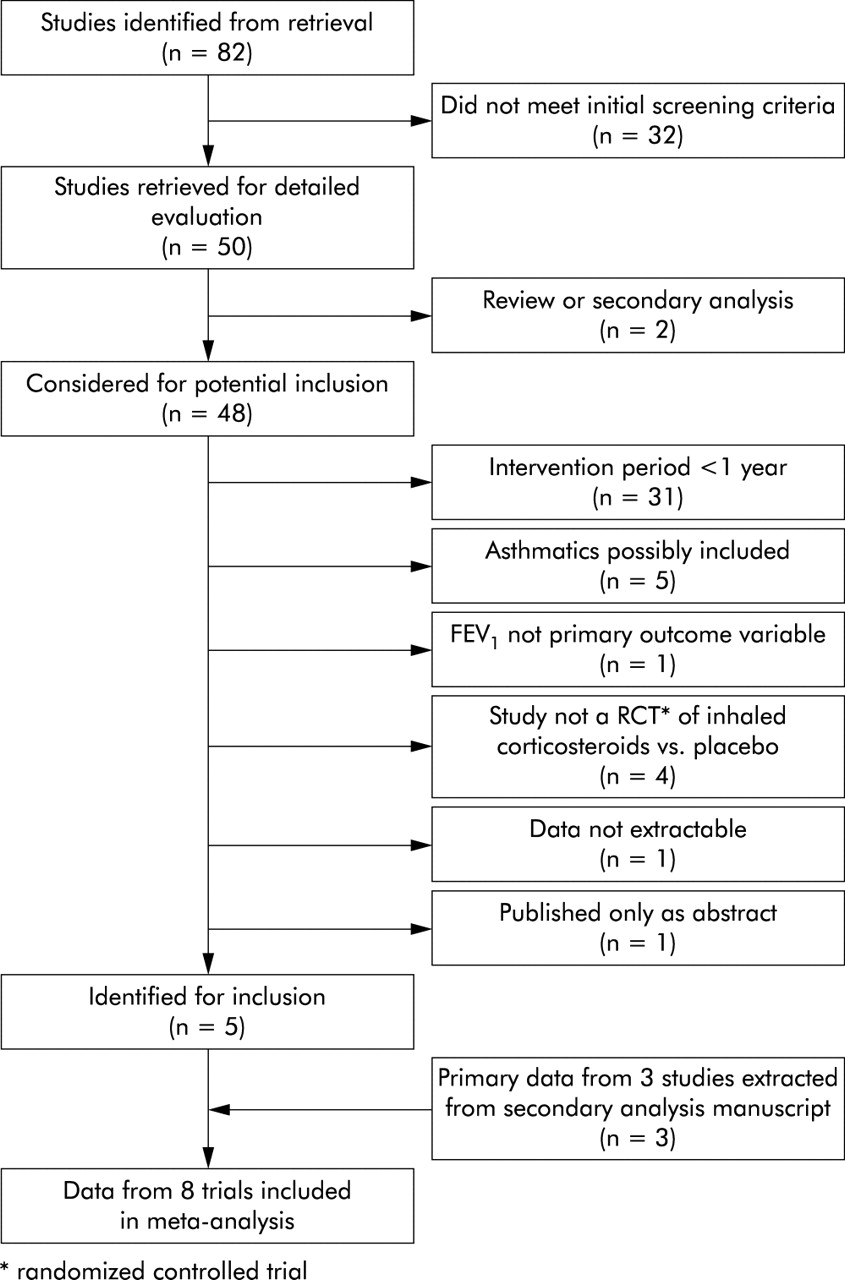
The results of the literature search were then sorted, using the criteria above, for inclusion in the meta-analysis (fig 1). Pertinence of these citations to the meta-analysis was evaluated using a sequential screening approach beginning with the title, followed by evaluation of the abstract and then the paper itself. Screening of citations was performed individually by each author and trials were selected and agreed upon by consensus.

Flow diagram depicting the selection of studies for meta-analysis.
Outcome variable
The primary outcome for this meta-analysis was annual rate of change in FEV1, a primary end point for which multiple individual trials of inhaled corticosteroid therapy have been unable to show a significant effect.
Data extraction and quality
Data regarding the primary outcome variable were abstracted from each article and confirmed by consensus. With one exception,9 investigators modelled the mean annual change in FEV1 to take into account the correlated nature of repeated measures within individuals. One of the eight trials10 reported a median change in FEV1 over time. After an unsuccessful attempt to obtain mean values for the primary outcome from this large study (n=1277), an assumption was made that the median value approximated the mean, and standard error was estimated from the reported p value11 for the median differences. The assumed mean and estimated standard error conformed closely to outcome data reported in other clinical trials. Standard error was calculated from the 95% confidence interval where necessary.12 Data reflecting change over the entire study period were abstracted for use in the meta-analysis.
Statistical analysis
The random effects model of DerSimonian and Laird13 was used to perform quantitative synthesis of the extracted data. Random effects methodology was chosen to account for both within study and between study variation.14 Summary effect estimates were represented as a point estimate and 95% confidence intervals and plotted on a forest plot.15 Heterogeneity of data was evaluated using the Q statistic.16 Publication bias was evaluated by means of a funnel plot17 and formal statistical analysis.18 STATA software version 7 (STATA Corporation, College Station, Texas) was used for all analyses.
RESULTS
Study selection
The literature search strategy identified 82 unique and potentially relevant citations (fig 1). Review of bibliographies and discussion with experts did not uncover additional studies. Thirty two citations did not meet initial screening criteria, leaving 50 citations for which abstracts were reviewed for inclusion. Of these abstracts, one was a qualitative review of inhaled corticosteroids in COPD and one was a secondary pooled analysis of primary data from three prior clinical trials. Of the remaining 48 abstracts, 43 were excluded for the following reasons: follow up was less than 1 year (n=31), subjects with asthma were possibly included (n=5), FEV1 was not the primary outcome variable (n=1), study was not a randomised controlled clinical trial of inhaled corticosteroids versus placebo (n=4), data were not extractable (n=1), or the study was published in abstract form only (n=1).
The five remaining studies5,7,9–10,12 were included in this meta-analysis. Close evaluation of the secondary analysis paper19 revealed it to be an analysis of data from three prior clinical trials of long term inhaled corticosteroids20–22 in which, in some cases, a mixed population of subjects with asthma and COPD were evaluated. The authors obtained the original study data for subjects with COPD and performed a pooled analysis of the data from these subjects.19 Because of their pertinence to this meta-analysis, these data were included, making data from subjects enrolled in a total of eight individual studies available for meta-analysis.
Subject and study characteristics
Data for 3715 subjects were available for meta-analysis. Table 1reports age, baseline FEV1 as percentage predicted, FEV1 percentage reversibility in response to inhaled beta-agonist, and smoking prevalence for the placebo and steroid arms of each study. Table 2reports the number of subjects by treatment allocation, drug used for treatment, and duration of treatment for each study. Although the search strategy was designed to identify studies with a duration of as little as 1 year, all studies were ⩾2 years in duration. The annual change in the rates of FEV1 decline from each study is reported in table 3.
Age, physiological characteristics, and smoking status of study subjects randomised to receive placebo or inhaled corticosteroid
Number of subjects and treatment allocation by study
Annual rate of decline in post-bronchodilator FEV1 by treatment allocation
Effect of inhaled corticosteroids on FEV1
Random effects meta-analysis of data from all studies indicated that inhaled corticosteroids significantly reduced the rate of decline in FEV1 by 7.7 ml/year (95% confidence interval (CI) 1.3 to 14.2, p=0.02; fig 2).
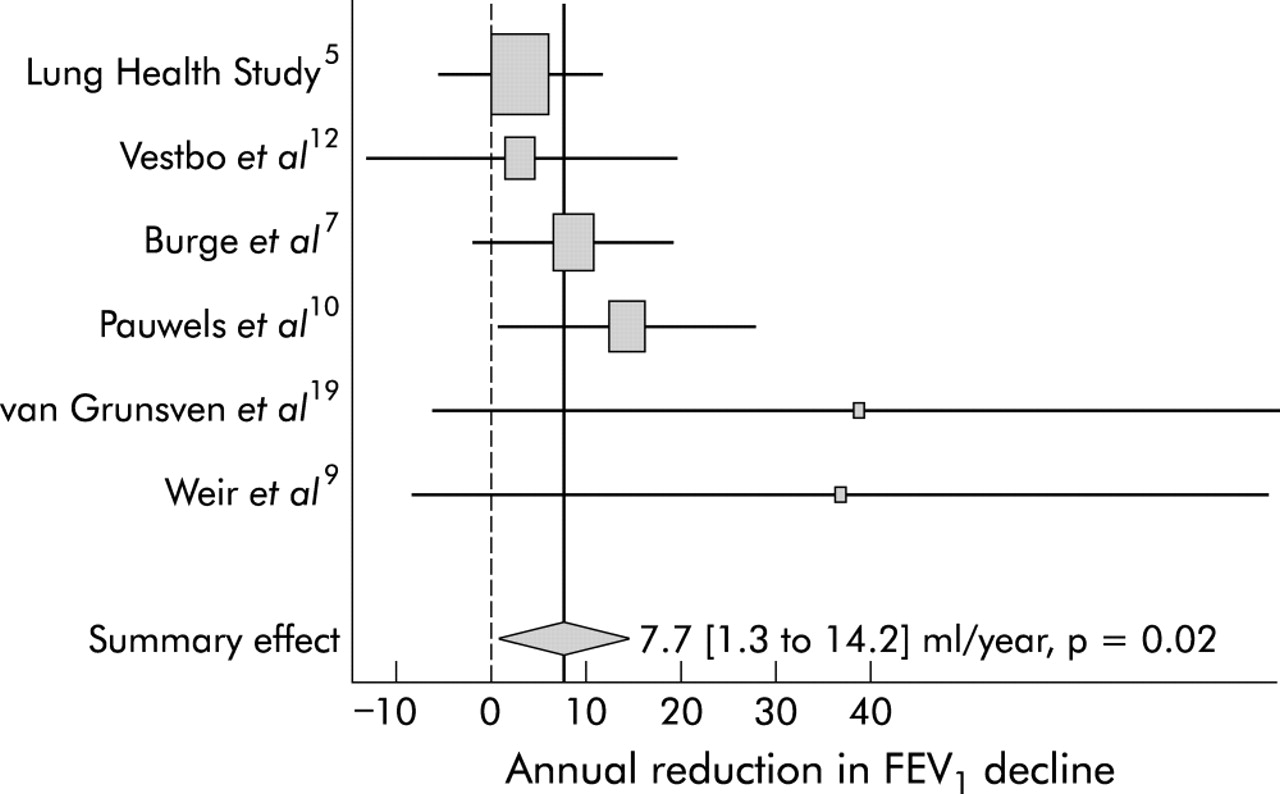
Summary effect of inhaled corticosteroids on the rate of decline in post-bronchodilator FEV1 in patients with COPD. The centre of the diamond indicates the summary effect and its width the 95% confidence interval.
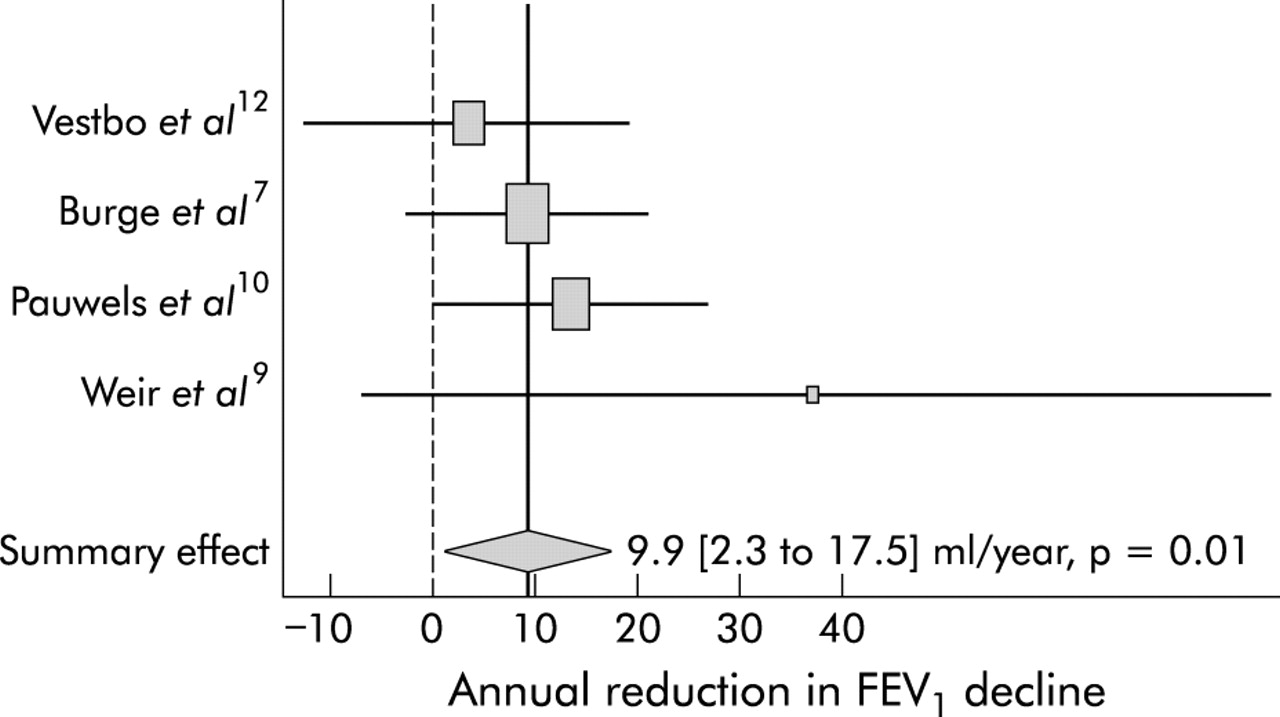
Sensitivity analyses were performed to determine whether there was an increased response to high dose3 inhaled corticosteroids and whether inhaled steroids had a greater effect in subjects with baseline FEV1 ⩽50% of predicted. Meta-analysis of trials with high dose steroid regimens (n=2416)7,9–10,12 demonstrated a greater reduction in the rate of FEV1 decline of 9.9 ml/year (95% CI 2.3 to 17.5, p=0.01) than was seen in the meta-analysis of all studies (fig 3). Comparison meta-analysis of studies with lower dose regimens could not be performed as only one of the included studies (the Lung Health Study5) used a non high-dose regimen. The secondary analysis of van Grunsven and colleagues19 pooled data from subjects who were treated with a mixture of medium and high dose regimens and these data were therefore not appropriate for inclusion in the analysis of lower dose studies.

Summary effect of high dose inhaled corticosteroids on the rate of decline in post-bronchodilator FEV1 in patients with COPD. The centre of the diamond indicates the summary effect and its width the 95% confidence interval.
In studies which enrolled subjects with a baseline FEV1 of ⩽50% predicted (n=1032 subjects),7,9,19 a reduction in the rate of decline in FEV1 of 18.3 ml/year was observed, but the 95% confidence interval was not significant (−1.5 to 38.0 ml/year, p=0.07).
Statistical heterogeneity and publication bias
For the analysis of all studies there was no evidence of significant statistical heterogeneity (Q =5.9, p=0.32). Furthermore, there was no evidence of significant statistical heterogeneity in the analysis of studies which used high dose inhaled corticosteroid regimens (Q =2.4, p=0.50) or in the analysis of studies which enrolled subjects with a baseline FEV1 of ⩽50% predicted (Q =2.8, p=0.25).
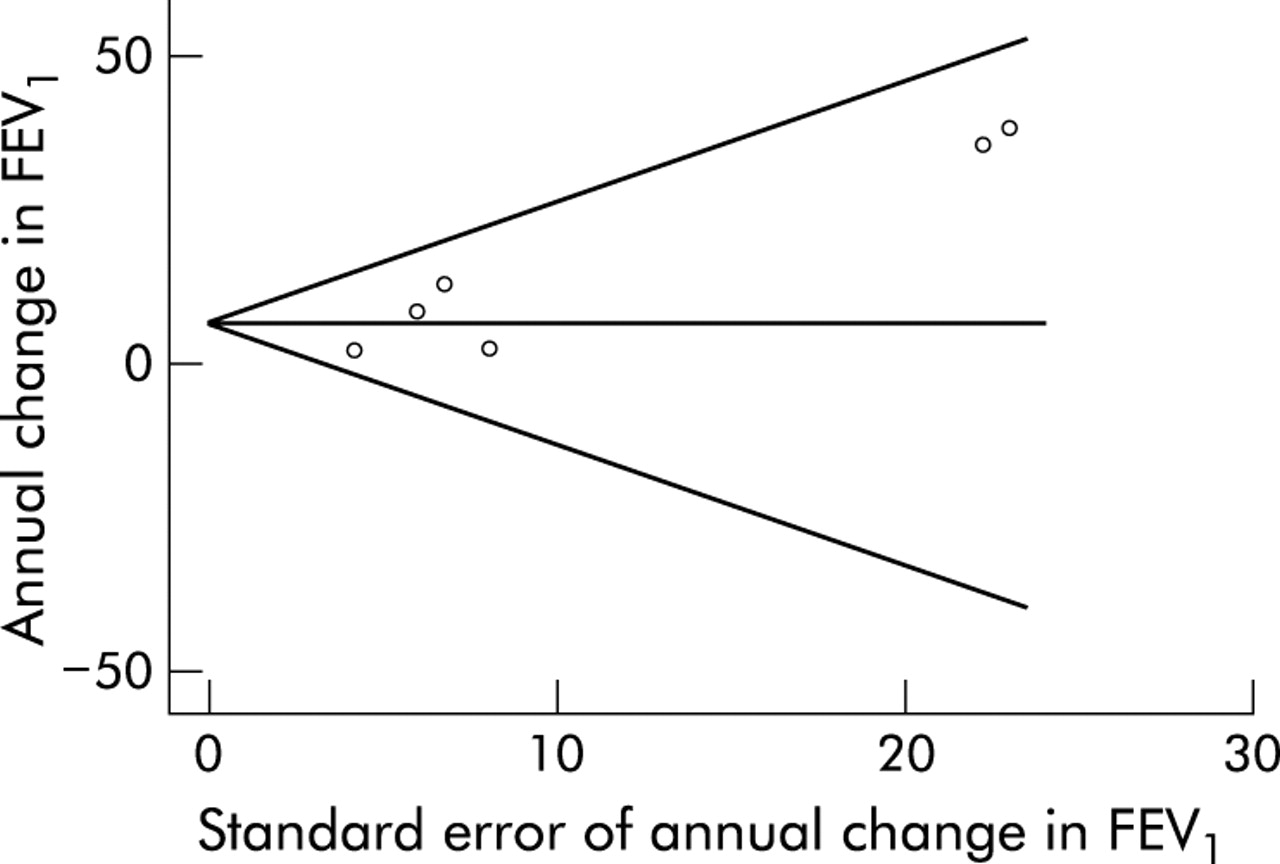
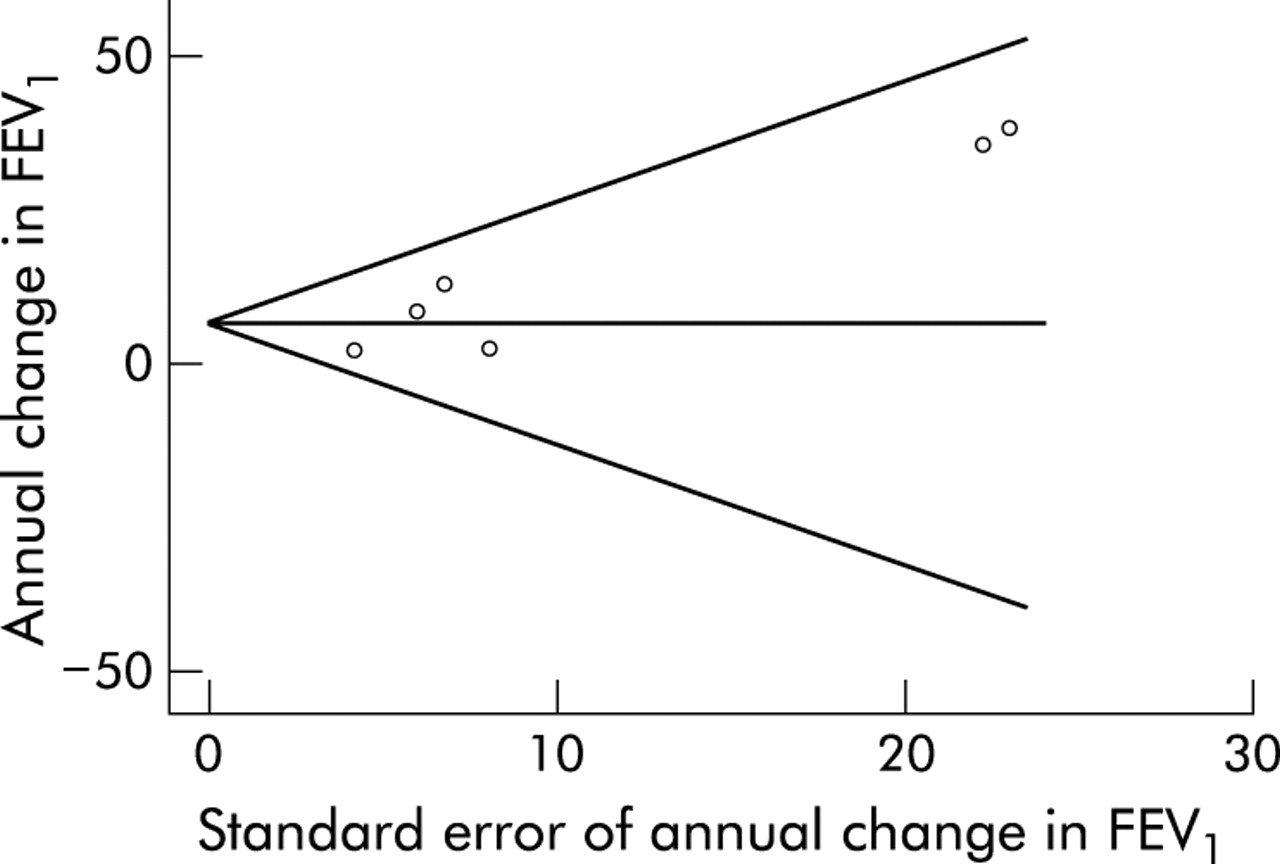
Funnel plot analysis (fig 4)17 of the included studies demonstrated asymmetry with an Egger18 p=0.03, suggesting that there was publication bias manifested by an absence in the literature of studies that resulted in negative mean effect estimates with high standard errors.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of included studies.
DISCUSSION
The results of this meta-analysis suggest that inhaled corticosteroids significantly slow the rate of deterioration in FEV1 in patients with COPD when used for a period of at least 24 months. This effect appears to be augmented by high dose regimens3 of inhaled corticosteroids.
The size of the effect derived from inhaled corticosteroids is numerically small, with the reduction in the rate of FEV1 decline ranging from 7.7 to 9.9 ml/year. Although these numbers are small in the absolute, they represent a relative reduction in the rate of FEV1 decline of approximately 13–17% in smokers with COPD and 26–33% in non-smokers with COPD.2 This effect of inhaled corticosteroids on the rate of FEV1 decline is less than the effect of smoking cessation, which can achieve a reduction of approximately 50% in the rate of deterioration.2 However, many of the subjects contributing data to this meta-analysis continued to smoke during inhaled corticosteroid treatment, suggesting that the beneficial effect of inhaled corticosteroids occurs despite an ongoing inflammatory stimulus.
Current guidelines recommend that inhaled corticosteroids be administered to COPD patients with frequent symptoms despite optimal bronchodilator therapy, frequent exacerbations, and FEV1 of ⩽50% predicted.23 Analysis of studies on this population showed a trend towards a greater effect that did not achieve statistical significance. Further research is required to determine which patients respond best to inhaled corticosteroids and whether this effect is greater in patients with low FEV1. Although we were able to show a larger effect size with studies of high dose regimens compared with all studies, only one lower dose study5 was available for comparison, preventing a comparison meta-analysis and possibly limiting the ability to draw conclusions about dose-response. The majority of long term studies of inhaled corticosteroids in COPD have used high dose regimens and, although the greater effect size seen in high dose studies may be evidence of a dose-response effect, it may also reflect issues related to sample size and statistical heterogeneity.
The clinical importance of an improvement in FEV1 of 7.7–9.9 ml/year is debatable. However, as noted previously, many of the trials included in this meta-analysis showed a benefit of inhaled corticosteroids with regard to secondary outcome measures such as exacerbation frequency, symptom scores, and quality of life. Exacerbations contribute to the decline in lung function in COPD,24 and the effect of inhaled steroids on FEV1 may be mediated in part by a reduction in exacerbation frequency. Additionally, the physiological benefit of inhaled corticosteroids may not be reflected by changes in FEV1 but rather by changes in lung volumes and hyperinflation, as occurs with inhaled bronchodilators.25 Although the numerical effect of inhaled steroids is small, these drugs do have a moderate relative effect and may supplement other interventions such as smoking cessation in modifying the natural history of this disease. The fact that studies with a follow up of ⩾2 years were included in this meta-analysis may underestimate the beneficial short term effects of inhaled steroids. In many clinical trials of these drugs in COPD there is an increase in FEV1 over the initial months of treatment, so we chose long term studies to avoid an undue influence of this early increase on the long term outcome. However, we did not have access to the primary data necessary formally to test the effect of this initial increase on the overall outcome, and further studies are needed to determine the effect of this initial increase on the overall response.
The choice of primary end points also affects interpretation of clinical trials of inhaled corticosteroids in COPD, and improving FEV1 has been an elusive goal in clinical trials in patients with this condition. FEV1 is poorly correlated with symptom indices,23 and improvement in FEV1 may be a suboptimal choice of primary outcome for clinical trials. Many of the trials included in this meta-analysis reported significant results for secondary end points including symptom scores, quality of life and exacerbation rates, an effect confirmed in a recent meta-analysis of exacerbation rates in short and long term trials of inhaled corticosteroids in COPD.26 It should be noted that, in seven of the eight included studies, a modelled rather than crude estimate of post-bronchodilator FEV1 change was reported. Although this may have improved our ability to detect a positive effect, modelling is a necessary and appropriate means of accounting for the correlated nature of longitudinal spirometric data.
This meta-analysis has limitations. Although we did not find any evidence of statistical heterogeneity, there is design heterogeneity between the included studies with regard to factors such as pre-randomisation physiology, smoking prevalence, drug dosing, and study duration. This is likely to have an impact on inhaled corticosteroid efficacy, but it may also more fairly represent the real life clinical variation seen in the treatment of patients with COPD. However, our inclusion of only randomised studies forced these factors to be distributed randomly in the study population, reducing the likelihood that they were significant confounders. There is a suggestion of publication bias in that there is an absence of small studies with negative outcomes in the reported literature. Whether this represents true publication bias or whether studies with such results have been performed is unclear. There is no shortage of large studies with negative outcomes, and it is unlikely that identifying small negative studies would significantly impact on these results. Finally, as is often the case in meta-analyses of published literature, data quality differed between studies. For example, only 72% of included data were specified by original investigators to have been analysed by intent-to-treat principles, and median (rather than mean) outcome data were used in one case.
In summary, these data suggest that inhaled corticosteroids significantly slow the rate of decline in FEV1 in patients with COPD. The effect is numerically small but represents a moderate relative effect compared with interventions such as smoking cessation. Further clinical data from studies of inhaled corticosteroids are necessary to inform clinicians more fully as to the appropriate place of these drugs in COPD pharmacotherapy.
Acknowledgments
The authors acknowledge the contribution of Michael A Stoto, PhD to this research.
REFERENCES
Footnotes
-
Funding: NIH K23 HL04385 (Dr Sutherland), The Wellcome Trust (Dr Venn).
Linked Articles
- Airwaves