Article Text

Abstract
Background: In chronic obstructive pulmonary disease (COPD), the degree of circadian variation in forced expiratory volume in 1 second (FEV1) and the influence of anticholinergic blockade is not known. Tiotropium is a long acting inhaled anticholinergic bronchodilator that increases daytime FEV1 in COPD. We hypothesised that tiotropium would modify the overnight change in FEV1, and this would be unaffected by the timing of drug administration.
Methods: A double blind, randomised, placebo controlled trial was conducted with tiotropium 18 mg once daily in the morning (09.00 hours), evening (21.00 hours), or an identical placebo. Patients with stable COPD (n=121, FEV1=41% predicted) underwent spirometric tests every 3 hours for 24 hours at baseline and after 6 weeks of treatment.
Results: There were no significant differences at baseline between the groups. Tiotropium improved mean (SE) FEV1 (over 24 hours) in the morning (1.11 (0.03) l) and evening (1.06 (0.03) l) groups compared with placebo (0.90 (0.03) l), and nocturnal FEV1 (mean of 03.00 and 06.00 hours) in the morning (1.03 (0.03) l) and evening (1.04 (0.03) l) groups compared with placebo (0.82 (0.03) l) at the 6 week visit (p<0.01). FEV1 before morning or evening dosing was similar, while the peak FEV1 moved later in the day with active treatment. The mean percentage change in FEV1 from 09.00 hours to 03.00 hours (the nocturnal decline in FEV1) was −2.8% in the morning group, −1.0% in the evening group, and −12.8% in the placebo group. The magnitude of the peak to trough change in FEV1 was not statistically different.
Conclusions: Tiotropium produced sustained bronchodilation throughout the 24 hour day without necessarily abolishing circadian variation in airway calibre.
- tiotropium
- chronic obstructive pulmonary disease
- circadian rhythm
Statistics from Altmetric.com
Many patients with respiratory disease complain of symptoms which are worse during the night or in the early morning. This has been well documented in bronchial asthma1,2 but is also reported by patients with chronic obstructive pulmonary disease (COPD).3–,5 In patients with asthma the symptoms have usually been ascribed to a substantial increase in the normal circadian variation in airway calibre,6 but data in COPD are less convincing and have relied on unsupervised home peak expiratory flow (PEF) recording. Nonetheless, a circadian variation of 16 l/min per day has been reported in COPD and is substantially less than in asthmatic subjects.7
There is general agreement that central cholinergic mechanisms are the major determinants of this variation in airway calibre.8 However, this has been difficult to test in man as the duration of action of existing anticholinergic drugs does not completely span the overnight period.9 Moreover, the side effects of systemically administered anticholinergic drugs preclude the chronic treatment required to assess this response, as does their attendant sleep disruption. Nonetheless, there are data that suggest that inhaled oxitropium bromide can reduce the overnight fall in PEF in nocturnal asthma.10
Tiotropium bromide is a new long acting inhaled anticholinergic bronchodilator that improves lung function for 24 hours after once daily dosing. The pharmacological properties of muscarinic receptor kinetic subselectivity11,12 and prolonged binding to the M3 receptor have been proposed as explanations for this prolonged duration of action.13 An earlier dose ranging study of single dose tiotropium in patients with COPD showed that, despite significant bronchodilation, a nocturnal decline in FEV1 occurred approximately 15–19 hours after morning inhalation of a single dose.14 This change was less marked than that with placebo, suggesting that morning administration of tiotropium partially reverses the nocturnal decline in lung function.
Evening administration of tiotropium has not previously been evaluated. The time of administration may influence the pharmacodynamics of some bronchodilators such as theophylline, with evening administration of certain formulations having a more pronounced effect on lung function during the night.15 Similar time dependent effects of dosing have been seen with corticosteroids in asthma.16,17
In this study we examined whether the circadian variation in FEV1 in patients with COPD was greater than that reported in healthy subjects, whether it could be abolished or reduced by sustained anticholinergic blockade in the airways, and whether the timing of the dose of tiotropium influenced its effect on overnight FEV1 compared with placebo treated patients.
METHODS
Subjects
All patients recruited were at least 40 years old with a smoking history of at least 10 pack years and a clinical diagnosis and spirometric parameters compatible with COPD as defined by the American Thoracic Society (ATS).18 Their FEV1/FVC ratio was less than 70% and their absolute FEV1 was 25–65% predicted using the European Community for Coal and Steel (ECCS) reference values.19 Patients with a history of asthma, allergic rhinitis, or atopy, or a total eosinophil count ⩾600/mm3 were excluded, as were those with significant diseases other than COPD. No patient had experienced an exacerbation of COPD within the preceding 4 weeks. Medications not permitted after the run in phase were short acting inhaled anticholinergic drugs, long acting inhaled β agonists, oral β agonists, and theophylline. Use of other concurrent medication was required to be stable during the study period. The protocol was approved by local institution review boards and informed consent was obtained from all patients.
Study design
A 6 week, multicentre, randomised, double blind, double dummy, parallel group design was used. Three treatment arms were compared: tiotropium 18 μg daily administered at 09.00 hours (Tio-AM), tiotropium 18 μg daily administered at 21.00 hours (Tio-PM), and placebo. All patients inhaled the contents of one capsule twice daily (either placebo or tiotropium, depending on the group). The times of study administration selected were based on the anticipated average time that a person might take morning or evening medication, considering the study design needed to separate the dose-time interval by 12 hours. Study medication was administered by a dry powder device (HandiHaler).
After initial screening, patients entered a 7 day baseline period to ensure clinical stability (no exacerbations). They attended the clinic where spirometric tests were performed 3 hourly over a 24 hour period, at the end of which they received their first morning dose of study medication. They were instructed to take the study medication in the morning (09.00 hours) and evening (21.00 hours) and to record their morning and evening PEF throughout the study in a diary card immediately before administering study medication.
After 6 weeks the patients attended for their second clinic visit. Spirometric assessment began before the administration of the evening dose of medication. Patients remained in the clinic overnight and spirometric tests were again repeated 3 hourly throughout the following day (including overnight measurements and immediately before the morning dose of study medication). Patients were awakened for spirometric testing if necessary.
A continuous 24 ECG (Holter monitor) was recorded during the patients’ stay in the clinic at baseline and at 6 weeks. Analysis of the Holter ECG tapes was performed by Hertford Medical BV, Maasdam, The Netherlands by investigators blinded to the purpose of the study. Adverse events were monitored throughout the baseline and 6 week treatment periods.
Study procedures
Baseline spirometric tests were conducted between 08.00 and 12.00 hours. They were conducted in triplicate and met ATS standards of reproducibility.20 The highest values of FEV1 and FVC from three reproducible tracings were recorded. Identical portable electronic spirometers (Microlab 3300 Spirometer; Micromedical, Kent, UK) were used for all measurements at all centres. Home PEF recordings were made using a Personal Best Peak Flow Meter (Health Scan Products Inc, Cedar Grove, NJ, USA) and were recorded as the best of three efforts in the morning and the evening.
Data analysis
The primary end point was the mean change from baseline in FEV1 recorded at 03.00 and 06.00 hours on the morning following the last dose of study medication on visit 4 (after 42 (3) days of treatment). Baseline FEV1 was derived from the measurements recorded at 03.00 and 06.00 hours before the administration of the study drug on visit 2 (day 1). The overall steady state bronchodilator efficacy of tiotropium was determined by the mean FEV1 response measured over a 24 hour time interval on visit 4. The mean FEV1 at baseline was calculated as the mean of the 3 hourly readings measured over 24 hours from 09.00 to 09.00 at visit 2. The mean response was defined as the difference between the mean FEV1 at baseline (visit 2) and the mean FEV1 at the end of treatment (visit 4).
The sample size calculation was based on data from previous studies of the effect of tiotropium on FEV1 in COPD.14 Assuming a standard deviation of 0.17 l for FEV1,21 a sample size of 30 patients per treatment group would be sufficient to detect a difference of 0.15 l in FEV1 between treatment groups at a 5% level of significance and 90% power using a two tailed t test.
Data are presented as mean (SD) for the population and SE for between-group comparisons. Analysis of covariance with terms for treatment and centre and baseline as a covariate was used as the statistical model for all efficacy analyses. The baseline value was included in the analysis of covariance model as a covariate to adjust for any baseline differences between treatment groups. Patients were excluded from individual analysis if adequate data were not available (for example, missing baseline data). Differences were accepted as being statistically significant at p<0.05. Circadian variation in peak flow and FEV1 was calculated as the difference between the highest and lowest values divided by the mean of the values available for that period—that is, all FEV1 measurements during the 24 hour period and all PEF measurements during the week of study. However, the study was not originally powered to examine circadian variation and the analyses performed for this evaluation were conducted post hoc.
RESULTS
Demographic data
Patient baseline features for the three treatment groups are presented in table 1⇓. The mean age for the groups combined was 65.8 years, 62% were men, and the group mean FEV1 was 1.08 l (40.8% predicted). The mean smoking history was 44 pack years, with 62% of the total population being ex-smokers. The groups did not differ in their pulmonary function or in their usual pulmonary medication before randomisation (table 1⇓).
Demographic characteristics of patients at screening (n=121)
Spirometric parameters
Forced expiratory volume in 1 second (FEV1)
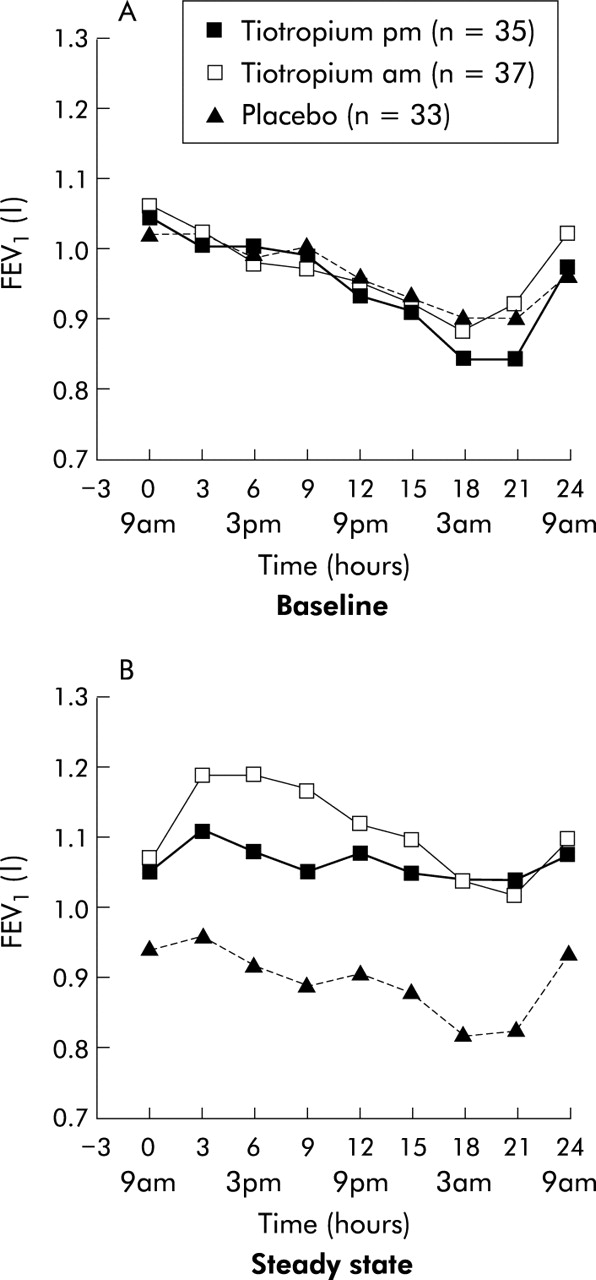
The mean (SE) nocturnal FEV1 (mean FEV1 at 03.00 and 06.00 hours) for the Tio-AM, Tio-PM, and placebo groups and the corresponding overall steady state FEV1 (mean over 24 hours) values are presented in table 2⇓. The differences from placebo in both the morning and evening dosing groups as well as the nocturnal FEV1 were statistically significant (p<0.05) at all time points on day 42. The baseline 24 hour spirometric recordings showed significant circadian variation in FEV1 in all three patient groups with the highest values recorded at 09.00 hours on the study day and the lowest values occurring at either 03.00 or 06.00 hours on the following morning (fig 1A⇓). The group mean change in FEV1 between 09.00 and 03.00 hours at baseline was: −180 ml in Tio-AM, −200 ml in Tio-PM, and −120 ml in the placebo group, corresponding to 03.00 hour absolute values of FEV1 of 0.88, 0.84, and 0.90 l, respectively. The mean FEV1 over the 24 hour day was 0.96, 0.95 and 0.96 l for the Tio-AM, Tio-PM, and placebo groups, respectively. The mean circadian variation for each group was 33.3%, 35.6% and 25.9%, respectively. There was considerable intersubject variability and these values did not differ statistically between the groups (ANOVA), but in the pairwise comparisons the variation in the Tio-PM group was higher than in the placebo group (p=0.03). However, the baseline variability before treatment was lower in the placebo group and this might influence the results.
Mean* (SE) nocturnal forced expiratory volume in 1 second (FEV1) and overall steady state FEV1 differences between treatment groups after 6 weeks of study drug

Mean forced expiratory volume in 1 second (FEV1) in litres over 24 hours (A) at baseline and (B) after 6 weeks (steady state) of tiotropium in the evening (pm), tiotropium in the morning (am), or placebo.
When the FEV1 profile was repeated after treatment, patients receiving placebo had a lower 24 hour mean FEV1 (0.91 (0.02) l) which was statistically lower than at the baseline visit (0.96 (0.02) l). On this occasion, the peak value occurred at 12.00 hours with the minimum FEV1 again being recorded between 03.00 and 06.00 hours on the following day, corresponding to an absolute FEV1 of 0.82 l (fig 1B⇑).
In both tiotropium groups the FEV1 increased significantly at all time points during the 24 hour observation period compared with placebo (fig 1B⇑). In patients treated with tiotropium the highest FEV1 now occurred at 12.00 hours, but the nadir remained between 03.00 and 06.00 hours. There was a non-significant trend towards a reduction in the magnitude of overnight decline in FEV1 compared with placebo when this was expressed as a percentage change from the mean at 09.00 hours (fig 2⇓), but not as an absolute change from the mean daily FEV1 value (Tio-AM=60 ml, Tio-PM=48 ml, placebo=56 ml).

Proportional nocturnal decline in forced expiratory volume in 1 second (FEV1) at baseline and after 6 weeks of study drug (steady state). Percentage decline in FEV1 = (FEV1 9 am − FEV1 3 am)/FEV1 9 am × 100.
Individual maximum variation was calculated as the difference between maximum and minimum FEV1 expressed as a proportional change from the minimum (100 × (maximum − minimum)/minimum). At baseline the mean maximum variation was 41.6%, 46.5%, and 30.2% for Tio-AM, Tio-PM, and placebo, respectively. After treatment the mean maximum variation declined in the Tio-AM (34.5%) and the Tio-PM (37.2%) groups but was similar to baseline in the placebo group (32.7%).
Forced vital capacity
The pattern of nocturnal FVC (mean FVC at 03.00 and 06.00 hours) and overall steady state FVC (mean over 24 hours) was similar to the FEV1 responses, and both tiotropium groups were statistically better than placebo (p=0.0001). The mean (SE) nocturnal FVC for the Tio-AM, Tio-PM, and placebo groups and the corresponding overall steady state FVC values are presented in table 3⇓. No statistically significant differences were seen between the two tiotropium dosing groups with respect to the nocturnal FVC (p=0.61) and overall steady state FVC (p=0.35). As with FEV1, the FVC profile after 6 weeks of treatment showed that both tiotropium groups were consistently better than the placebo group throughout the 24 hour observation period.
Mean* (SE) nocturnal forced vital capacity (FVC) and overall steady state FVC differences between treatment groups after 6 weeks of study drug
Peak expiratory flow
The mean morning and evening PEF during the baseline period were comparable across the three treatment groups (table 4⇓). The weekly mean morning and evening PEF for both tiotropium groups was statistically better than for placebo (p<0.02, fig 3⇓). For both tiotropium groups the mean weekly morning and evening PEF increased after 1 week on treatment, and remained consistently better than placebo throughout the 6 weeks of treatment.
Mean (SE) baseline weekly means for morning (PEF am) and evening (PEF pm) peak expiratory flow rates (l/min)

{kind=link}
{kind=link}
{kind=link}
The mean of the weekly means for (A) morning and (B) evening PEF (l/min) over 6 weeks of treatment with either tiotropium in the evening (pm), tiotropium in the morning (am), or placebo.
Adverse events
COPD exacerbations and upper respiratory tract infection were more common with placebo than with Tio-AM and Tio-PM, although the differences were not statistically significant. Exacerbations of COPD and upper respiratory tract infections were diagnosed by the physician and reported as adverse events. Eight patients (20.0%) in the placebo group had a COPD exacerbation compared with four patients (9.3%) in the Tio-PM group and one (2.6%) in the Tio-AM group. Six patients (15.0%) in the placebo group experienced upper respiratory tract infection compared with three (7.0%) in the Tio-PM group and one (2.6%) in the Tio-AM group. There were no differences in other adverse events in the tiotropium groups compared with the placebo group. Treatment with tiotropium was not associated with cardiac rhythm or heart rate abnormalities as assessed by 24 hour Holter monitoring.
DISCUSSION
Like many other biological variables, airway calibre exhibits a circadian variation during the 24 hour day with maximum values occurring around noon and the minimum values in the early morning.22 This variability is characteristic of bronchial asthma and is associated with increased levels of inflammatory mediators in the airways during sleep.16 The practice of defining variability by changes in morning and evening PEF has been transferred to patients with COPD where, contrary to the current definition of “relatively little variation in airflow calibre”,23 several studies have shown evidence of circadian variation.4,7,24–,27 Using the PEF in COPD is potentially misleading as the measurement is effort dependent and underestimates the impairment of FEV1 in COPD.19 Previous reports have significant limitations. They included only small numbers of patients and did not obtain measurements during the night.7,24,26 Some failed to include a control limb when studying bronchodilator effects24,26 or included patients with substantial degrees of bronchodilator responsiveness.4 This is the first study to document circadian variation in FEV1 in patients with stable COPD before and after a long acting inhaled bronchodilator and to include measurements during the early morning hours when FEV1 is lowest. Our findings have implications both for the mechanisms underlying this process and the interpretation of the results of treatment trials.
Studies of spirometric tests in normal subjects report a mean maximum change across the day of 200 ml in FEV1.28 Observations in a large population of healthy individuals whose FEV1 was measured on different occasions between 09.00 and 21.00 hours confirm that the peak values occurred around midday.29 They suggested that those who are older, smoke cigarettes, or have some respiratory symptoms show a more marked fall in FEV1 in the later evening. At baseline in our patients with COPD there was a mean (SE) daily FEV1 change of 286 (17) ml for the whole group with the maximum value in the late morning and the minimum in the early hours of the morning. This overall pattern was reproducible over the 6 weeks in the placebo group although the 09.00 value tended to be lower, possibly reflecting differences in the duration of effect of other permitted medications. The FVC data parallel those for FEV1 with no meaningful difference in the FEV1/FVC ratio throughout the 24 hour day, an observation supportive of consistent effort in performing the measurements throughout the day. The mean PEF was lower in the morning than in the evening throughout the 6 weeks in the placebo treated patients, varying by 13–17 l/min. These values are similar to those in the only other study to report patients of similar severity.7 These mean data mask significant between-week and between-individual variations and highlight the limitation of using measurements of circadian variation where the precise time of measurement is not known.
Lower respiratory system resistance in COPD rises significantly throughout sleep, independent of sleep stage30 and, although polysomnographic data were not included in the present study, our data are compatible with this. Increased cholinergic tone in the airway smooth muscle is believed to be a major contributor to this process, but data from the COPD patients treated with tiotropium indicate that this may not be the only factor involved. Tiotropium is an effective inhaled anticholinergic drug which can block methacholine challenge in patients with asthma for long periods.31 The mean FEV1 value over the 24 hour day increased after tiotropium and the absolute FEV1 was always higher at any time point after the active drug than the pretreatment baseline and placebo values. The timing of FEV1 variation also changed, with the highest FEV1 occurring between 12.00 and 18.00 hours, a pattern closer to that described in healthy individuals.32 Despite this improvement in absolute FEV1, the difference between the highest and lowest values during the day was similar after the active drug whenever given and resembled that reported in normal subjects.22 Whether this is due to changes in airway calibre in areas not reached by the inhaler, to different factors modulating airway smooth muscle activation, or simply differences in the control of lung volume or secretion clearance as proposed elsewhere33 cannot be resolved by our study.
The data illustrate some of the problems in interpreting bronchial reactivity indices in patients with a low baseline FEV1. If we relate the change in FEV1 after tiotropium administered at 09.00 hours to a specific time point as in fig 2⇑, reactivity appears to decline even though the absolute change from maximum to minimum is unaffected. Similar problems arise when other indices recommended in population studies are calculated.34 This emphasises the need to relate such variables to baseline lung function and helps explain the poor concordance between PEF changes and other measures of bronchial reactivity in patients with COPD.35
Although the timing of the dose of some drugs, such as corticosteroids in asthma,16,17 may influence the subsequent FEV1, this was not seen in these studies with tiotropium in COPD. The absolute change in FEV1 compared with baseline appeared smaller than that reported in some larger trials,36 but the changes relative to placebo were similar in magnitude. Nevertheless, the timing of the measurements can influence the end points selected. The 03.00 hours value had a mean difference of 220 ml in the Tio-AM and Tio-PM groups compared with placebo, while the 09.00 hours value had a mean difference of 130 and 110 ml, respectively. This dependence on timing may help explain why patients with COPD vary in response to the same drug in different studies.
In summary, we have found that circadian variations in FEV1 are present in patients with COPD. This is likely to contribute to the disturbed sleep seen in such patients and reflected in their daytime symptoms. Although the absolute change in FEV1 over 24 hours is close to normal, it comprises a proportionately greater amount of the waking value and this can complicate the interpretation of the usual measures of bronchial responsiveness. Our findings show that tiotropium once daily, whether administered in the morning or evening, results in sustained improvements in spirometric indices throughout the 24 hours, including improvement in the early morning nadir in spirometric values, without necessarily affecting circadian variability.
Acknowledgments
The authors acknowledge the contributions of the following investigators who participated in the study: Dr N M Foley, Royal United Hospital, Bath, UK; Dr N K Harrison, Morriston Hospital, Swansea, UK; Dr S J Langley, Wythenshawe Hospital, Manchester, UK; Dr B R O’Driscoll, Hope Hospital, Salford, UK; Dr J A van Noord, De Wever Hospital, Heerlen, The Netherlands; Dr R J White, Frenchay NHS Trust, Bristol, UK; Dr A J Winning, West Middlesex University Hospital, Isleworth, UK.
REFERENCES
Supplementary materials
. Publisher Correction
Please note that there is an error in the author list, The name of the senior author, Dr Kesten, was spelt incorrectly.
The correct author list is shown here:
PMA Calverley, A Lee, L Towse, J van Noord, TJ Witek, and S KestenThe error is much regretted.
Footnotes
PMAC contributed patients to the study,helped develop the data analysis plan and wrote the manuscript together with SK. JvN contributed patients, LT organised the study implementation and AL undertook the statistical analysis. All authors contributed to development of the study protocol, data interpretation, and to the final manuscript.
The study was supported by Boehringer Ingelheim Pharmaceuticals Inc.