Article Text

Statistics from Altmetric.com
INTRODUCTION
Need for recommendations on respiratory aspects of fitness to dive
Diving has long been performed for commercial and military purposes but it has undergone a dramatic increase in popularity as a leisure pursuit over the past 30 years. It is estimated that, in the United Kingdom, 100 000 individuals participate in diving activities. In addition, diving technology has evolved rapidly, allowing divers to descend to greater depths and to dive in places which would previously have been impossible. As a sport, diving can be physically and emotionally demanding, and is associated with some specific risks. Medical practitioners are increasingly likely to be faced with requests to comment on fitness to undertake diving. Many of these requests relate to respiratory aspects of fitness. A number of existing guidelines or discussion papers on respiratory aspects of fitness to dive are in existence.1–3 However, the advice given in these is not consistent and these documents may not be readily available to the practising physician or general practitioner. The British Thoracic Society (BTS) Standards of Care Committee therefore established a Working Party to formulate national recommendations for assessing respiratory fitness to dive. This guideline is intended to provide respiratory physicians and physicians interested in diving medicine with a practical framework on which to base advice. The UK Sport Medical Diving Committee advises the British Sub Aqua Club, the Sub Aqua Association, and the Scottish Sub Aqua Club on aspects of fitness to dive. It has recently introduced a questionnaire-based declaration of fitness for prospective members of these organisations and advises that medical examination is required only when positive responses to the questionnaire are obtained. Commercial and military diving are subject to additional specific regulations.
Purpose of recommendations
-
To promote understanding of the factors which influence respiratory fitness to dive.
-
To provide an authoritative up to date literature review of available evidence.
-
To provide practical evidence-based advice for healthcare professionals who may be asked to provide advice on respiratory aspects of fitness to dive.
-
To describe situations in which further specialist advice is required and to indicate sources of appropriate advice.
Methods of production
The Working Party determined the target and purpose of the recommendations. A literature review was then performed using a number of search strategies. Topics examined in the literature review included (1) the diving environment and physiological effects of diving, (2) diving related illness, (3) diving deaths and adverse events (epidemiology), (4) specific respiratory conditions and diving, and (5) specialist organisations and advice sources.
Databases searched were Medline (1966–2000), Embase (1980–2000), Cinahl (1982–2000), the Cochrane Library database, Healthstar (1975–2000), and Sportdiscus (1949–2000). The following diving related websites were also searched: British Sub Aqua Club (www.bsac.com), BSAC Diving Incident Reports (http://www.bsac.com/techserv/increp99/intro.htm), Scottish Sub Aqua Club (http://www.scotsac.com), Divers Alert Network (http://www.diversalertnetwork.org), Professional Association of Diving Instructors (http://www.padi.com), Diving Medicine Online (http://www.gulftel.com/∼scubadoc), and South Pacific Underwater Medical Society (http://www.spums.org.au).
Keywords used in the searches were: dive, diving, barotrauma, respiratory disease, hyperbaric, asthma, COPD, sarcoidosis, emphysema, bronchitis, pneumothorax, fitness, pulmonary, SCUBA, underwater, Trimix, Nitrox, hyperbaric oxygen.
Papers identified were reviewed independently by two members of the Working Party, graded according to the Scottish Intercollegiate Guideline Network (SIGN) guideline criteria for levels of evidence, and recommendations were developed from the literature review according to SIGN principles (see Appendix 1). A draft document was prepared by the Working Party. This was then circulated to the BTS Standards of Care Committee and to selected reviewers listed in Appendix 2. The draft document was displayed for one month on the BTS website. A final draft was then prepared incorporating feedback from all these sources.
Interests of guideline developers
There are no perceived conflicts of interest. Dr Farrell is a member of the UK Sport Diving Medical Committee; Dr Watt advises on fitness to dive for commercial divers.; Dr Wilmshurst is a member of the UK Sport Diving Medical Committee and acts as a medical consultant and paid column writer for Diver Magazine; Professor Denison is a Civil Consultant in Applied Physiology to the Royal Navy, a Scientific Advisor to the Royal Navy on Submarine Escape, and a referee for the Health and Safety Executive on appeals concerning fitness to dive.
SUMMARY OF KEY POINTS AND RECOMMENDATIONS
The diving environment
-
Diving is an arduous underwater activity in which environmental conditions affect bodily structure and function.
-
For every 10 metres descent in sea water, ambient pressure increases by 100 kPa, equivalent to 1 atmosphere (1 bar). The volume of a given mass of gas changes inversely in proportion to pressure. The gas in bodily cavities such as the lungs, sinuses, middle ear and intestine is therefore subject to compression during descent and expansion during ascent. This may lead to tissue damage.
-
Partial pressure of gases increases in direct proportion to the increase in ambient pressure. Greater quantities of inert gas, mainly nitrogen, therefore dissolve in tissues at depth and come out of solution on ascent.
-
The density of inhaled gas increases with pressure, restricting breathing.
-
Immersion displaces blood from the periphery into the thorax, reducing lung volume.
-
Work of breathing increases due to a combination of increased gas density, increased hydrostatic pressure, and altered respiratory mechanics.
-
Underwater breathing apparatus adds dead space and increases resistance to breathing.
-
During diving, carbon dioxide retention may result from the above listed effects on the body.
Potential risks of diving
-
General risks: panic, hypothermia, physical trauma, and drowning.
-
Equipment/technique problems: hypoxia, hyperoxia, or poisoning by inappropriate gas mixtures or contaminant gases may result from equipment malfunction or poor dive planning. A malfunctioning respiratory regulator may result in aspiration.
-
Barotrauma: is caused by compression or expansion of gas filled spaces during descent or ascent, respectively. Compression of the lungs during descent may lead to alveolar exudation and haemorrhage. Expansion of the lungs during ascent may cause lung rupture leading to pneumothorax, pneumomediastinum, and arterial gas embolism.
-
Decompression illness: may occur when gas, which has dissolved in tissues while at depth, comes out of solution as bubbles. Clinical manifestations vary, the most severe being cardiorespiratory and neurological.
-
Loss of buoyancy control: is a cause of many accidents, usually when it leads to rapid uncontrolled ascent.
It is also essential to consider comorbidities such as diabetes and epilepsy which may influence capability for diving but are outside the scope of this document.
The physician should bear the following general concepts in mind when assessing respiratory fitness to dive:
The subject may be required to swim in strong currents.
The subject may be required to rescue a companion (dive buddy) in the event of an emergency.
The diving environment is associated with a risk of lung rupture.
The gas breathed by the diver may be very cold.
Buoyancy control is essential and requires training, experience, and use of appropriate equipment.
The following recommendations are therefore made.
Assessment of respiratory fitness to dive
-
In the history, particular attention should be paid to current respiratory symptoms, previous history of lung disease including childhood history, previous trauma to the chest, and previous episodes of pneumothorax. [B]
-
Respiratory system examination should be performed. [B]
-
Forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and peak expiratory flow rate (PEF) should be measured. [C] FEV1 and PEF should normally be greater than 80% of predicted and the FEV1/FVC ratio greater than 70%.
-
Routine chest radiography is not considered necessary in asymptomatic subjects with no significant respiratory history and normal examination findings. [C] However, all professional divers, including recreational divers, who plan to work as instructors are recommended by the Health and Safety Executive to undergo prior chest radiography.
-
Chest radiography is appropriate if there is a previous history of any significant respiratory illness—for example, pleurisy, pneumonia, recurrent respiratory infections, sarcoidosis, chest surgery or trauma, pneumothorax—and in those with current respiratory symptoms and/or abnormal examination findings. [C]
-
Routine measurement of the expiratory flow-volume loop, exercise testing, or bronchial provocation testing are not considered necessary although these tests may be useful in specific cases. [C]
-
Thoracic CT scanning, which has greater sensitivity than standard chest radiography to detect lung structural abnormality, may be useful in specific cases. [C]
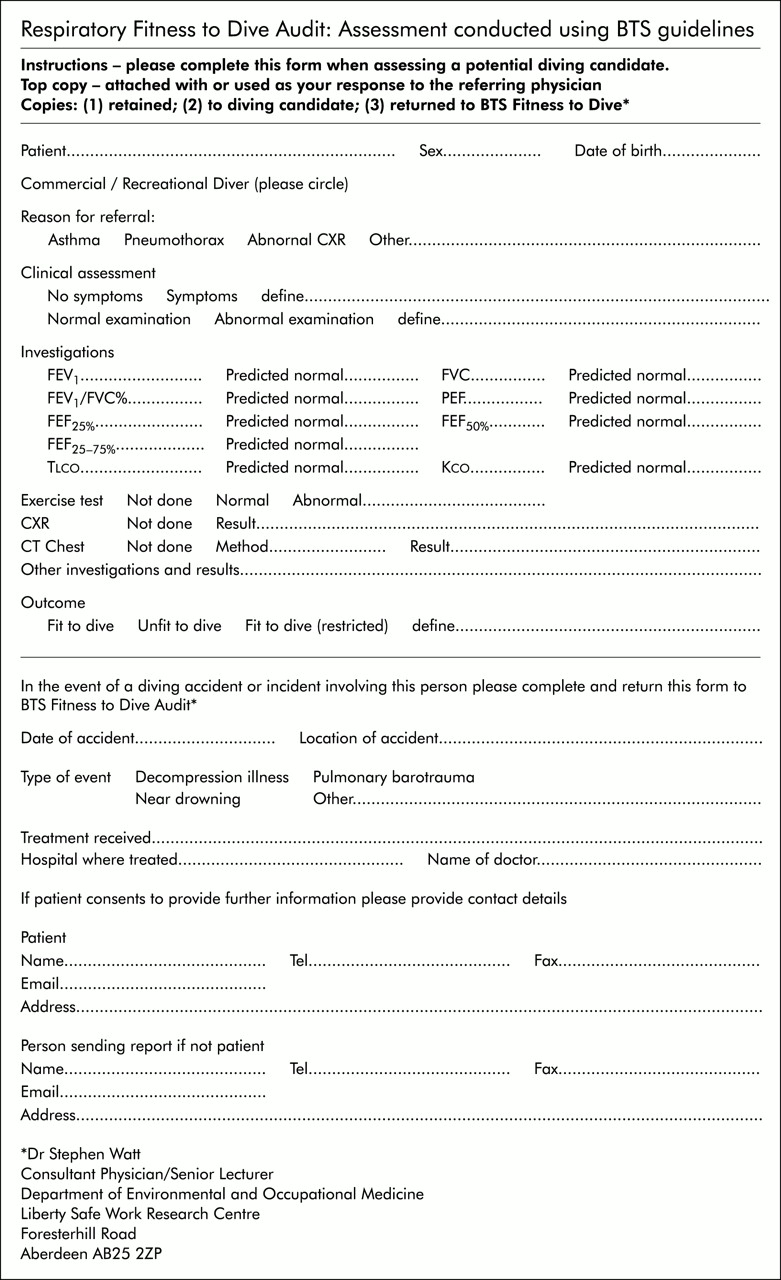
An algorithm assessing respiratory fitness for diving is shown in fig 1. A specimen recording form, which could also be used for audit purposes as discussed in Appendix 3, is shown in fig 2.
Recommendations on specific respiratory conditions
-
Lung bullae or cysts increase risk of barotrauma and are contraindications to diving. [B]
-
Previous spontaneous pneumothorax is a contraindication unless treated by bilateral surgical pleurectomy and associated with normal lung function and thoracic CT scan performed after surgery. [C]
-
Previous traumatic pneumothorax may not be a contraindication if healed and associated with normal lung function, including flow-volume loop and thoracic CT scan. [C]
-
Subjects with asthma should be advised not to dive if they have wheeze precipitated by exercise, cold, or emotion. [C]
-
Subjects with asthma may be permitted to dive if, with or without regular inhaled anti-inflammatory agents (step 2 of the BTS guidelines4), they: [C]
-
are free of asthma symptoms;
-
have normal spirometry (FEV1 >80% predicted and FEV1/VC ratio >70% predicted); and
-
have a negative exercise test (<15% fall in FEV1 after exercise).
-
-
Subjects with asthma should monitor their asthma with regular twice daily peak flow measurement and should refrain from diving if they have: [C]
-
active asthma—that is, symptoms requiring relief medication in the 48 hours preceding the dive;
-
reduced PEF (more than 10% fall from best values);
-
increased peak flow variability (more than 20% diurnal variation).
-
-
COPD carries a theoretical increased risk of barotrauma and reduced exercise tolerance. Subjects will probably be advised against diving on the basis of reduced pulmonary function (FEV1 <80% predicted). [C]
-
Sarcoidosis has been associated with pulmonary barotrauma. Diving is contraindicated in subjects who have active sarcoidosis. Those in whom sarcoidosis has resolved should have normal chest radiography and pulmonary function testing before being advised that they may proceed with diving. [C]
-
Tuberculosis is a potentially transmissible disease that may cause residual impairment of lung structure and function. A subject with active tuberculosis should not dive. After curative treatment they may dive if lung function and chest radiograph are normal. [C]
-
Cystic fibrosis is often associated with abnormal pulmonary function and increased risk of pneumothorax. Diving is contraindicated in those patients who have pulmonary involvement. [C]
-
Fibrotic lung disease reduces lung compliance and impairs gas transfer. Diving is therefore contraindicated in subjects who have fibrotic lung disease. [C]
Long term effects of diving on the lung
-
Divers tend to have large lung volumes with proportionately greater increases in vital capacity than in FEV1. This may be attributable in part to the effects of repeatedly breathing dense gas through increased resistances. [III]
-
Divers may have reduced expiratory flow rates at low lung volumes, possibly reflecting small airway disease. [III]
-
Vital capacity of divers may decline with age at an increased rate. [III]
-
Saturation diving causes a fall in carbon monoxide transfer which, once the dive is completed, gradually returns to pre-dive values. [IIb]
Sources of specialist advice
In the United Kingdom, advice on sports diving may be sought from the medical referees of the British Sub Aqua Club, the Scottish Sub Aqua Club, or the Sub Aqua Association. Information is available on the UK Sport Diving Medical Diving Committee website (http://www.uksdmc.co.uk). The Royal Navy Institute of Naval Medicine is also willing to discuss cases with both divers and physicians.
The Health and Safety Executive (HSE) is responsible for commercial diving policy and regulation. Individuals who are diving at work require a current HSE certificate of fitness to dive following examination by an approved medical examiner of divers.
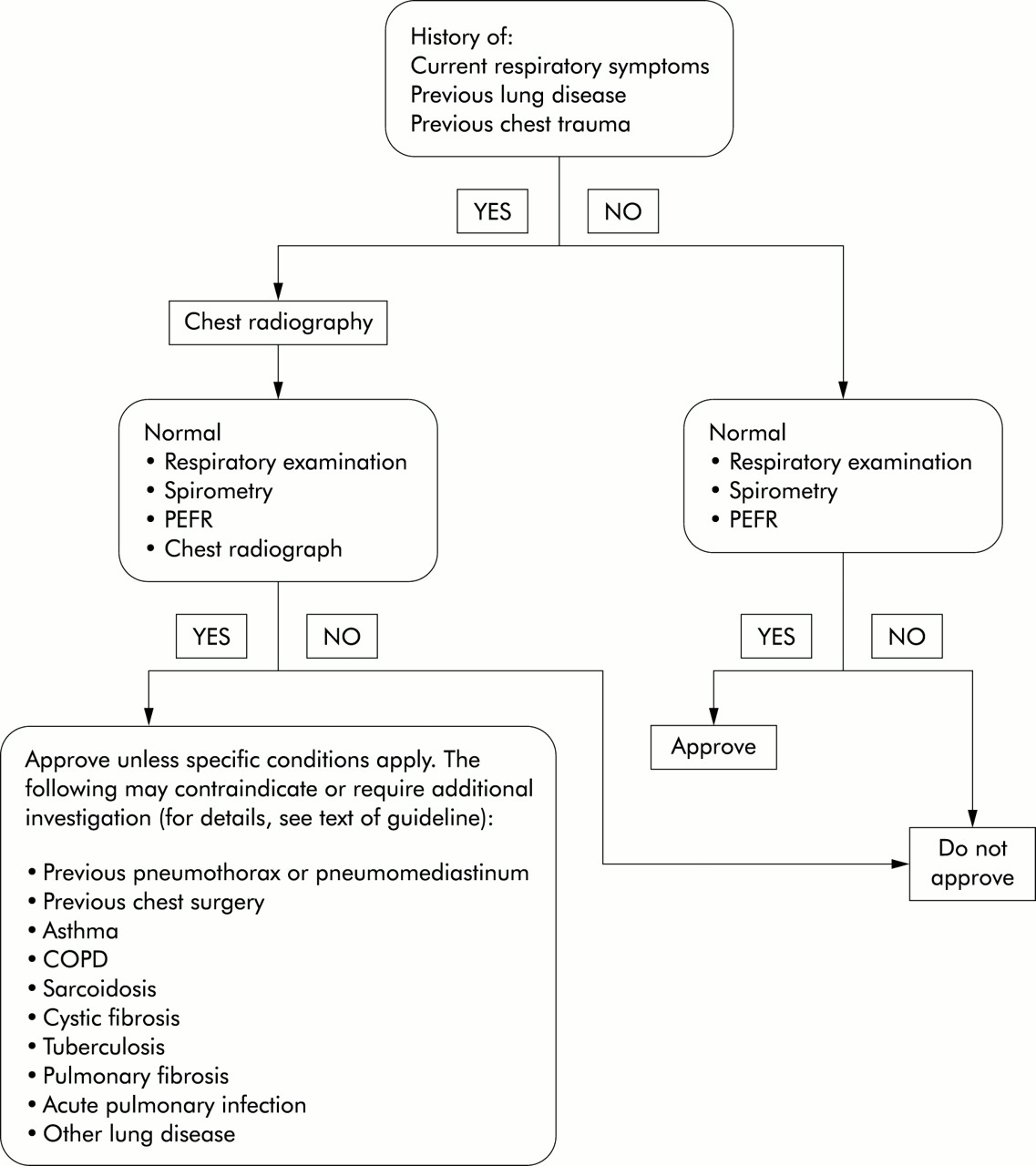
Algorithm assessing respiratory fitness for diving.
{kind=link}
{kind=link}
Specimen form for recording and auditing purposes.
BACKGROUND LITERATURE REVIEW
The diving environment and physiological effects of diving
Diving is an arduous underwater activity in which environmental conditions affect bodily structure and function. Anyone undertaking diving may be required to swim in a fast current and to rescue a companion (dive buddy) in the event of an emergency.
They must also be able to cope with the physical stresses imposed by the underwater environment. To understand the principles behind fitness to dive, a simple understanding of diving physics and physiology is helpful. More detailed information can be gained from standard diving textbooks.5–8
Pressure-volume relationships
On land at sea level, man is exposed to an ambient pressure of 1 bar (equivalent to 1000 millibar, 750 mm Hg, or 100 kPa). Under water, because of the relative incompressibility of water associated with its high density, pressure rises rapidly and linearly with depth such that, for every 10 metres of sea water (msw) descent, pressure increases by 1 bar. As a consequence of the volume-pressure relationships described by the gas laws, for a given mass of gas an increase in pressure is associated with a reduction in volume. Thus, gas contained in any space within the body (e.g. lungs, sinuses, middle ear, intestine) will be compressed during descent and expand during ascent. In a breath hold diver, an intrathoracic gas volume of 6 litres at sea level would be compressed to 2 litres at 20 metres depth (3 bar) and 1.5 litres at 30 metres depth (4 bar). Similarly, a closed pneumothorax comprising 1 litre volume developing in a diver at 30 metres depth (4 bar) would expand to occupy a volume of 4 litres as the diver ascended to the sea level (1 bar), potentially a life threatening situation. A diver using breathing apparatus underwater retains relatively normal lung volumes but needs to breathe a much greater mass of gas while at pressure.
Partial pressure relationships
Breathing room air at sea level, the partial pressure of nitrogen (pN2) is 0.78 bar and oxygen (pO2) is 0.209 bar with small contributions from other gases. If the diver descends to 10 msw (2 bar) breathing air pN2 rises to 1.56 bar and pO2 to 0.418 bar. While gas fractions are frequently used in medicine to specify gas mixtures, the body’s physiological response is to partial pressure. Thus, breathing air at 10 msw produces the same oxygen tension and physiological effect as breathing 42% oxygen at sea level. One consequence of this increase in partial pressure is that proportionately more gas dissolves in the tissues. If the diver ascends at a rate that exceeds the body’s capacity to clear this excess gas, inert gas bubbles may form leading to decompression illness.
Gas density effects
Increased ambient pressure results in increased gas density which, in turn, results in an increase in the work of breathing and a reduction in breathing capacity, proportional to the depth at which the subject is located. For example, at a simulated depth of 30 metres in a hyperbaric chamber, maximum voluntary ventilation is reduced by more than 50% from surface values.5
Immersion in water
Immersion in water has several physiological consequences. When upright, the additional hydrostatic pressure on the dependent limbs forces blood into the chest resulting in an increase in intrathoracic blood volume of about 700 ml.9 Cold exposure produces a similar effect. The consequent increase in right heart pressure triggers a diuresis and loss of plasma volume. Ventilation perfusion matching may be affected and a mechanical reduction in lung volume of about 300 ml vital capacity occurs.10 In diving, variations in posture may alter these values. Work of breathing also increases and varies with posture.
Use of breathing apparatus
Breathing apparatus used during diving results in an increase in dead space, increased inspiratory and expiratory resistance, and therefore an increase in work of breathing related to the equipment.11 This compounds the increase associated with breathing dense gas. When associated with immersion12 these factors may result in a degree of carbon dioxide retention.
Types of diving
The simplest form of diving is breath hold diving in which no equipment is used and the duration and depth of dive is determined by the individual’s ability to sustain and remain functional during a single breath hold. However, most recreational diving is performed using breathing apparatus such as SCUBA (self contained underwater breathing apparatus) containing air. In recent years, gas mixtures containing varying concentrations of oxygen and nitrogen and, in some cases, other inert gases such as helium have been introduced to recreational diving. Closed and semi-closed circuit breathing apparatus are also used by a few recreational divers. Details of these techniques are beyond the scope of this guideline, as are commercial and military techniques such as surface supplied air diving and saturation diving. However, the principles of assessing fitness to dive are in general unaffected by the type of apparatus or gas mixture to be used.
As an illustration of the environment which the diver might face, consider the situation of a recreational diver breathing air from SCUBA equipment at 20 metres depth in sea water off the coast line of the UK. The environment has limited visibility and is cold (average temperature 5–10°C) requiring suitable protective clothing. The diver is breathing cold gas, which has greater density than on the surface, through equipment imposing both increased inspiratory and expiratory resistance and increased dead space. The work of breathing is further increased by the increase in intrathoracic blood volume and consequent small airway closure. The partial pressures of oxygen and nitrogen or other gases the diver is breathing are three times greater than those on the surface. The diver is exercising for propulsion and other physical tasks, and has a tendency to carbon dioxide retention. The depth and duration of the dive is limited by the need to offload inert gas during the ascent phase of the dive, without causing bubble formation sufficient to cause decompression illness. These inert gases, principally nitrogen, have dissolved in the body tissue during the dive. During descent and ascent, changes in volumes of gas filled spaces in the body may lead to tissue injury known as barotrauma. Other potential risks to the diver include equipment failure, physical trauma, and drowning in the event of equipment malfunction. Because of this potentially hostile environment, adequate training is essential for all recreational divers as well as those diving professionally.
Long term effects of diving on the lung
Divers have larger lung volumes than standard reference populations.13,14 The most consistent finding is a greater increase in forced vital capacity (FVC) than in forced expiratory volume in 1 second (FEV1),15 leading to a reduced FEV1/FVC ratio. This may be in part related to natural selection of those wishing to dive,16 but also to repetitive breath holding and resistive breathing during diving activities. Despite these increases in lung volumes, a number of studies have shown reduced expiratory flows at low lung volumes, possibly indicating pathological changes in the lung periphery.15,17 In a cross sectional study of 180 healthy male divers and 35 control subjects, Tetzlaff et al18 found that the divers had lower mid-expiratory flow values at 25% of vital capacity than controls and that their mid expiratory flows at 25% and 50% of vital capacity were inversely related to years of diving. In a more recent study of 87 divers followed during the first three years of their commercial diving career, mean FEV1 fell by 1.8% and mean forced expiratory flow at 75% of vital capacity (FEF75%) by 10.4% over the three year follow up period, indicating changes in small airway function.16 To test whether structural changes could be demonstrated in life, Reuter et al compared divers and non-diving controls using high resolution CT scanning.19 Mild emphysema was found in about one quarter of both divers and controls. Air trapping and interstitial changes also did not differ between divers and controls. Limited data from longitudinal studies of commercial divers suggest that lung volumes decline at a faster than expected rate.20 Acute exposure to a deep saturation dive results in a loss of transfer factor (diffusing capacity) which may recover over time.21,22 This has been attributed to low level oxygen toxicity occurring as a result of breathing increased partial pressures of oxygen at depth, and to the effects of bubbles on the pulmonary circulation.
Diving related illness
Any form of intercurrent acute illness may of course develop during diving. Trauma, oxygen toxicity, or hypoxia due to equipment malfunction or poor dive planning and hypothermia are also potential risks for the diver. Useful brief outlines of diving related medical problems have been provided.23–25 In this section, however, we will describe three specific types of diving related illness—barotrauma, decompression illness, and pulmonary oedema associated with immersion (a rarer event).
Barotrauma
Barotrauma is the consequence of compression or expansion of a gas filled body cavity during descent or ascent, respectively. The space between a diver’s suit and body may also undergo such changes. Organs particularly at risk include the ear, lungs, sinuses, intestine, and skin (due to suit compression).
Compression of the lung during descent in a breath hold dive (lung squeeze) or rapid descent when breathing equipment has failed may lead to alveolar exudation, haemorrhage, and wall rupture leading to cough, haemoptysis, and dyspnoea.26,27 This is rare.
Barotrauma of the lung (burst lung) on ascent is more frequent and serious. A diver using compressed gas at depth breathes at lung volumes similar to those on the surface. During ascent, the volume of the gas in the lungs expands and the diver must exhale to allow gas to escape. If anything impedes exhalation, either at whole lung or segmental level, the lung may rupture. This may also occur if very large breaths are taken or if an intermittent pattern of breathing (“skip breathing”) is adopted. Gas then tracks to the hilum and mediastinum, the retroperitoneum or the pleural space. Gas may also enter the pulmonary venous system leading to gas embolism into the systemic circulation, a potentially fatal situation. Fatal cases of barotrauma where gas has been found in the central circulation have been described.28 The risk of pulmonary barotrauma is increased where there is localised or generalised airway narrowing, bulla formation, or any localised weakness of the lung parenchyma. The risk of pulmonary barotrauma during submarine escape tank training is inversely related to FVC measured before training.29
The most common situations in which barotrauma of ascent occurs are where compressed gas supply runs out at depth, or during loss of buoyancy control when a rapid uncontrolled ascent may occur. A number of clinical presentations are possible. Pneumomediastinum usually presents with central chest discomfort, hoarseness, and dyspnoea. Arterial gas embolism may present with any combination of major neurological symptoms and signs together with impairment of consciousness, convulsions, and sudden death due to coronary embolism. There have been numerous case reports of barotrauma which demonstrate the variable circumstances in which it may occur. For example, Weiss and van Meter30 described two cases of cerebral air embolism in asthmatics undertaking scuba dive training in a swimming pool. In these subjects asthma was thought to be the major risk factor. In some cases no prior risk factor can be identified. Carpenter31 described a 27 year old man who had two episodes of barotrauma 6 months apart with four uneventful pressure exposures in a chamber between these episodes. This subject had a normal high resolution CT scan of the chest, a normal ventilation scan, and negative methacholine challenge test. Serious barotrauma can occur after shallow dives as might be expected from the pressure-volume relationships which require large volume changes for a given change of pressure close to the surface. Friehs et al32 described a subject who developed pneumomediastinum, bilateral pneumothorax, and air embolism with subsequent paraparesis after a dive to 5 meters. Barotrauma of ascent has been described after a breath hold dive.33 The mechanism here is unclear, but has been attributed to differential expansion of lung subsegments leading to rupture. If pneumothorax occurs at depth and ascent continues, the risk of tension is significant due to continued expansion of the gas in the pleural cavity.
In a report on records of the Institute of Naval Medicine over a 20 year period (1965–84),27 140 cases of pulmonary barotrauma, including one death, were recorded. Of these, 23 were associated with respiratory manifestations only, 58 had signs of arterial gas embolism, and the remainder had arterial gas embolism without respiratory signs or symptoms at presentation. The relationship between underlying lung disease and the occurrence of barotrauma remains contentious. In a report on necropsy findings in deceased divers and experimental pressure exposures on human cadavers,34 pleural adhesions and lung bullae were a constant finding in those with pneumothorax. However, up to 26% of lungs from control subjects, who had died for other reasons, also had pleural adhesions. In cases of barotrauma there was no constant association between lung scars or fibrous tissue and the site of barotrauma. The suggestion was therefore made that, once barotrauma had recovered, the subject should not necessarily be excluded from further diving. The interpretation of necroscopic studies is always complicated by the issue of whether lung cysts, bullae, or pleural lesions antedated the episode which caused the death. In early experimental models of barotrauma induced by raising intratracheal pressure in dogs35 it was found that interstitial emphysema and air embolism occurred above pressures of 80 mm Hg. Binding of the thorax and abdomen protected against these complications, allowing intratracheal pressure to be raised to 180 mm Hg. These experiments suggested that, rather than absolute intratracheal pressure, transpulmonary pressure and transatrial pressure were the more important determinants of risk. Experiments on human cadavers, both unbound and bound, produced similar figures for intratracheal pressure and risk of rupture.34,36 The nature of an individual’s lung mechanics may be related to risk. In a study of 14 men who had suffered pulmonary barotrauma, Colebatch and Ng37 showed that these individuals had less distensible lungs and airways than healthy divers and non-smoking non-divers. They suggested that the relative stiffness of the airways increased the elastic stresses in the peribronchial alveolar tissue leading to an increased risk of alveolar rupture. It has been suggested that the increase in thoracic blood volume during immersion may compound this problem by further reducing lung distensibility.38
Is there evidence that lung function testing can predict the risk of barotrauma? In a comparison of pre-dive lung function tests from 13 divers who had developed pulmonary barotrauma with 15 divers who had developed decompression illness without pulmonary barotrauma, Tetzlaff et al39 found that those with pulmonary barotrauma had lower mid-expiratory flow rates at 50% and 25% of vital capacity. In four of those with pulmonary barotrauma, CT scans performed after the injury revealed subpleural blebs or cysts which were not evident on radiographs performed before or after the injury, and in two of these patients follow up scans several months later40 showed no change in the blebs. In a group of four divers who suffered pulmonary barotrauma at or near the surface, three had abnormal pulmonary function (reduced flow rates at low lung volumes and reduced carbon monoxide transfer factor) measured 4 weeks or more after the incident.41 In only one of these was pre-injury lung function available and it had been normal at that time.
The literature on pulmonary barotrauma comprises mainly isolated case reports and small case series such as these. In an interesting study of amateur divers who had suffered neurological symptoms within 5 minutes of surfacing from an apparently “safe” dive, Wilmshurst et al identified a group who had an intracardiac shunt (a recognised risk factor), and another group with no shunt.42 Among the latter group 50% had abnormalities of the flow-volume loop, suggesting small airway disease, and 55% were smokers. The history of the neurological episodes in this group suggested that they had suffered barotrauma and air embolism. However, this study indicated that, in 50% of subjects, no abnormality of lung function was detectable. Thus, while a significant proportion of these subjects had abnormal function, it is apparent that FEV1 and FVC values within the predicted normal range do not exclude an individual from developing pulmonary barotrauma. Firm conclusions on the relationship between pulmonary barotrauma and pre-existing lung function or structural abnormality cannot be made, as has been highlighted by Russi.43 Whether screening by measurement of airflow at low lung volumes is of greater value44 remains contentious.45
Prognosis is variable but may be improved by rapid recompression. In the series of diving accidents over a 20 year period (1965–1984) recorded by the Institute of Naval Medicine27 in which 140 cases of pulmonary barotrauma were reported, 12 cases of recurrent barotrauma were described.46 Review of these cases suggested that recurrence seemed to be more severe than the original incident. Prevention of pulmonary barotrauma depends on diver training to prevent situations leading to barotrauma and on medical screening to prevent those at increased risk from diving. This therefore underlies much of the respiratory assessment of fitness to dive.
Decompression illness
The lung, specifically the pulmonary circulation, plays a major role in the prevention of decompression illness. Decompression illness occurs as a result of bubble formation during or after ascent as inert gas, dissolved in the diver’s tissues at depth, comes out of solution. The symptoms of decompression illness may include limb pains (the bends), fatigue, malaise, and a wide range of neurological symptoms. Bubbles forming in the tissues may reach capillaries and are then transported to the lungs. If the lung circulation is intact and no shunting of blood occurs, the majority of bubbles are filtered at the pulmonary capillary level. If a large volume of bubbles forms, then the pulmonary circulation itself may be compromised leading to pulmonary decompression illness (“the chokes”). This may present with chest tightness, cough, dyspnoea, and a fall in systemic blood pressure. If there is any anatomical shunt—such as an atrial septal defect, patent foramen ovale or intrapulmonary shunt—or a physiological shunt which may occur when the volume of bubbles is large, bubbles may access the systemic circulation and travel to the tissues causing skin, cardiovascular, or neurological abnormalities.47,48 There is some evidence that pulmonary abnormalities are associated with an increased risk of decompression illness and obstructive airway disease has been identified as an independent risk factor. Bubble formation within the circulation is associated with many secondary phenomena such as complement and platelet activation leading to the formation of microemboli and altered endothelial function. The exact symptom complex produced by such bubbles depends on their final resting place in the systemic circulation, and the inert gas (nitrogen) content of the tissues embolised, which determines the ability of the tissues to amplify embolic bubbles. Symptoms may range from relatively trivial aches and pains, through focal neurological deficits to collapse, convulsions, and death.
Pulmonary oedema associated with immersion
Several reports have described acute pulmonary oedema in divers during the course of a dive and also in swimmers.49–52 The diver usually develops increasing cough and breathlessness while underwater. This often becomes more marked during the ascent phase of the dive, partly as a result of the falling oxygen tension in the breathing gas, and may continue to deteriorate after surfacing. Haemoptysis often occurs and symptoms may persist for 24–48 hours after the dive. Chest radiographs show patchy alveolar oedema consistent with the appearance of adult respiratory distress syndrome. The cause remains unclear but some divers have repeated episodes, supporting the likelihood of individual susceptibility. It appears more common in older divers and there is an association with hypertension. The underlying cause may be haemodynamic disturbances associated with immersion but cold, prior respiratory tract infection, or water inhalation may act as precipitating factors. Because of the risks associated with the onset of acute breathlessness while in the water, individuals with this history should be advised against further diving.
Diving deaths and adverse events: epidemiology
Precise statistics on diving deaths and adverse events are not available because of incomplete recording and the difficulty of ascertaining numbers of individuals undertaking recreational diving. The literature contains many case reports and short case series describing specific diving fatalities and their circumstances. Diving organisations such as the British Sub Aqua Club (BSAC) and Divers Alert Network (DAN) operate reporting systems. However, it is impossible to calculate fatality rates due to the imprecision of a voluntary reporting system and the difficulty of ascertaining the number of individuals actively participating in sport diving at any time. In 1995 membership of the BSAC was 52 364, an estimated 3 million dives were performed, and 351 adverse incidents were reported including 18 fatalities.53 It is likely, however, that this is an underestimate of adverse events. In a review of military diving between 1968 and 1981, 1174 adverse events were reported from 706 259 dives.54 Of the adverse events, decompression illness comprised 41%, barotrauma 22%, pneumothorax 0.3%, and mediastinal emphysema 0.8%. There was a relationship between dive depth and accident rate, the greatest risk occurring at depths greater than 30 metres. However, these figures relate to diving practices of more than 20 years ago. In addition, military diving procedures may differ substantially from civilian recreational practices. Estimates of diving adverse events in the United States are quoted by Twarog et al.55 The number of divers is estimated at between 600 000 and 3 million, performing up to 30 million dives per year, with reports of decompression illness or arterial gas embolism estimated at 500–600 per year, giving an overall risk of 0.017–0.2%. The wide ranges quoted indicate the potential inaccuracy of these figures. In a report of figures from the National Underwater Accident Data Centre (NUADC) in the United States, 67 recreational scuba fatalities were reported in 1991, with an estimated fatality rate of 2.09–2.68 per 100 000 participants.56 This report highlights the varied procedural, technical, and external factors that may lead to fatalities—such as buoyancy problems, insufficient air, entrapment, and the effects of drugs and alcohol as well as underlying medical problems. In the same time period, Divers Alert Network in the United States received reports of 708 episodes of decompression illness involving American divers, of whom 26% had a current medical problem. There is some evidence that diving accident rates may be increasing. Reported episodes of decompression illness affecting members of diving clubs in the UK between 1981 and 1993 showed an increase from about one case to two cases per 1000 members, an associated survey suggesting that the number of dives undertaken was also increasing.57 In a report from Leicester of accidents occurring in an inland diver training centre where activity is logged, the accident rate increased from 4/100 000 dives in 1992 to 15.4/100 000 dives in 1996.58 However, the actual numbers involved were small. A more recent report from the year 2000 in Orkney, a major recreational diving centre where the majority of open water dives are to 30–40 metres, suggests a much higher accident rate. The incidence of decompression illness was 0.49/1000 dives while that of significant dive related accidents was 0.8/1000 dives.59
Specific respiratory conditions and diving
Pneumothorax
The development of a pneumothorax at depth is associated with great risk since, during ascent, the volume of gas within a closed pneumothorax will expand according to Boyle’s law, creating tension. Subjects with certain lung diseases such as emphysema and cystic fibrosis (relatively common), Ehlers-Danlos syndrome and histiocytosis X (rare) are at increased risk of a first episode of pneumothorax. However, spontaneous pneumothorax is well recognised in young apparently fit individuals and is associated with a significant risk of recurrence. In a questionnaire survey of 112 US aircrew personnel who had suffered a spontaneous pneumothorax, 28% reported a first recurrence, 23% of those a second recurrence, 14% of those a third recurrence, for a total recurrence rate of 35%.60 Since 67% of these subjects had chest drainage, with or without other procedures, for their first pneumothorax, this recurrence rate is likely to be lower than would be expected without intervention. In a UK study of 153 patients presenting to hospital with primary spontaneous pneumothorax, 54% developed recurrence, of which about one quarter were contralateral.61 In that study the majority of recurrences (74%) occurred within 2 years of the initial episode. However, recurrence at much later time intervals has been described and, in the study of Voge et al,60 18% of recurrences occurred between 6 and 9 years after the initial episode. In another study of 319 military personnel,62 the mean time to first recurrence was 39 months with a standard deviation of 39 months, again reflecting the presence of late recurrences. Where procedures are performed to prevent recurrence, there is evidence that open thoracotomy produces the lowest recurrence rates. In a series studied by Abolnik et al62 the recurrence rate for ipsilateral pneumothorax was zero after surgical pleurodesis, 26.5% after chemical pleurodesis, and 38.5% after tube drainage alone. Thoracotomy with pleural abrasion or pleurectomy is generally associated with a failure rate of less than 0.5%.63,64 Pleurectomy provides protection against the risk of recurrent pneumothorax but there are no data concerning any continued risk of pneumomediastinum or gas embolism which might arise from the underlying lung abnormality. Video assisted thoracoscopic surgery (VATS) has been associated with recurrence rates of 5–10%65,66 and is therefore inappropriate as a treatment modality in those wishing to dive after treatment for pneumothorax. Decisions regarding fitness to dive must be taken in the light of these observations.
Lung bullae
Lung bullae may predispose to the development of pneumothorax or may develop tension during ascent. In a case series of three individuals presenting with pneumothorax or tension bullae,67 all three were tourists who had undertaken resort dives without prior chest radiographs. Radiographs taken after the event demonstrated large bullae of varying size in all three subjects. Mellem et al68 also described an episode of cerebral gas embolism in a 23 year old woman in whom retrospective review of pre-dive chest radiographs revealed the presence of a lung bulla. Two further similar cases have been reported in which chest radiographs were normal but CT scans demonstrated bullae.47
Asthma
Asthma is a common cause of concern among those wishing to dive. In a review of referrals to the medical committee of the Scottish Sub Aqua Club for expert advice on fitness to dive, respiratory disorders were responsible for 30% of referrals, the majority being for evaluation of asthma.69 However, the literature concerning asthma and diving is contentious and inconclusive. Theoretically, it might be expected that the diving environment would provoke bronchospasm and that asthma might increase the risk of barotrauma and reduce exercise capability. The latter is a potentially dangerous problem for a diver who may require to swim strongly against currents or to escape danger and thus avoid drowning. In a “state of the art” review in 1979, Strauss suggested that contraindications to diving should include the following: significant obstructive pulmonary disease with minimal values for FEV1, FVC, and maximum voluntary ventilation (MVV) of 75% of predicted; any attack of asthma occurring within 2 years; a requirement for medication; or any episode of bronchospasm associated with exertion or inhalation of cold air.70 Some authors would now regard these guidelines as too restrictive and the issue of asthma risk and diving has been approached from several viewpoints.
Is there epidemiological evidence that asthmatic divers are at excess risk? In 1991 Edmonds reported that, in a series of 100 diving deaths in Australia and New Zealand, nine occurred in asthmatics despite the fact that fewer than 1% of divers reported a history of asthma.71 In contrast, Neuman et al72 found a 5% prevalence of asthma among recreational divers in the USA, similar to that in the general USA adult population, and a fatal accident rate of one asthmatic in 2132 deaths. During the period 1988–94, 369 cases of arterial gas embolism and 2720 cases of decompression illness were reported to Divers Alert Network in the USA; 23 of those reporting arterial gas embolism, and 123 of those reporting decompression illness had coexistent asthma.73 These figures suggest that the prevalence of asthma among those developing arterial gas embolism and decompression illness is similar to that in the general population. There is evidence that some asthmatics can dive without incident. Among 104 responders to a questionnaire for asthmatic divers published in a diving magazine, 96 reported taking a prophylactic β2 agonist before diving and only one reported decompression illness. There were no reported cases of pneumothorax or gas embolism. However, more than half of these subjects were unaware of the contemporary advice for asthmatic divers74 and this was a self-selected sample. In a case control study of 196 episodes of arterial gas embolism, investigators calculated a 1.6 fold increase in risk for subjects with any asthma and a 1.98 fold increase for those with current asthma, but confidence limits were broad and neither figure reached conventional statistical significance.75
It is unclear whether pulmonary function testing can predict risk of diving related illness. In a study of 50 unselected experienced SCUBA divers in Australia, five gave a history of current asthma and one of previous childhood asthma. Ten subjects had an FEV1/FVC ratio 0f <75% and five of these had reduced mid expiratory flow rates. Twenty three of the subjects had a fall in FEV1 of more than 10% from baseline after either histamine or saline inhalation challenge. The authors suggest that, since this group was diving regularly without significant problems, function testing is a poor predictor of diving related illness.76
Is there a role for bronchial provocation testing in predicting risk for asthmatic divers? Among 180 divers with a history of asthma studied by Anderson et al, 90 had normal pulmonary function tests and no bronchial hyperresponsiveness.77 Thirty had a fall in FEV1 of more than 15% after inhaling hypertonic saline indicating bronchial hyperresponsiveness, and the authors would recommend their exclusion from diving. For subjects in whom the post saline fall in FEV1 was 10–14.9%, the authors speculate that diving may be permissible if tests of static lung volumes and expiratory flows at low lung volumes derived from the flow-volume loop are normal. There has been speculation that diving itself might induce bronchial hyperresponsiveness by affecting small airway function. In a cross sectional study of 28 divers and 31 controls, Tetzlaff et al78 reported a higher prevalence of bronchial hyperresponsiveness to histamine among the divers than in non-diving matched controls (12/28 v 5/31). There was a non-significant trend towards an association between the degree of responsiveness and the number of compressed air dives performed. However, there has been no prospective testing of the relationship between bronchial hyperresponsiveness and risk in divers and current evidence does not support routine use of bronchial provocation testing in assessing fitness to dive.
Despite the inconclusive epidemiology and reservations about pulmonary function testing, there is a consensus among diving experts that asthmatics should be advised not to dive if they have wheeze precipitated by exercise, cold, or emotion.3,79 Jenkins et al1 are more conservative, suggesting that any asthma symptoms in the preceding 5 years should prompt advice against diving. However, UK and US authorities recommend that asthmatic individuals who are currently well controlled and have normal pulmonary function tests may dive if they have a negative exercise test. How should the exercise test be performed? Bronchodilators should be withheld for 24 hours before testing. The UK Sports Diving Medical Committee guidelines suggest using a 43 cm step test for 3 minutes or running outside to raise heart rate to 80% of maximum followed by serial peak flow measurements. A fall in peak flow of more than 15% from baseline occurring 3 minutes after exercise is regarded as an exclusion criterion. Since the asthmatic response to exercise is dependent on ventilation rate, temperature, and humidity of inspired air, an ideal protocol would monitor all of these parameters to ensure a reproducible challenge. In practice, a step or free running test and the above heart rate target is more widely applicable and is acceptable. However, a more appropriate schedule to assess the response is to measure FEV1 at 1,3, 5 10, 15 20, and 30 minutes after exercise. A decrease in FEV1 of 10% or more from baseline is abnormal and a decrease of 15% or more is diagnostic of exercise induced bronchoconstriction80 and would contraindicate diving. This protocol has the advantage of detecting subjects with a later nadir in airway function.
Asthmatic subjects who meet the criteria for diving require specific advice on management of their asthma during the diving season. They should monitor their asthma symptoms and twice daily peak flow measurements and should not dive if they have any of the following: active asthma—that is, symptoms requiring relief medication in the 48 hours preceding the dive; reduced PEF (>10% reduction from best values); or increased PEF variability (>20% diurnal variation). There are subjects in whom allergy is the only precipitating factor for wheeze and they may be permitted to dive if they have normal pulmonary function. However, there is a note of caution here. In one unusual case report an asthmatic who was allergic to Pareteria pollen suffered an episode of bronchospasm at depth which proved to be related to contamination of his gas supply and mouthpiece with pollen particles.81
Further discussion of the issues surrounding asthma and diving is available in the proceedings of a conference published in 1996.82
Sarcoidosis
Sarcoidosis is a disease predominantly of young adults and might therefore be expected to be encountered in the population of potential divers. Tetzlaff et al describe a case of barotrauma occurring in a pressure chamber which might be attributed to sarcoidosis.83 Although primarily a respiratory disease, sarcoidosis may also affect the heart, predisposing to arrhythmias which would contraindicate diving.
Other diseases
We did not find specific literature relating to other lung diseases including COPD, lung cancer, and rarer lung conditions. It is likely that, in these conditions, the impairment of lung function or general health would exclude the subject from actively pursuing diving. The presence of any active pulmonary infection would preclude diving until the infection has resolved. In the case of tuberculosis, which is a transmissible disease, diving would be precluded until treatment is complete,84 the subject is asymptomatic and non-infectious, and appropriate investigations confirm that there has been no lasting impairment of lung structure and function.
An algorithm assessing respiratory fitness for diving is shown in fig 1.
SUGGESTED AREAS FOR FUTURE RESEARCH
-
High quality epidemiological information on the incidence of, and factors associated with, dive related illness and injury is required. It is essential that incidence studies incorporate reliable denominator data—that is, number and type of dives performed. Case-control studies may provide useful insights into factors associated with injury.
-
Further information on the predictive value of lung function testing for dive related illness should be based on prospective data collection. The optimal choice of screening test should be determined.
-
The predictive value of thoracic CT scanning versus standard radiography for dive related illness should be investigated.
-
Information on perception of risk among the diving community would inform future provision of advice on dive safety.
APPENDIX 1 SIGN LEVELS OF EVIDENCE AND GRADING OF RECOMMENDATIONS
Levels of evidence
Ia: Evidence obtained from meta-analysis of randomised controlled trial.
Ib: Evidence obtained from at least one randomised controlled trial.
IIa: Evidence obtained from at least one well designed controlled study without randomisation.
IIb: Evidence obtained from at least one other type of well designed experimental study.
III: Evidence obtained from well designed non-experimental descriptive studies such as comparative studies, correlation studies, and case-control studies.
IV: Evidence obtained from expert committee reports or opinions and/or clinical experience of respected authorities.
Grading of recommendations
A (Levels Ia, Ib) At least one randomised controlled trial as part of body of literature of overall good quality and consistency addressing the specific recommendation.
B (Levels IIa, IIb and III) Requires well conducted clinical studies but no randomised controlled trial on the topic of recommendation.
C (Level IV) Requires evidence from expert committee reports or opinions and/or clinical experience of respected authorities. Indicates absence of directly applicable studies of good quality.
APPENDIX 2 LIST OF EXTERNAL REVIEWERS
We are grateful to the following who reviewed earlier drafts of the manuscript. Responsibility for the content of the final document rests entirely with the authors.
Reviewers included: Surgeon Commander Peter Benton, Institute of Naval Medicine ; Dr Phil Bryson, Diving Diseases Research Centre; Dr Sandra Domizio, UK Sport Diving Medical Committee; Dr James Francis; Dr Stephen Glen, UK Sport Diving Medical Committee; Dr Peter Glanvill; Dr Nerys Williams, Health and Safety Executive; Professor Hans Ornhagen, Swedish Defence Research Institute.
APPENDIX 3 TOPICS FOR AUDIT
Auditing the success and relevance of this guideline will require feedback from users. Dr Stephen Watt, a member of the subcommittee and Senior Lecturer in Environmental and Occupational Medicine at the University of Aberdeen, has devised a reporting form (fig 2) which could be used to monitor the value of the guideline.
It is suggested that users could complete this form when carrying out an evaluation. The document would be copied to their own records, to the subject and, if agreement was obtained from the subject, to Dr Watt as a representative of the BTS committee. In the event of a future diving adverse incident, supplementary information could be fed back using the second portion of the form, either by the attending physician or by the subject. A copy of the form is shown on page 00.
Completed forms should be returned to: Dr Stephen Watt, Consultant Physician/Senior Lecturer, Department of Environmental and Occupational Medicine, Liberty Safe Work Research Centre, Foresterhill Road, Aberdeen AB25 2ZP, UK.
REFERENCES
-
- 1.↵
- 2.
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.
- 51.
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵