Article Text

Abstract
Hypoventilation secondary to brainstem stroke resulting in chronic respiratory failure is extremely uncommon. This case documents the treatment of chronic type II respiratory failure secondary to central hypoventilation with medroxyprogesterone, a new treatment option.
- chronic respiratory failure
- brainstem stroke
- medroxyprogesterone
Statistics from Altmetric.com
CASE REPORT
A 59 year old man presented with acute onset of nausea, unsteady gait, and dysphagia. There was a history of systemic hypertension which was treated with bendrofluazide 2.5 mg daily. He smoked 40 cigarettes daily. There was no previous respiratory history and exercise tolerance had been unlimited. Examination revealed nystagmus on horizontal gaze to the right, impaired right sided palatal movement, and an absent gag reflex. Full blood picture, erythrocyte sedimentation rate, antinuclear antibody, ANCA, and thrombophilia screen were all negative or normal. Magnetic resonance imaging showed infarction in the medulla and cerebellum, confirming the clinical diagnosis of a right sided pontomedullary stroke. Several hours later he suddenly lost consciousness and became apnoeic. He was ventilated and transferred to the intensive therapy unit. A CT scan did not show evidence of haemorrhage or raised intracranial pressure. When weaned from invasive ventilation 10 days later, he had persistent but stable type II respiratory failure. On transfer to our unit, speech was incoherent and swallowing was delayed with impaired palatal movement and pharyngeal clearance. Cognitive impairment limited rehabilitation. Type II respiratory failure persisted with arterial carbon dioxide tension (Paco2) >9.8 kPa and arterial oxygen tension (Pao2) <8.3 kPa despite supplemental oxygen (fig 1). Five acute episodes of respiratory decompensation associated with bronchopneumonia occurred over the following 9 weeks. During these episodes pH was 7.12–7.20, Paco2 10–14 kPa, and Pao2 <7 kPa. Initial treatment was with invasive ventilation, but subsequently he was managed with brief periods of non-invasive ventilation (NIV). The use of continuous NIV was not possible because of non-compliance related to cognitive dysfunction. Feeding via a gastrostomy tube was commenced because of inadequate calorific intake and concerns relating to aspiration.

{kind=link}
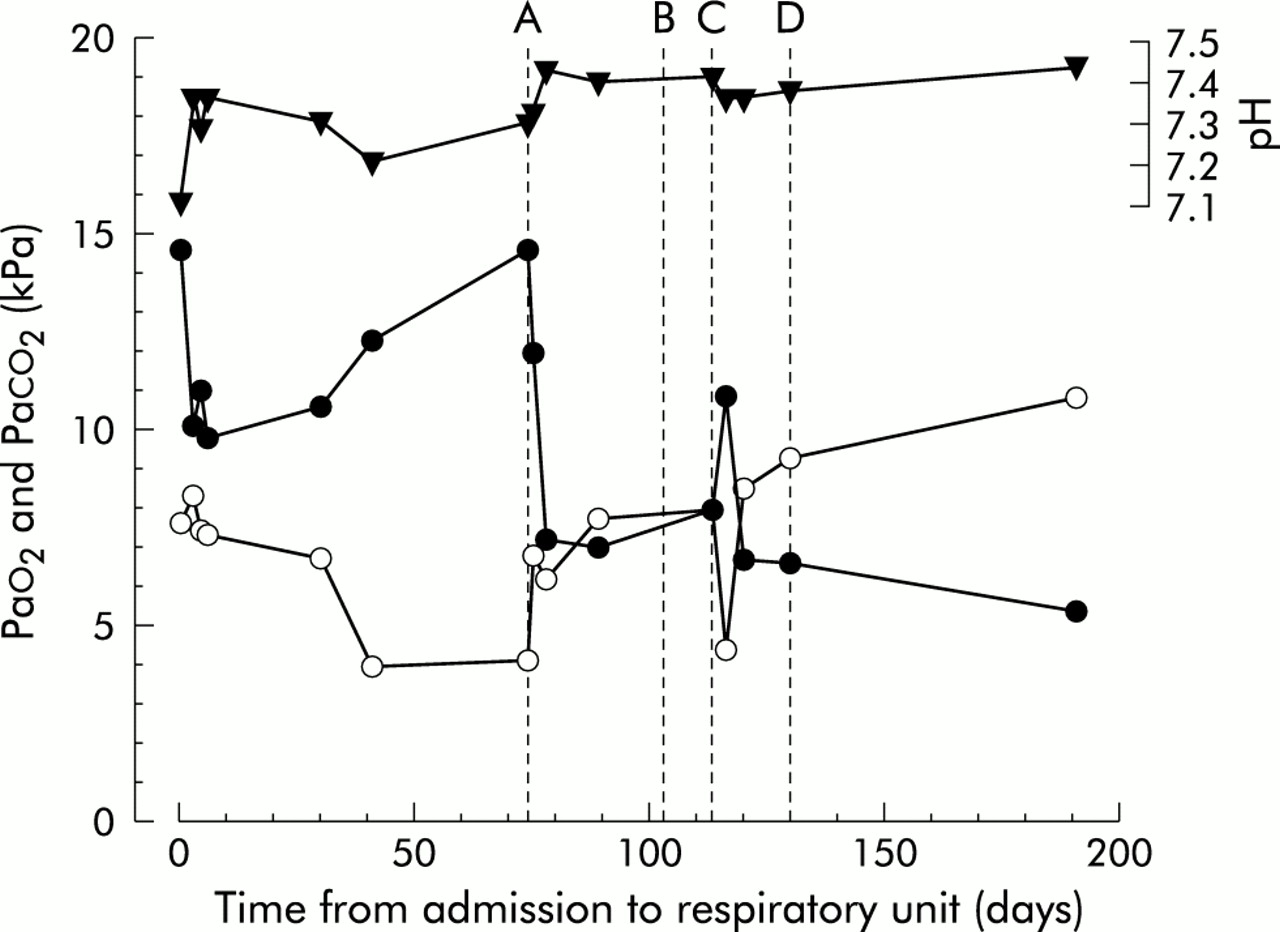
Arterial blood gas analyses from time of initial admission to respiratory unit. Time in days is shown on the x axis. Line A = introduction of medroxyprogesterone (MP); line B = initial discharge from hospital; line C = readmission and commencement of non-invasive ventilation (NIV); line D = final discharge. Values from line A onwards were taken on room air; values before this date were on varying concentrations of oxygen. . , pH; +, Paco2; C, Pao2.
Oral medroxyprogesterone (20 mg tds) was commenced 9 weeks after his initial respiratory arrest. Serial blood gases before and after commencement of medroxyprogesterone are shown in fig 1. Within 1 week the Paco2 had fallen to <7 kPa, higher mental function returned to normal, speech and swallowing improved, and the gastrostomy tube was removed. Spirometric values, previously unobtainable, were normal. He was discharged home without any functional impairment. Two weeks later he presented with acute type II respiratory failure following non-compliance with medroxyprogesterone. Medroxyprogesterone was recommenced and NIV instituted and continued on discharge. At follow up 3 months later he remains well without further hospital admissions.
DISCUSSION
The respiratory centre is located in the pons and medulla. Brainstem disease is a common cause of respiratory failure in an acute setting. However, hypoventilation secondary to brainstem stroke resulting in chronic respiratory failure is extremely uncommon. To our knowledge this is the first report documenting the treatment of chronic type II respiratory failure secondary to central hypoventilation with medroxyprogesterone. Progesterone is probably responsible for the hyperventilation observed in pregnancy as early as the first trimester and the increase in ventilation during the luteal phase of the normal menstrual cycle.1 Medroxyprogesterone, an analogue of progesterone, is used primarily as a depot contraceptive but has been recognised as a respiratory stimulant for some time. It has been shown to benefit patients with respiratory failure resulting from obstructive sleep apnoea,2 chronic obstructive pulmonary disease (COPD),3 and in obesity-hypoventilation syndrome (Pickwickian syndrome).4
The mechanism of action of medroxyprogesterone is unclear. It is suggested that it acts as a respiratory stimulant by increasing central responsiveness to CO2 or hypoxia with inhibition of the hypoventilatory portion of the apnoea cycle. In addition, in obstructive sleep apnoea it has been proposed that, with increased neurogenic drive to the pharyngeal muscles, pharyngeal patency is improved.5
The clinical improvement observed in our patient after medroxyprogesterone was rapid and dramatic. The improvement was not confined to ventilatory capacity, however, with speech, swallowing, and higher mental function all returning to normal. Medroxyprogesterone may have had a direct stimulatory effect on the respiratory centre and the resulting improvement in arterial blood gas tensions may, in turn, have improved brainstem and cerebral function. Alternatively, a direct effect on brainstem function may have occurred which may have improved ventilation and pharyngeal muscle tone independently. The latter is thought to be a mechanism of action in obstructive sleep apnoea and in our patient may have accounted for the improvement in speech and swallowing.