Article Text

Abstract
Background: The accurate diagnosis of latent tuberculosis infection (LTBI) is an important component of any tuberculosis control programme and depends largely on tuberculin skin testing. The appropriate interpretation of skin test results requires knowledge of the possible confounding factors such as previous BCG vaccination. Uncertainty about the effect of BCG vaccination on tuberculin skin testing and the strength with which recommendations are made to individual patients regarding treatment of LTBI have identified a need to analyse the available data on the effect of BCG on skin testing. A meta-analysis of the evidence for the effect of BCG vaccination on tuberculin skin testing in subjects without active tuberculosis was therefore performed.
Methods: Medline was searched for English language articles published from 1966 to 1999 using the key words “BCG vaccine”, “tuberculin test/PPD”, and “skin testing”. Bibliographies of relevant articles were reviewed for additional studies that may have been missed in the Medline search. Articles were considered for inclusion in the meta-analysis if they had recorded tuberculin skin test results in subjects who had received BCG vaccination more than 5 years previously and had a concurrent control group. Only prospective studies were considered. The geographical location, number of participants, type of BCG vaccine used, type of tuberculin skin test performed, and the results of the tuberculin skin test were extracted.
Results: The abstracts and titles of 980 articles were identified, 370 full text articles were reviewed, and 26 articles were included in the final analysis. Patients who had received BCG vaccination were more likely to have a positive skin test (5 TU PPD: relative risk (RR) 2.12 (95% confidence interval (CI)1.50 to 3.00); 2 TU RT23: 26.50 (95% CI 1.83 to 3.85). The effect of BCG vaccination on PPD skin test results was less after 15 years. Positive skin tests with indurations of >15 mm are more likely to be the result of tuberculous infection than of BCG vaccination.
Conclusions: In subjects without active tuberculosis, immunisation with BCG significantly increases the likelihood of a positive tuberculin skin test. The interpretation of the skin test therefore needs to be made in the individual clinical context and with evaluation of other risk factors for infection. The size of the induration should also be considered when making recommendations for treatment of latent infection.
- tuberculosis
- skin testing
- BCG vaccination
Statistics from Altmetric.com
Tuberculosis (TB) is a significant global public health challenge.1 The accurate diagnosis of latent tuberculosis infection (LTBI) is an important component of any TB control programme and depends largely on skin testing. The appropriate interpretation of skin test results requires knowledge of the possible confounding factors such as previous Bacille Calmette Guérin (BCG) vaccination. Many countries have discontinued the use of BCG vaccination, although it is still offered in high prevalence populations and in high risk groups such as newborn Canadian Aboriginal subjects living on reserve.2 Many foreign born subjects have been vaccinated at birth or at school and therefore, even in countries with no BCG vaccination programmes but a large population of foreign born individuals, interpretation of a tuberculin skin test (TST) in the context of a BCG history is important. This is especially true of immigrants who come from high prevalence countries where BCG vaccination is routinely offered. The proportion of individuals with a prior BCG vaccination who have a positive TST result has been reported to vary from 0%3 to 90%.4 Subsequent reactivity can vary depending on dose,5 manufacturer of the vaccine,4 age when vaccinated,3,6,7 and the interval between vaccination and testing.3,6–8
BCG vaccination provides a variable protective effect against TB. A meta-analysis suggested that it gives approximately 60% protection against the development of pulmonary TB with greater protection against tuberculous meningitis and disseminated TB.9 However, prior administration of the BCG vaccine has the potential to interfere with surveillance efforts, particularly when investigating contacts of an active case of pulmonary TB. The uncertainty of the effect of BCG vaccination on TST results and interpretation affects the likelihood of treatment being offered, which is known to be effective.10 In countries with a low prevalence of TB such as Canada and the USA, treatment of LTBI has a potentially greater role than in countries with a higher prevalence where resources are concentrated on case finding and treatment of active cases.11 The recent report by the Institute of Medicine on the control of TB in the US recommends that immigrants to the US should have a TST and those with a positive response should report for treatment of LTBI before receiving their green card.12 The effect of BCG vaccination and tuberculin testing will have a significant impact on the implementation of this recommendation. A recent study in British Columbia compared 837 patients with no prior BCG vaccination and 444 who had been vaccinated with BCG; 43% of vaccinated patients were offered treatment for LTBI following a cluster outbreak of TB compared with 17% of non-vaccinated individuals.10 Several reports from Quebec suggest that BCG vaccination in infancy does not contribute to a subsequent positive PPD response, whereas BCG given in childhood or at an older age may result in a positive TST.11
Uncertainty as to the effect of BCG vaccination on the TST and the strength with which recommendations are made to individual patients regarding treatment of LTBI have identified a need to analyse the available data on the impact of BCG vaccination on skin testing. We have therefore carried out a structured review of the medical literature and a meta-analysis of the impact of BCG on skin test results. Meta-analysis has been recognised as a useful approach for analysing data and it provides more power to detect true differences, especially when studies are small and inconclusive.13
METHODS
A Medline search was conducted for articles published between 1966 and 1999 which measured TSTs in subjects with and without BCG vaccination using the following search terms: “BCG vaccine”, “tuberculin test/PPD”, and “skin test”. Relevant articles were identified from the title or abstract (when available) for further review. Bibliographies of the articles retrieved for review were also evaluated for other relevant references. Prospective studies that compared TST results in patients with and without BCG vaccination and those where the BCG vaccine had been given at least 5 years before inclusion in the skin test surveys were selected. The studies also needed to include a measurement of the TST result presented in a way that allowed calculation of the proportions with a positive test (> 10 mm induration) or the actual measurements. All the control groups were concurrent controls. Studies that included known contacts of active cases were excluded.
Descriptive data recorded included study location, population studied, BCG type, and dose. When available, the time between BCG vaccination and the study was recorded and studies were grouped accordingly. Data on numbers in each study with and without BCG vaccine and numbers with a positive TST (defined as > 10 mm) in each group were analysed.
The overall relative risk (RR) of a positive response for 5 TU and 2 TU was estimated using meta-analytical methods. The logarithmic transforms of the RRs were calculated for each study and combined using inverse variance estimates as weights.14,15 Relative risks were used in preference to odds ratios as the response rates were too high for odds ratios to provide close approximations to relative risks. Chi square tests of homogeneity were performed and, as the hypotheses of homogeneity were rejected, random effects models were used to derive the final estimates across the studies.14,15
Analogous methods were applied to the estimation of the relative risks at cut off points of > 5 mm and > 15 mm wheal diameters, respectively. Response rates at specific diameters were compared between subjects who had and had not received BCG vaccination. Since the estimated proportions were low, rate differences rather than RRs were used in these comparisons and high precision estimates of the corresponding variances were employed.16 Rate differences were again combined using random effects models with inverse variance estimates as the weights.
We used several a priori hypotheses to address differences between studies in an attempt to explain heterogeneity. Studies using different types of tuberculin (5 TU PPD and RT23) were analysed separately. The age at which BCG was administered may affect the TST measurement, as can vaccinations. Studies using two step testing were compared with studies using a single TST. As geographical location may affect the efficacy of BCG vaccination,17 studies were grouped according to latitude.
The articles were independently reviewed by two investigators (MOT, RKE) to decide on eligibility for inclusion in the meta-analysis. The reviewed articles were not blinded to author or setting of each study.
RESULTS
A total of 980 potential articles were identified from the Medline search and bibliography review, 370 of which were retrieved. Fifty six studies met the inclusion criteria. Studies were excluded if they were found to be not prospective or if they did not have concurrent controls. There was combined agreement between the two reviewers to include 24 studies. A further two were included after consensus review, giving a total of 26 studies in the meta-analysis.18–43 The demographic characteristics of the selected studies are summarised in table l.
Demographic characteristics of studies included in the meta-analysis
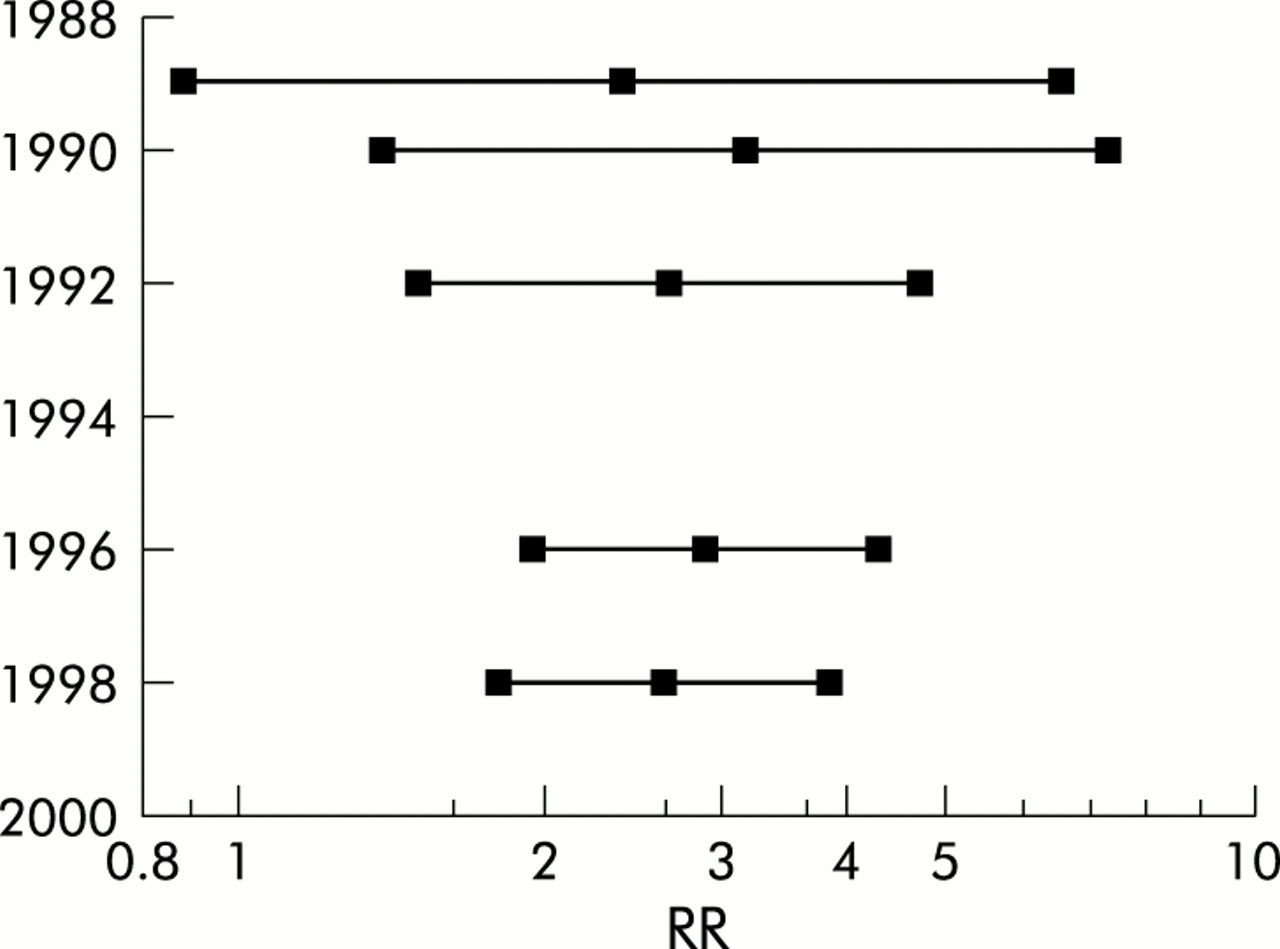
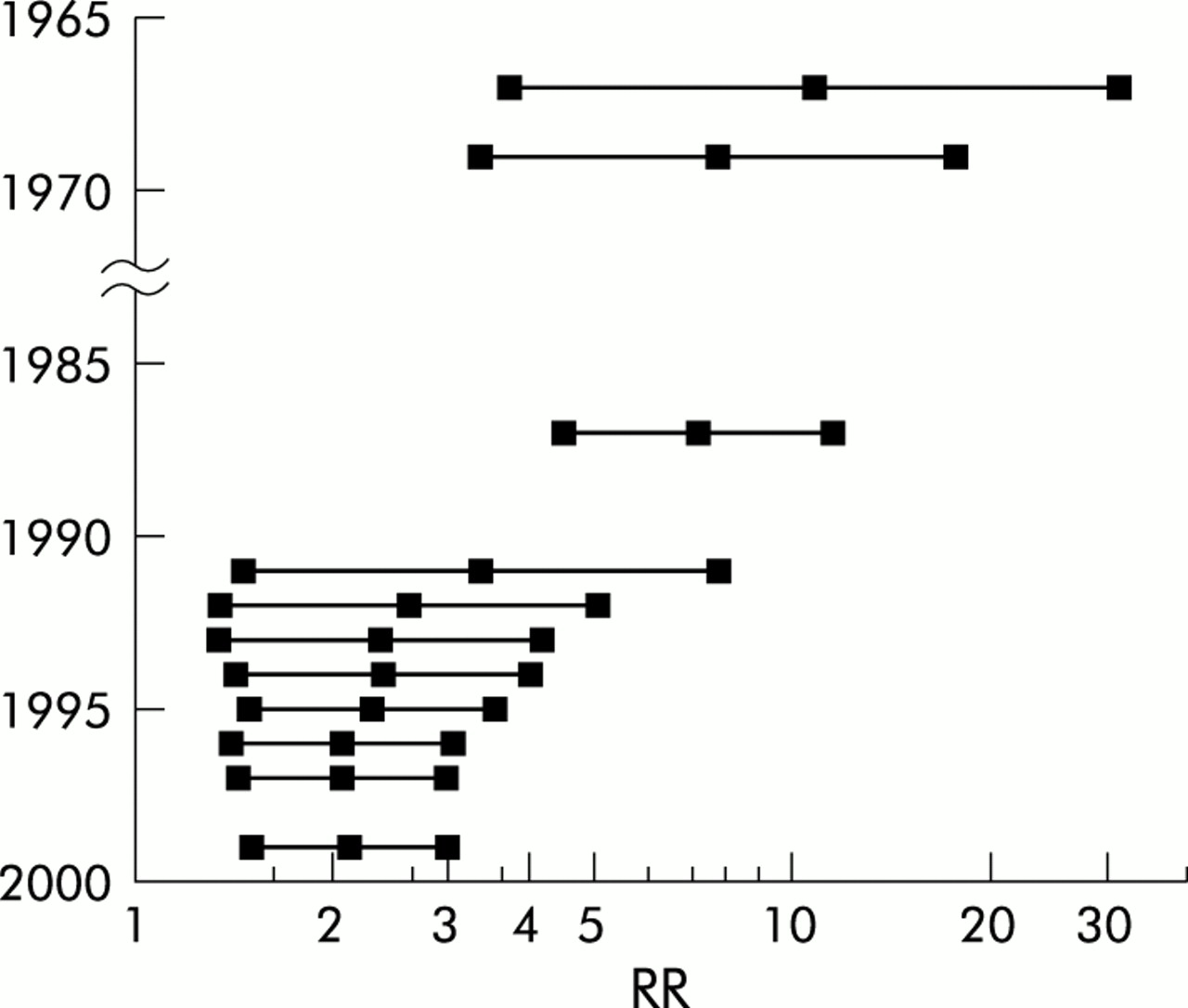
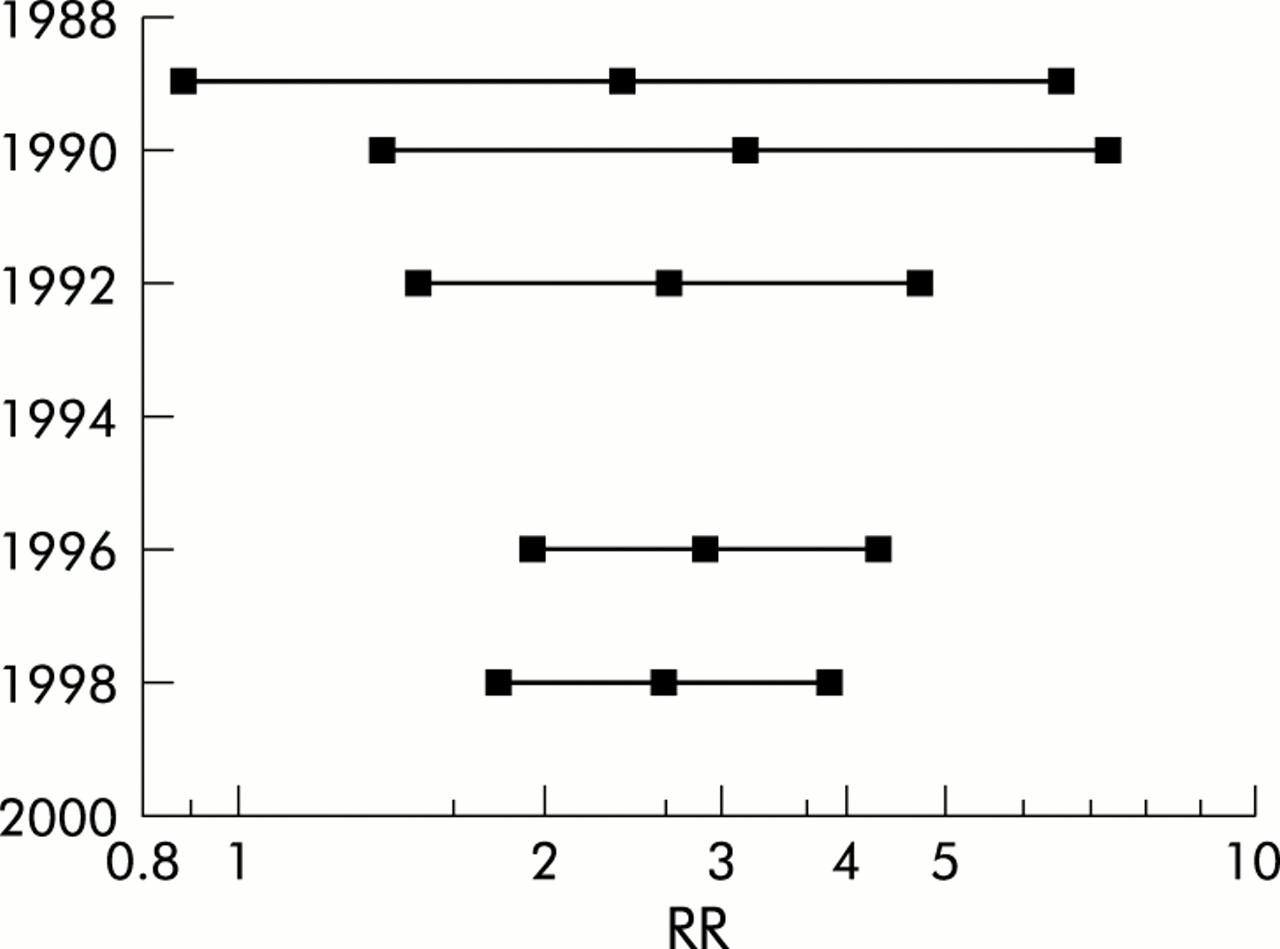
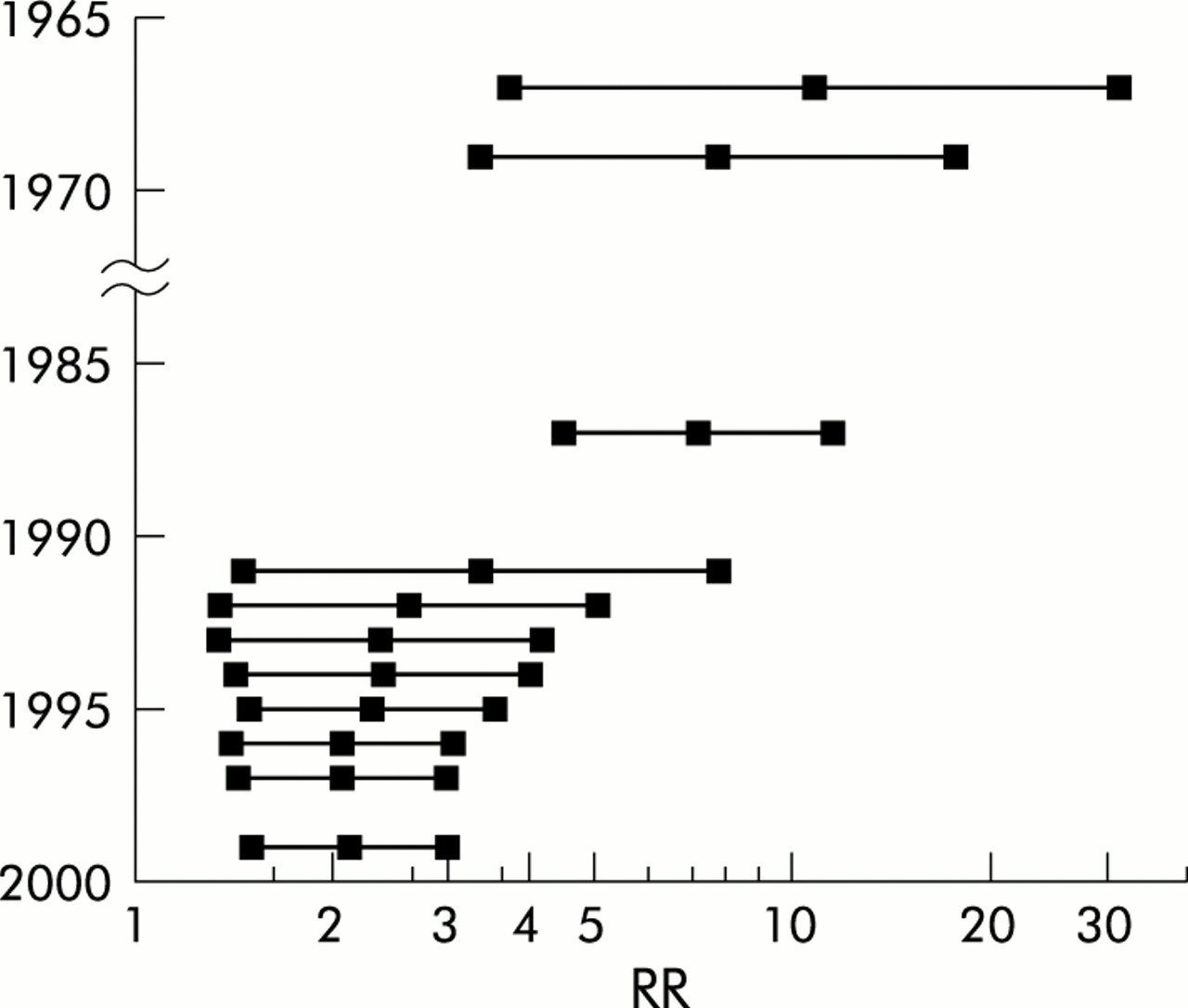
The meta-analysis showed that subjects who had received BCG vaccination were more likely to have a positive skin test reaction to both 5 TU PPD and RT23. The RR for 5 TU PPD, 2 TU RT23, and 1 TU RT23 was 2.12 (95% CI 1.50 to 3.00), 2.65 (95% CI 1.83 to 3.85), and 2.85 (95% CI 2.05 to 3.95), respectively (table 2). Table 3 shows the RR when cut off points of > 5 mm and > 15 mm induration were used. Figures 1 and 2 show the cumulative RR of a positive TB skin test using 5 TU PPD and RT23, respectively.
Positive skin test results with different antigens using > 10 mm as cut off point
Positive skin tests using different antigens and a cut off point of > 5 mm or > 15 mm
Cumulative RR for a positive PPD skin test using > 10 mm induration and 5 TU RT23.
Cumulative RR for a positive response with 5 TU PPD using > 10 mm as a cut off point.
Temporal association of BCG vaccination
The timing of the BCG vaccination was also important. Immunisation given after infancy was almost twice as likely to result in a positive skin test as vaccination at birth when using 5 TU PPD. When 2 TU RT23 was used as the antigen, BCG vaccination was significantly associated with a positive reaction even when given at infancy. There was a higher RR of a positive skin test when 5 TU PPD was administered within 15 years of the BCG vaccination. In those tested more than 15 years after vaccination there was a significant but attenuated effect. Subjects immunised after infancy and tested less than 15 years later had a high RR of a positive skin test but, even when given after infancy, skin testing more than 15 years after vaccination did not result in a significant reaction (table 4).
Skin test results at different times of BCG immunisation and varying times between tuberculin skin testing and immunisation for different antigens
Booster effect and geographical location
Four studies addressed the boosting phenomenon with two step testing being performed. Those with a prior history of BCG were more likely to boost their reaction, adding 17.4% to the positive group, but 10% were also added to the group without BCG vaccination (table 5).
Skin test results in two step tuberculin testing by different antigens
The effect of geographical location was evaluated by grouping studies according to latitude (5 TU PPD only). No difference in RR of a positive test based on geographical location was observed (table 6).
Geographical location and skin test results with 5 TU PPD
Size of tuberculin skin test and BCG status
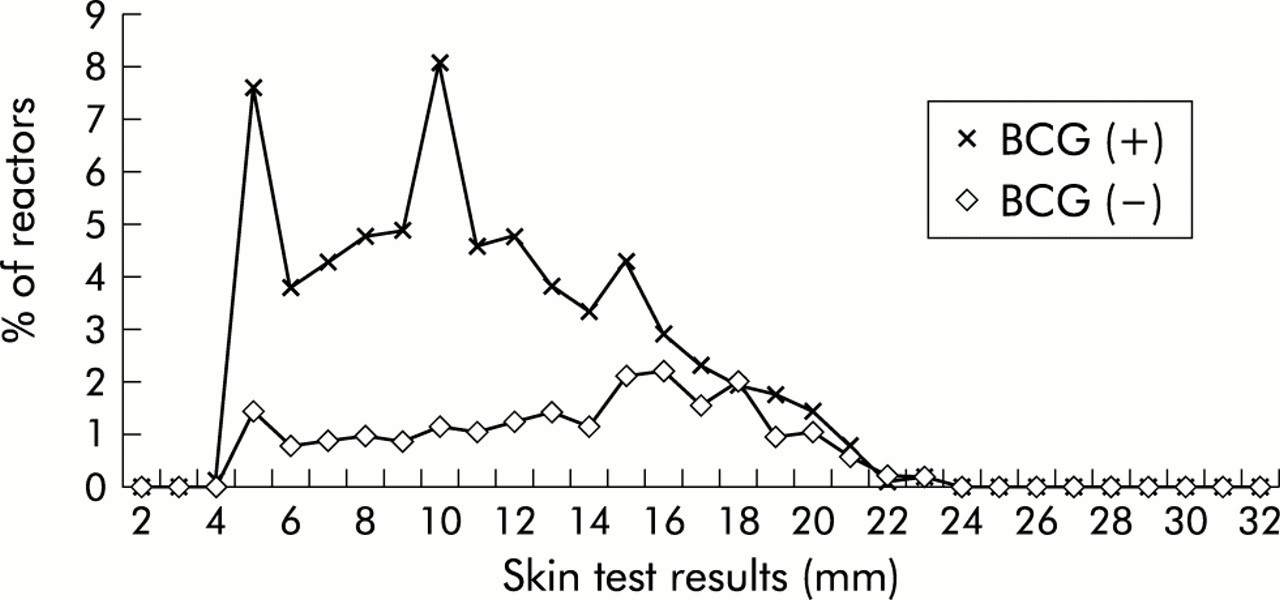
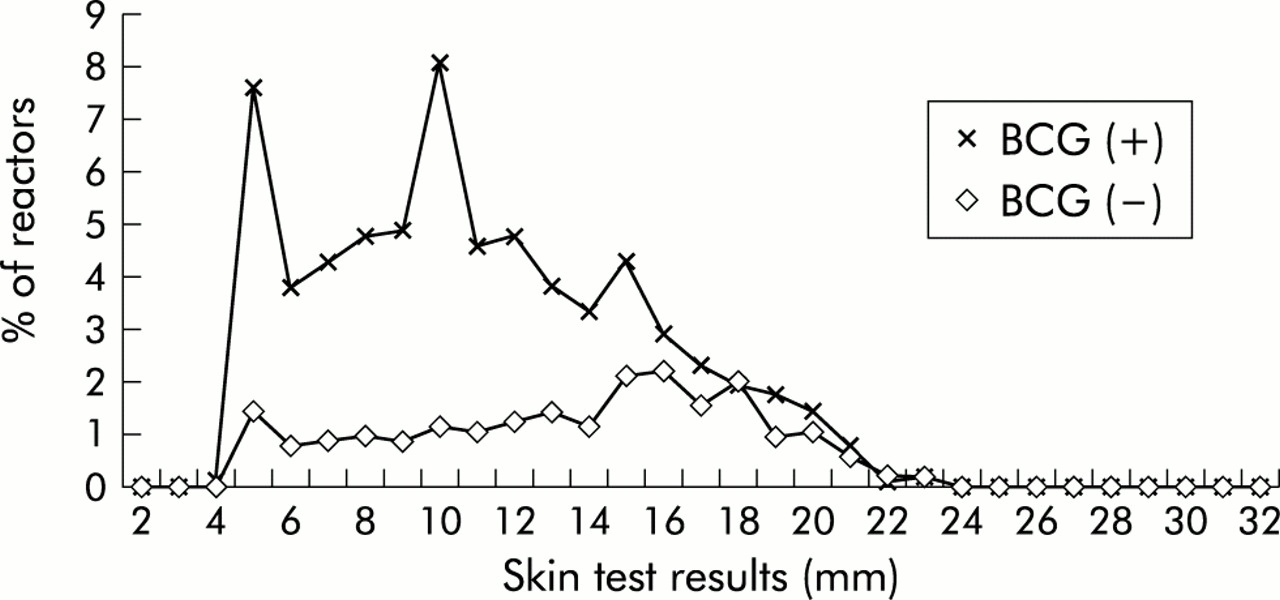
Four studies had discrete data for each measurement of the TST response (figs 3 and 4). There was no difference between the proportions of BCG positive and negative subjects at 14 mm with 5 TU PPD (p=0.31) or at 16 mm with RT23 (p=0.17).
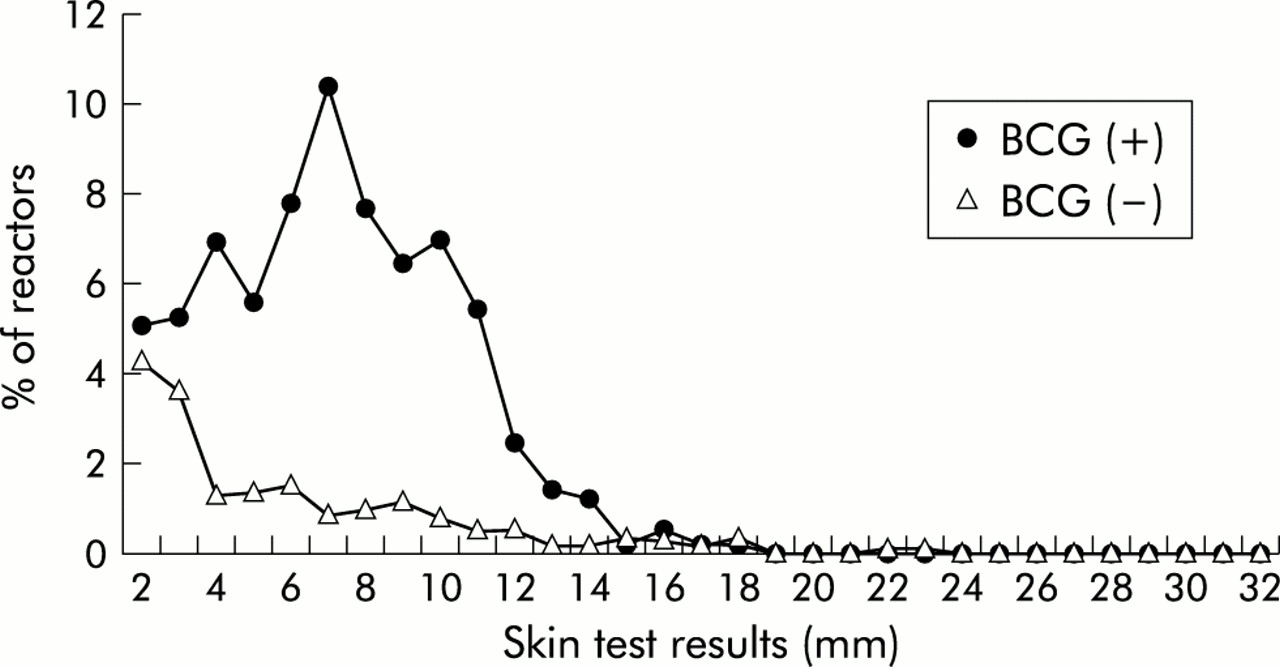
Percentage reactors versus skin test results in mm with 5 TU PPD (576 BCG+, 1145 BCG–).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage reactors versus skin test results in mm with 2 TU RT23 (2880 BCG+, 1425 BCG–).
DISCUSSION
This meta-analysis has extended our understanding of the effect of BCG on the likelihood of having a positive PPD skin test in patients without a known TB contact. An argument frequently used against the use of BCG vaccination in TB control programmes (apart from questions of efficacy) is the subsequent effect on the TST as it might interfere with the identification of infected individuals, especially contacts of active cases of TB.9 This is not a problem for most people born in North America because BCG vaccination is not commonly administered. However, the proportion of TB cases occurring among foreign born individuals is increasing both in Canada46 and the US.47 Many of the contacts of these active cases will also be foreign born and are likely to have been vaccinated with BCG. Our results should therefore simplify interpretation of a positive TST in foreign born individuals and facilitate recommendations for the treatment of LTBI. This clarification is particularly important as the recent Institute of Medicine report has recommended that immigrants to the US should have a TB skin test performed in their country of origin. If positive, they would need to complete a course of treatment for LTBI before obtaining their final immigration status.12 Our data suggest that, if the BCG vaccination was given more than 15 years previously, it should be ignored as a cause of a current positive TST result, especially if the induration is > 15 mm. In addition, our data show that use of RT23, a common tuberculin used outside North America, is much more likely to be associated with a positive TST response than PPD.
Menzies et al have previously shown in patients studied in Quebec that BCG vaccination given in infancy was unlikely to cause a subsequent positive TST result.20 Our data refine their conclusions by demonstrating a temporal effect between BCG vaccination and TST. The RR of a positive TST result was 3.56 (95% CI 3.05 to 4.15) when the skin test was performed within 15 years of BCG vaccination but only 1.46 (95% CI 1.40 to 1.53) after 15 years. When BCG vaccination was given after infancy,21 the result of a TST performed within 15 years was strongly associated with a positive test (RR 9.99, 95% CI 5.29 to 18.89). In the two studies in which the TST was performed more than 15 years after BCG vaccination given after infancy there was no association with a positive TST (RR 0.80, 95% CI 0.74 to 0.85).22,23
The type of tuberculin used for testing had a significant effect on heterogeneity. The extent of the differences in the magnitude of effect was unexpected. Non-vaccinated patients were three times as likely to have a positive TST when tested with RT23 2 TU (RR 3.02) and RT23 1 TU (RR 2.85) than with 5 TU PPD. Subjects who had received BCG vaccination in infancy were even more likely to have a positive test when RT23 was used (RR 3.86 for 2 TU RT23 v 0.96 for 5 TU PPD). Several studies have compared RT23 PPD with 5 TU PPD-S and Tubersol.48,49 Comstock et al49 compared 5 TU PPD-S with doses of RT23 in Inuit children, TB patients, and US navy recruits and found equivalence in the Inuits but more positive reactions with RT23 in the navy recruits. This result was attributed to non-specific sensitivity and raised a caution about interpretations in areas with a decreasing prevalence of TB. A recent Korean study suggested decreased potency of RT23, but this remains controversial.48 There have been some concerns about equivalency in batches of PPD Tubersol and Aplisol.49 The reasons for our observations are unclear, but infection with atypical mycobacteria and geographical latitude may have some impact.19 Other possibilities include the type of vaccine used, a true difference in potency of the tuberculin, or other unknown nutritional or genetic factors.
A positive TST of > 15 mm is less likely to be due to BCG vaccination, regardless of the type of tuberculin used for testing (figs 3 and 4). It seems that a strongly positive reaction (>15 mm) is more likely to be caused by tuberculosis infection than the effect of previous BCG vaccination. These data are particularly important if the timing or status of BCG vaccination is unknown.
The contribution of BCG vaccination to the booster response was only addressed by four studies. BCG vaccinated subjects were more likely to have a positive TST on first testing (28.7% v 22.3% (RR 1.28, 95% CI 1.15 to 1.43)). BCG had a greater effect on boosting with a positive second test in 17.3% compared with 11.8% in a non-vaccinated group (RR 1.47, 95% CI 1.22 to 1.76). These data are consistent with a study from Montreal that associated previous BCG vaccination (p <0.001), interval from BCG vaccination to testing (p<0.01), and older age when vaccinated (p<0.02) with a greater likelihood of having a booster response.35 The impact of BCG vaccination on boosting the TST is particularly relevant in evaluating groups at risk of exposure to TB such as healthcare workers, in which subgroups of foreign born workers are likely to have received one or more BCG vaccinations.10,29
This meta-analysis has several methodological limitations. We limited our search strategy to the English language literature and Medline. We did not hand search any journals and therefore may have missed some published studies. However, the study did include pooled data from 117 507 subjects and therefore the conclusions should be robust. We sought data regarding the type of BCG used from primary authors of the included studies (25 letters, 12 replies) and also group data to interpret graphically presented data, but otherwise made no attempt to identify unpublished data.
In summary, this meta-analysis addresses important clinical and epidemiological questions about interpreting the TST in patients with previous BCG vaccination. The finding of a temporal association between a positive TST result and BCG vaccination should help TB workers and consultants to educate patients and their primary care physicians when offering treatment for LTBI in a setting of previous BCG vaccination, a positive skin test, and no known TB contact. In our experience there is a strong tendency for primary care physicians to attribute any positive skin test in a vaccinated foreign born patient to BCG. Large or strongly positive skin tests are most probably due to tuberculous infection rather than BCG. This observation is supported by a recent study from Botswana in children aged 3–60 months with >90% BCG vaccination rates which found positive TST results to be most strongly associated with close TB contact in mothers and aunts.50 Our results strongly support the recommendations that emphasise the continued value of skin testing BCG vaccinated individuals in the appropriate clinical setting.51,52
Acknowledgments
This study was funded in part by a grant from Medical Services Branch, Health Canada. Dr Lei Wang was funded by the World Bank. The authors thank Drs Sverre Vedal, Ruth Milner and Eduardo Hernandez for statistical advice and Edwin Mak for assistance in data management and programming.
Dr FitzGerald is a recipient of a Vancouver General Hospital Scientist Award and also a Canadian Institute of Health Research/BC Lung Association Investigator Award.
REFERENCES
Linked Articles
- Correction