Article Text

Abstract
Background: Exhaled carbon monoxide has been reported to increase in inflammatory pulmonary diseases and to be correlated with blood carboxyhaemoglobin (Hb-CO) concentration. A study was undertaken to determine whether arterial blood Hb-CO increases in patients with inflammatory pulmonary diseases.
Methods: The Hb-CO concentration in arterial blood was measured with a spectrophotometer in 34 normal control subjects, 24 patients with bronchial asthma, 52 patients with pneumonia, and 21 patients with idiopathic pulmonary fibrosis (IPF).
Results: The mean (SE) Hb-CO concentrations in patients with bronchial asthma during exacerbations (n=24, 1.05 (0.05)%), with pneumonia at the onset of illness (n=52, 1.08 (0.06)%), and with IPF (n=21, 1.03 (0.09)%) were significantly higher than those in control subjects (n=34, 0.60 (0.07)%) (mean difference 0.45% (95% confidence interval (CI) 0.23 to 0.67), p<0.01 in patients with bronchial asthma, mean difference 0.48% (95% CI 0.35 to 0.60), p<0.0001 in patients with pneumonia, and mean difference 0.43% (95% CI 0.26 to 0.61) p<0.001 in patients with IPF). In 20 patients with bronchial asthma the Hb-CO concentration decreased after 3 weeks of treatment with oral glucocorticoids (p<0.001). In 20 patients with pneumonia the Hb-CO concentration had decreased after 3 weeks when patients showed evidence of clinical improvement (p<0.001). The values of C-reactive protein (CRP), an acute phase protein, correlated with Hb-CO concentrations in patients with pneumonia (r=0.74, p<0.0001) and in those with IPF (r=0.46, p<0.01). In patients with bronchial asthma changes in Hb-CO concentrations were significantly correlated with those in forced expiratory volume in 1 second (FEV1) after 3 weeks (r=0.67, p<0.01). Exhaled carbon monoxide (CO) concentrations were correlated with Hb-CO concentrations (n=33, r=0.80, p<0.0001).
Conclusions: Hb-CO concentrations are increased in inflammatory pulmonary diseases including bronchial asthma, pneumonia, and IPF. Measurement of arterial Hb-CO may be a useful means of monitoring pulmonary inflammation.
- carboxyhaemoglobin
- haem oxygenase
- inflammatory pulmonary disease
Statistics from Altmetric.com
Carbon monoxide (CO) is produced endogenously by the class of enzymes known collectively as haem oxygenase (HO).1 HO-1, the inducible form of HO, is induced by various stimuli including proinflammatory cytokines and nitric oxide.1 CO is known to be present in measurable quantities in the exhaled air of normal subjects.2,3 Exhaled CO is increased in patients with inflammatory pulmonary diseases such as bronchial asthma, bronchiectasis, upper respiratory tract infections, and seasonal allergic rhinitis.3–7 Treatment with inhaled and oral corticosteroids, which have been shown to reduce airway inflammation, is associated with a reduction in the exhaled levels of CO in asthma.3,8 Furthermore, exhaled CO is increased in exacerbations of bronchial asthma induced by respiratory virus infections.8 Based on these findings, it has been proposed that measurements of exhaled CO may serve as an indirect marker of airway inflammation.3–8 On the other hand, exhaled CO concentration is reported to correlate closely with blood carboxyhaemoglobin (Hb-CO) concentrations over the range of values encountered in smokers and non-smokers,2 which suggests that the Hb-CO concentration may increase in patients with inflammatory pulmonary diseases. However, the Hb-CO concentration in inflammatory pulmonary diseases has not been studied.
This study was undertaken to determine whether the Hb-CO concentration in arterial blood is increased in patients with inflammatory pulmonary diseases including bronchial asthma, pneumonia, and idiopathic pulmonary fibrosis (IPF).
METHODS
Subjects
Thirty four normal elderly control subjects (mean (SE) age 73.8 (0.7) years), 24 patients with bronchial asthma (75.1 (0.8) years), 52 with pneumonia (73.2 (1.7) years), and 21 with idiopathic pulmonary fibrosis (IPF) (72.1 (2.2) years) were studied. In 34 control subjects there was no history of respiratory or cardiovascular disease. None of the control subjects was receiving long term medication.
Asthma was defined as a clinical history of intermittent wheeze, cough, chest tightness, or dyspnoea and a documented reversible airflow limitation either spontaneously or with treatment during the preceding year.9 All 24 patients with bronchial asthma had a clinical history of these symptoms and reversible airflow limitation. Pneumonia was defined as a pulmonary infiltrate on the chest radiograph, cough, temperature >37.8°C, or subjective dyspnoea. All 52 patients with pneumonia had the features of a pulmonary infiltrate on the chest radiograph, cough, and temperature >37.8°C. Three of the patients had complained of dyspnoea. To define the diagnosis of IPF we obtained a transbronchial lung biopsy specimen from all 21 patients and light microscopic examination of the tissue showed interstitial pulmonary fibrosis with hypertrophy of the alveolar wall and increased fibrous tissue in the alveolar wall.10 Furthermore, no asbestos body, inflammatory granuloma, or lung cancer was found in the lung tissue. Autoimmune antibodies including antibodies to nuclei and DNA were negative. All 21 patients had the features of progressive dyspnoea of unknown origin, bilateral infiltrates on the chest radiograph with honeycombing, and pulmonary function test with reduced total lung capacity and forced vital capacity, and decreased single breath carbon monoxide transfer factor. The diagnosis of IPF was confirmed in all 21 patients.10
Twelve of the 34 control subjects, all the patients with bronchial asthma, 14 of the 52 patients with pneumonia, and six of the 21 patients with IPF were non-smokers, while other control subjects and patients were ex-smokers who had stopped smoking for at least 3 months before this study. To exclude current smokers we measured urinary cotinine concentrations (ng/ml) with high performance liquid chromatography as described previously.11 To adjust for urinary dilution, urinary cotinine concentrations were standardised to urinary creatinine concentration and expressed as cotinine/creatinine ratios.12 These urinary cotinine/creatinine ratios were calculated by dividing the urinary cotinine concentration by the urinary nicotine concentration.12 Because urinary nicotine concentrations were expressed as mg/ml, the cotinine/creatinine ratios were expressed as ng/mg.12 Patients with inflammatory diseases in organs other than the lung were excluded.
Measurement of Hb-CO and exhaled CO
The Hb-CO concentration in arterial blood was measured with a spectrophotometer (ASL System, Radiometer, Copenhagen, Denmark)2,13 and exhaled CO was measured on a portable Bedfont EC50 analyser (Bedfont Technical Instruments Ltd, Sittingbourne, UK) as previously described.2,3,6–8 It has been shown that exhaled CO can be a reflection of passive smoking in children, suggesting the influence of ambient CO on the values of exhaled CO.14 We therefore determined the exhaled CO by subtracting the background levels from the observed reading as described previously.3,6–8 The estimation of Hb-CO from exhaled CO measurements can be inaccurate in patients with severe airflow obstruction,15 so patients in whom the forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio was less than 45% were excluded.15
Study protocol
In all patients with bronchial asthma the Hb-CO concentration was measured on admission to hospital because of exacerbation. The patients who had been treated with inhaled corticosteroid (beclomethasone dipropionate 400–1200 μg/day) and oral bronchodilator (procaterol hydrochloride 50–100 μg/day) were treated with oral glucocorticoids (prednisolone 40 mg/day) for 21 days. To investigate the effect of oral corticosteroids on Hb-CO concentration, 20 patients with bronchial asthma were studied again after 3 weeks of treatment with oral glucocorticoids. Likewise, Hb-CO was measured in all patients with pneumonia before treatment with antibiotics. The patients with pneumonia were treated with antibiotics for 7–14 days and the Hb-CO concentration was then measured again in 20 patients with pneumonia after 3 weeks when the patients showed evidence of clinical improvement. In 21 patients with IPF the Hb-CO concentration was measured at the first admission for investigation and diagnosis. To examine the relationship between Hb-CO and exhaled CO, exhaled CO was measured in 33 subjects including control subjects (n=8) and patients (n=25).
Statistical analysis
Age, Hb-CO concentrations, and CRP values in each group are reported as mean (SE) values. The values of Hb-CO and CRP were compared between each patient group and the control group using the Student's t test. To analyse the differences in Hb-CO and CRP values, the mean difference and 95% confidence intervals were compared between each patient group and the control group. A matched analysis using the paired t test was performed for the comparison of values before and after recovery. The association of CO and CRP levels with Hb-CO, and of changes in the Hb-CO values with those in FEV1 were assessed by correlation analysis. Significance was accepted at p<0.05.
RESULTS
In control subjects the arterial Hb-CO concentrations in ex-smokers (n=12, mean (SE) 0.61 (0.03)%) did not differ from those in non-smokers (n=22, 0.62 (0.02)%) (mean difference –0.01%, 95% CI –0.18 to 0.15, p>0.50). In all the patients and control subjects the urinary cotinine/creatinine ratios were less than 30 ng/mg, the level used to categorise subjects as having been exposed to cigarette smoke,12 showing that the ex-smokers in both control and patient groups were not current smokers. We therefore analysed the data from non-smokers and ex-smokers together in the control and patient groups.
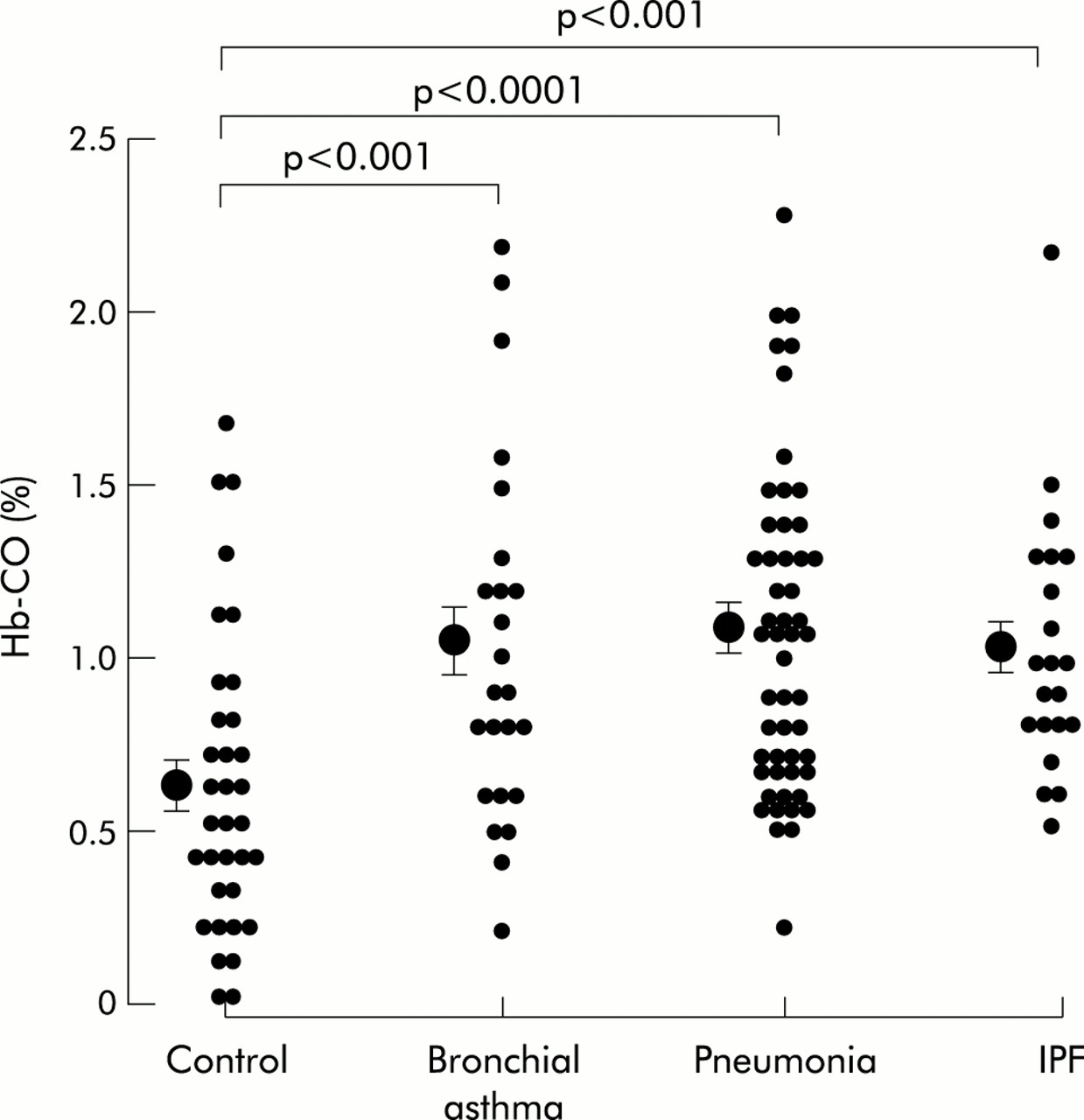
Hb-CO concentrations in the patients with bronchial asthma during exacerbations, in patients with pneumonia at the onset of illness, and in patients with IPF were significantly higher than those of control subjects (fig 1). In subjects aged less than 50 years the Hb-CO levels in patients with bronchial asthma (n=3, 1.13 (0.14)%), in those with pneumonia (n=4, 1.05 (0.01)%), and in those with IPF (n=3, 0.93 (0.03)%) were also significantly higher than those in control subjects (n=4, 0.65 (0.03)%) (mean difference 0.48% (95% CI 0.31 to 0.65), p<0.05 in patients with bronchial asthma, mean difference 0.40% (95% CI 0.38 to 0.42), p<0.01 in patients with pneumonia, and mean difference 0.28% (95% CI 0.24 to 0.32), p<0.01 in patients with IPF).

Arterial blood carboxyhaemoglobin (Hb-CO) concentrations in control subjects (n=34) and in patients with bronchial asthma (n=24), pneumonia (n=52), and idiopathic pulmonary fibrosis (IPF) (n=21). Mean (SE) values are indicated by closed circles with error bars.
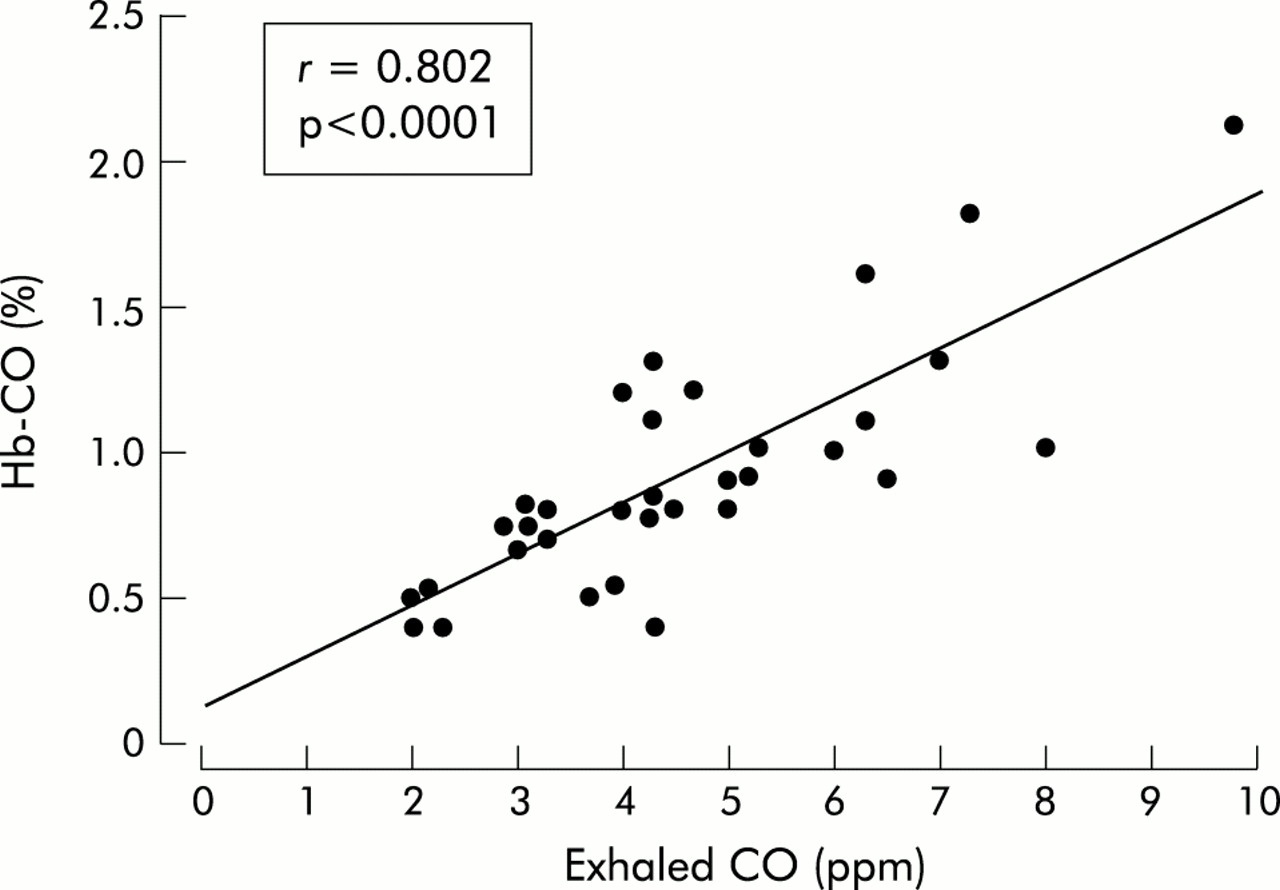
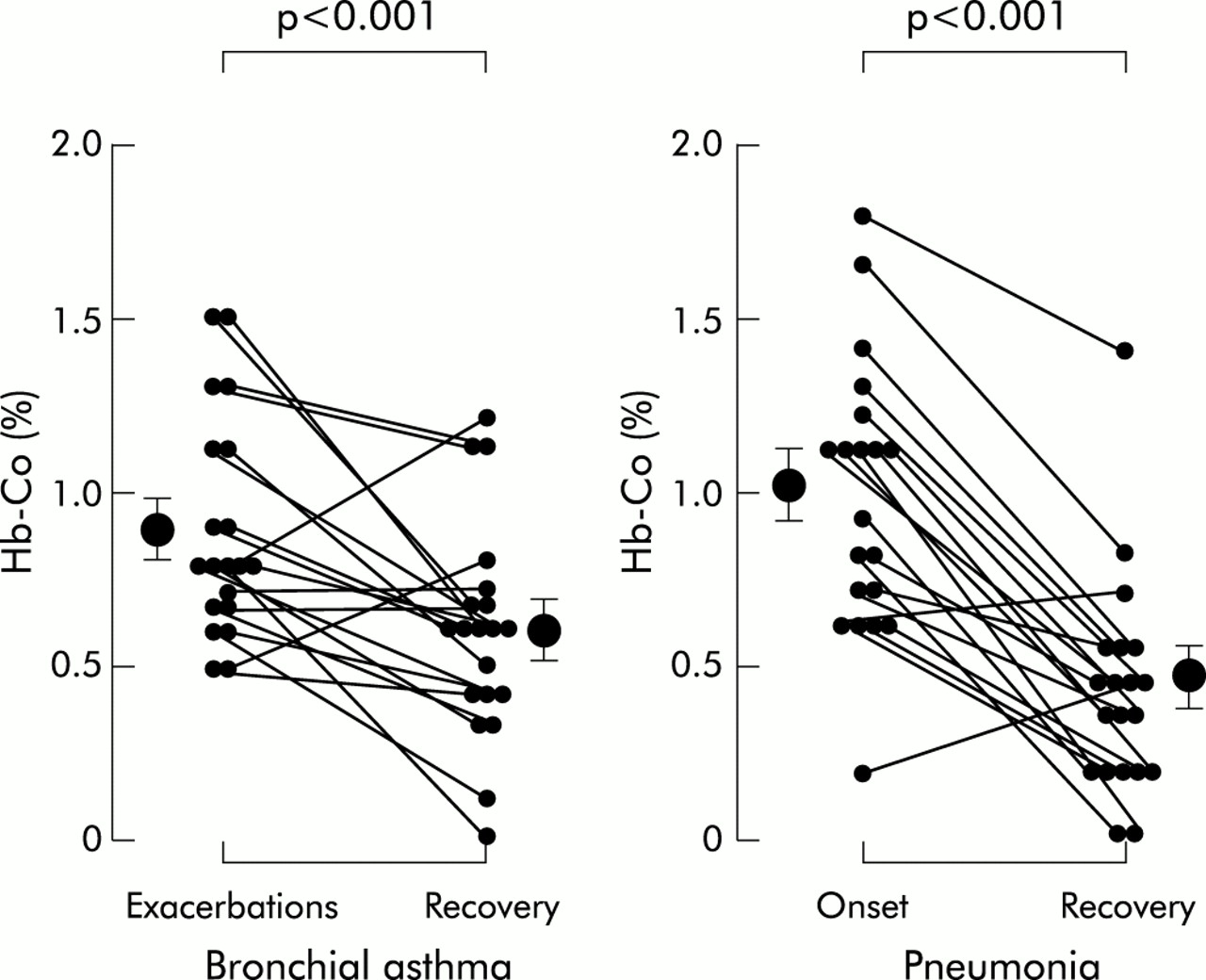
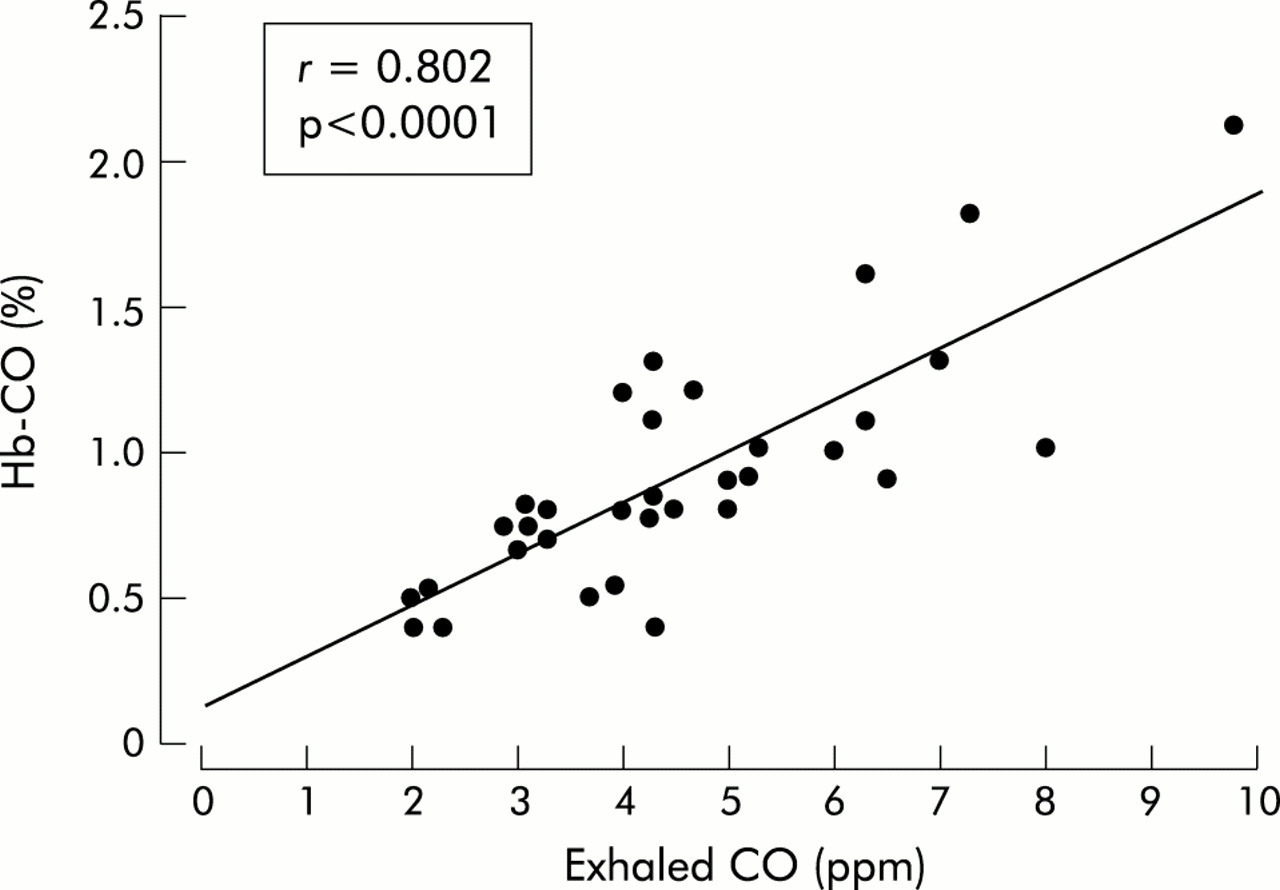
In 20 patients with bronchial asthma the increase in Hb-CO seen during the exacerbation decreased after 3 weeks of treatment with glucocorticoids (fig 2). Likewise, in 20 patients with pneumonia the Hb-CO decreased after 3 weeks when patients showed evidence of clinical improvement (fig 2). Exhaled CO values measured in 33 subjects including control subjects (n=8), patients with bronchial asthma (n=10), patients with pneumonia (n=12), and patients with IPF (n=3) significantly correlated with the concentrations of arterial Hb-CO (fig 3). The concentrations of CRP in patients with bronchial asthma (n=24, 0.96 (0.20) mg/dl), in patients with pneumonia (n=52, 7.57 (0.87) mg/dl), and in patients with IPF (n=21, 0.82 (0.07) mg/dl) were also significantly higher than those in control subjects (n=34, 0.28 (0.12) mg/dl) (mean difference 0.68 mg/dl (95% CI 0.26 to 1.10), p<0.05 in patients with bronchial asthma, mean difference 7.29 mg/dl (95% CI 5.53 to 9.05), p<0.01 in patients with pneumonia, and mean difference 0.54 mg/dl (95% CI 0.26 to 0.82), p<0.01 in patients with IPF). CRP values correlated with Hb-CO concentrations in patients with pneumonia (r=0.74, p<0.0001) and in those with IPF (r=0.46, p<0.01). In contrast, CRP values did not correlate with Hb-CO concentrations in patients with bronchial asthma (r=0.19, p=0.39). On the other hand, in patients with bronchial asthma changes in the Hb-CO concentrations were significantly correlated with those in FEV1 (r=0.67, p<0.01) after 3 weeks of treatment with glucocorticoids.

Arterial Hb-CO concentrations in symptomatic asthma before (Exacerbations) and after (Recovery) treatment with oral corticosteroids (left side) and in patients with pneumonia on admission (Onset) and after recovery (Recovery) (right side). Mean (SE) values are indicated by closed circles with error bars.
{kind=link}
{kind=link}
{kind=link}
Relationship between arterial carboxyhaemoglobin (Hb-CO) concentrations and exhaled carbon monoxide (CO) concentrations in 33 subjects including control subjects (n=8), patients with bronchial asthma (n=10), patients with pneumonia (n=12), and patients with IPF (n=3).
Gallium-67 citrate scintigraphy, a method of evaluating alveolitis,16 showed a positive uptake in all patients with IPF. Furthermore, the level of KL-6 antigen—a useful indicator of disease activity in patients with IPF17,18—in peripheral venous blood of patients with IPF was higher than the upper limit of the normal range (520 U/ml) reported previously by Kohno et al.17
DISCUSSION
We have shown increases in blood Hb-CO concentrations in the arterial blood of patients with bronchial asthma, pneumonia, and IPF. The levels of CRP in patients with bronchial asthma, pneumonia, and IPF were significantly higher than those in control subjects. The CRP levels were significantly correlated with the Hb-CO concentrations in patients with pneumonia and in those with IPF, but not in patients with bronchial asthma. The Hb-CO concentrations fell after treatment with oral corticosteroids and antibiotics in the patients with bronchial asthma and pneumonia, respectively. In patients with bronchial asthma changes in the Hb-CO concentrations significantly correlated with those in FEV1 after 3 weeks of treatment with oral glucocorticoids. Furthermore, the Hb-CO concentrations were significantly correlated with the exhaled CO concentrations, as previously reported.2
The exhaled CO levels in the present study were consistent with those in patients with inflammatory airway and pulmonary diseases such as bronchial asthma, bronchiectasis, upper respiratory tract infections, and seasonal allergic rhinitis as reported previously.3–8 Because exhaled CO is increased in patients with inflammatory airway and pulmonary diseases, it has been proposed that the measurement of exhaled CO may serve as an indirect marker of airway inflammation. Antuni et al also found a significant correlation between the deterioration in FEV1 and exhaled CO concentrations in patients with cystic fibrosis, and suggested that the measurement of exhaled CO is of potential value as an indicator of exacerbations in patients with inflammatory pulmonary diseases.19 The arterial Hb-CO concentration may also therefore reflect inflammation in the airway and lung in inflammatory pulmonary diseases. The estimation of Hb-CO from exhaled CO measurements is considered to be inaccurate in patients with severe airflow obstruction,15 so we measured exhaled CO in patients without severe airway obstruction. Further studies are needed to clarify the relation between the values of exhaled CO and Hb-CO.
HO-1 is upregulated by several factors including oxidative stress and inflammatory cytokines,1 which suggests that increased Hb-CO may not be specific for inflammatory pulmonary disease and that Hb-CO may increase in other acute conditions. Further studies are therefore needed to clarify whether Hb-CO increases in patients with inflammatory diseases other than pulmonary diseases.
It has been shown that exhaled CO can be a reflection of passive smoking in children, suggesting the influence of ambient CO on the values of exhaled CO.14 We determined exhaled CO by subtracting the background levels from the observed reading as described previously.3,6–8 To exclude subjects exposed to cigarette smoking, we measured urinary cotinine concentrations and found them to be less than those used to categorise subjects as having been exposed to cigarette smoke.12 The exhaled CO level is also increased in childhood asthma, but only in children with persistent asthma.14 In contrast, Vreman et al reported that the high levels of exhaled CO were not observed in patients with untreated asthma.20 Further studies are needed to clarify whether exhaled CO may be an indicator of airway and lung inflammation.
In control subjects arterial Hb-CO levels in ex-smokers did not differ from those in non-smokers. Urinary cotinine concentrations confirmed the non-smoking status in patient and control groups.14 CO bound to arterial blood haemoglobin as Hb-CO and exhaled CO therefore appear to be derived from an endogeneous source. Although the source of the CO in Hb-CO and exhaled CO is uncertain, HO-1—the inducible form of HO—is likely to be expressed in airway epithelial cells,21 endothelial cells,22 and alveolar macrophages.4,23
This study provides the first evidence that arterial Hb-CO concentrations in patients with bronchial asthma are significantly higher than in control subjects. Many cytokines are involved in asthmatic inflammation, including interleukin(IL)-1, IL-6, and tumour necrosis factor which can upregulate HO-1 activity in animal and human tissues.24,25 Asthmatic airways produce high levels of NO26–28 and NO decreases cytochrome P450 and microsomal haem through increases in the activity of HO-1.29 High levels of arterial Hb-CO may therefore reflect inflammation of the asthmatic lung.
Arterial Hb-CO concentrations fell in the patients with asthma after 3 weeks of treatment with oral corticosteroids. These findings are consistent with those of previous reports that inhaled and oral corticosteroids reduced exhaled CO in patients with bronchial asthma.3,8 Corticosteroids may reduce arterial Hb-CO by inhibiting HO-1 production in epithelial cells and alveolar macrophages in the lung.21,23 This may be by a direct effect on the HO promoter24 or by inhibition of the synthesis of proinflammatory cytokines24,25 and nitric oxide29 that can induce HO-1 in bronchial asthma.
Histological examinations reveal neutrophil accumulation and infiltration in the lung in bacterial pneumonia.30 Increased levels of reactive oxygen species in neutrophils and bronchoalveolar lavage fluid have been found in inflammatory lung diseases such as cystic fibrosis and adult respiratory distress syndrome.31,32 Reactive oxygen species including superoxide anion and hydrogen peroxide upregulate HO-1 production.33,34 Proinflammatory cytokines and nitric oxide are also increased in experimental pneumonia in rats.35,36 Furthermore, the reactive oxygen species and proinflammatory cytokines are thought to increase exhaled CO in patients with bronchiectasis and cystic fibrosis.5,37 These factors may induce HO-1 production24,25,29,33,34 in bacterial infections of the lung, thereby resulting in increased Hb-CO concentrations in patients with pneumonia.
Gallium-67 citrate scintigraphy, a method used to evaluate alveolitis,16 showed a positive uptake in all patients with IPF. The CRP values in patients with IPF were significantly higher than those in control subjects. Furthermore, the level of KL-6 antigen, a useful indicator of disease activity in patients with IPF,17,18 in peripheral venous blood of patients with IPF was higher than the upper limit of a normal range previously reported by Kohno et al.17 These findings suggest the presence of active alveolar inflammation in patients with IPF. In addition, Hb-CO concentrations in the patients with IPF were significantly correlated with CRP levels, suggesting an association of IPF activity with the increase in Hb-CO levels. Production of various inflammatory factors is observed in patients with IPF and active fibrosing alveolitis, including proinflammatory cytokines,38 reactive oxygen species,39 and NO.40 These factors may upregulate HO-1 production directly24,25,29,33,34 or via the synthesis of NO,41 and may be associated with the increased Hb-CO concentrations seen in patients with IPF in the present study. However, we did not measure Hb-CO in patients with inactive pulmonary fibrosis such as longstanding pneumoconiosis. Further studies are therefore needed to ascertain whether the increase in the Hb-CO concentration is a good marker of inflammation in patients with pulmonary fibrosis.
Hb-CO levels increased after recovery in four patients with bronchial asthma and in two patients with pneumonia. The precise reason is uncertain. However, all six patients had slight symptoms of upper respiratory tract infection such as sneezing and sore throat at the time of the second Hb-CO measurement. The upper respiratory tract infection might relate to the increased Hb-CO values in these patients, as reported previously.6
We have shown that arterial Hb-CO concentrations are increased in patients with inflammatory pulmonary diseases including bronchial asthma, pneumonia, and IPF. Because there was a significant correlation between the arterial Hb-CO concentration and exhaled CO, increased levels of Hb-CO in patients with inflammatory pulmonary diseases may reflect lung inflammation as exhaled CO.3–8 Arterial blood can be taken from patients with inflammatory pulmonary disease or from children who cannot perform the vital capacity manoeuvre to measure exhaled CO. The measurement of Hb-CO could therefore be a simple and valuable marker to indicate pulmonary inflammation.
Acknowledgments
The authors thank G Crittenden for assistance with English.