Article Text

Abstract
Background: The measurement of exhaled nitric oxide (NO) has recently been proposed as a useful technique for the evaluation of airway inflammation in asthma. The purpose of this study was to determine the effect of methacholine bronchial provocation on the levels of exhaled NO in asthmatic children.
Method: Exhaled NO was measurement immediately before and after methacholine provocation in 51 children with mild to moderate asthma.
Results: A significant decrease occurred in the level of exhaled NO (p<0.0001) after methacholine bronchial provocation which was not correlated with the percentage fall in forced expiratory volume in 1 second (FEV1).
Conclusions: The methacholine test should not be used immediately before measurement of exhaled NO in children with asthma.
- exhaled nitric oxide
- asthma
- bronchial hyperresponsiveness
- methacholine
Statistics from Altmetric.com
The measurement of exhaled nitric oxide (NO) has been suggested as an easy non-invasive method for the evaluation of airway inflammation, especially in asthmatic patients.1–4 Recent studies have shown that levels of exhaled NO are decreased by anti-inflammatory treatment,5 so the measurement of NO has been proposed as a method of monitoring the efficacy of treatment in asthmatic patients.6
However, despite the large number of studies of exhaled NO in asthma, the relationship between anti-inflammatory treatment and the decrease in NO levels is not direct or exclusive and additional factors are thought to be involved. Many aspects of the practical use of this method are still unexplored, and the ERS Task Force has suggested that factors influencing NO levels need further research.
This study was performed to determine whether levels of single breath exhaled NO are influenced by methacholine bronchial provocation, one of the most commonly used methods for investigating the presence of bronchial hyperresponsiveness in asthmatic patients.
METHODS
Subjects
Fifty one children aged 6–13 years with mild to moderate asthma according to the American Thoracic Society definition8 were evaluated at the Istituto Pio XII, Misurina BL, Italy. None of the patients had had a respiratory tract infection for at least 1 month before the beginning of the study. The study was approved by the Istituto Pio XII ethics committee and both the children and their parents gave consent to entering the trial.
Study design
Exhaled NO levels were measured immediately before and after a methacholine bronchial provocation test. The post-test measurement was performed when forced expiratory volume in 1 second (FEV1) had decreased by at least 20% compared with the baseline value, or after inhalation of 25 mg/ml methacholine in subjects who failed to show a decrease in FEV1 of at least 20%. Measurement of NO at the end of the test was performed immediately before administration of salbutamol given to reverse the bronchial obstruction induced by methacholine.
Regular treatment with inhaled steroids and long acting β agonists was withheld after admission which was at least 4 weeks before the start of the study. None of the children received oral steroids after admission. Short acting β2 agonists, theophylline, and anticholinergic medications were not allowed during the 24 hours before the methacholine bronchial provocation test (48 hours for long acting theophylline).
In vitro evaluation of effect of methacholine on NO measurement
To determine whether methacholine could directly influence the chemiluminescence signal, and therefore NO readings, an in vitro method similar to that described by van der Mark and coworkers was used.9 Briefly, a 1 litre glass container was filled with 117 ppb NO from a certified bottle and the flow from this bottle was kept constant during the measurement. Predosed deliveries of air from a 25 mg/ml solution of methacholine generated by a MeFar dosimeter (MeFar, Brescia, Italy) were intermittently fed into the glass container through a different access. Samples from the mixing bottle were passed directly into the measuring port of the NO analyser.
Methacholine provocation test
Bronchial hyperresponsiveness was measured by the methacholine bronchial provocation test performed using a MeFar dosimeter (MeFar).10 The dosimeter and ampoules were calibrated to nebulise 0.01 ml of solution in 1.2 s, generating particles ranging from 0.5 to 3.0 μm in diameter. All inhalations were performed by slow inspiration starting from functional residual capacity without reaching total lung capacity, followed by 5 seconds of breath holding. Before administering methacholine, five inhalations of buffer solution were given. One minute after the fifth inhalation of buffer solution, FEV1 was recorded again and the test was continued only if the difference in FEV1 between the two readings was less then 10%. The provocation test was performed in each patient with increasing doses of methacholine. Data were plotted so that concentrations of inhaled methacholine were logarithmically shown on the abscissa and the percentage decrease in FEV1 compared with FEV1 measured after nebulisation of the buffer control were arithmetically shown on the ordinate. The concentration of methacholine required to produce a fall in FEV1 of 20% (PC20, mg/ml) was calculated.10
NO measurement
Exhaled NO was measured using a chemiluminescence analyser (Logan LR 2149, Rochester, Kent, UK).3,4,11 Briefly, subjects were asked to perform a single slow exhalation through a mouthpiece against a resistance and with biofeedback to maintain a steady flow of 50 ml/s. The expiratory pressure was maintained between 5 and 20 cm H2O. This method allows separation of the nasopharynx and oropharynx by the soft palate, preventing contamination of exhaled NO with nasal NO. It has been used successfully in both adults and children. NO was measured at the plateau of the end exhaled reading and expressed in parts per billion (ppb) according to the guidelines.12 Values of NO used in the data analysis were always measured during the last part of exhalation (plateau exhaled NO), taking the plateau of the end exhaled carbon dioxide reading as representative of an alveolar sample.3
Statistical analysis
Data are expressed as mean (SD) and as medians with lower and upper quartiles (Q1, Q3). Differences in NO levels before and after the methacholine test were analysed by the Wilcoxon test; p values of <0.05 were considered significant. Relationships between the investigated parameters were analysed using the Spearman rank correlation test (r coefficient) and were considered significant when p<0.05.
RESULTS
Influence of methacholine on NO levels
Three sets of experiments were performed. The mean (SE) baseline level of NO in the mixing bottle was 113.2 (0.5) ppb. After a predosed delivery of environmental air, the level of NO decreased for a few seconds to 89.2 (0.5) ppb and then increased again to 113.1 (0.7) ppb. Two repeated predosed deliveries of 25 mg/ml methacholine were then performed, both of which resulted in a transient decrease in the NO level in the mixing bottle to 90.1 (0.5) ppb and 90.9 (0.4) ppb, respectively, followed by an increase to 112.7 (0.4) ppb and 112.9 (0.4) ppb, respectively. These data exclude a possible direct chemical effect of methacholine on NO levels measured by chemiluminescence analyser.
NO and methacholine test
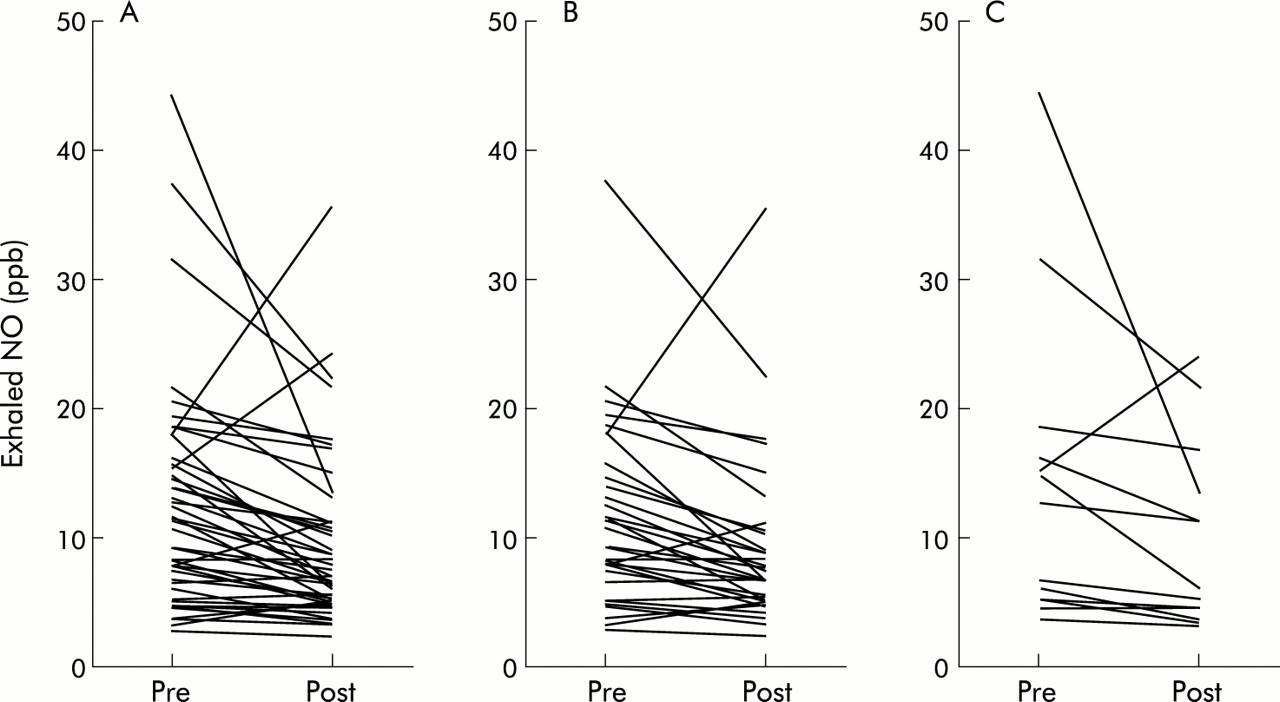
The mean (SE) and median (Q1, Q3) values of PC20 in the 51 children who underwent methacholine bronchial provocation testing are shown in table 1. The level of exhaled NO in this group was significantly reduced after the last dose of methacholine compared with the baseline value (p=0.0001; fig 1A). This was seen in the 38 subjects in whom a fall in FEV1 of more than 20% occurred (p=0.0001; fig 1B) as well as in the remaining 13 subjects who did not have a positive response to methacholine bronchial provocation even after the last dose of 25 mg/ml (p=0.0228; fig 1C).
Mean (SE) and median (lower and upper quartile) values of methacholine PC20 and exhaled NO levels before and after methacholine provocation in 51 children
{kind=link}
Exhaled NO levels before and after methacholine in (A) the whole group (n=51), (B) subjects who had a reduction in FEV1 of >20% after methacholine provocation (n=38), and (C) patients who did not respond to methacholine provocation (n=13).
No correlation was observed between the percentage fall in FEV1 (ΔFEV1) and the percentage fall in NO (ΔNO), either in the whole group (r=0.19, NS) or when the responders (r=0.308, NS) and non-responders (r=0.11, NS) were considered separately.
DISCUSSION
Several studies have shown that the levels of exhaled NO are increased in patients with asthma,1,6,12 particularly during the inflammatory late response to allergen,13 and that they are reduced after treatment with inhaled steroids5 which suggests that the measurement of exhaled NO could be usefully employed as a marker of airway inflammation in asthma.6
In this study we found that the levels of exhaled NO were significantly reduced after methacholine bronchial provocation. Garnier et al14 reported a non-significant decrease in the level of exhaled NO after the methacholine bronchial provocation test in five of seven subjects and an increase in two, raising the possibility that the results could have been affected by the small number of subjects.
The mechanism by which the level of exhaled NO is reduced after the bronchial methacholine test is not clear. In a previous study de Gouw et al15 observed a decrease in the NO level after bronchial provocation with histamine and adenosine-5`-monophosphate which was significantly correlated with the percentage fall in FEV1. The authors concluded that the fall in the NO level was not caused by the procedure itself but was related to the acute decrease in FEV1, suggesting that exhaled NO levels are modulated by the degree of airways obstruction.15 This explanation, however, is only partially applicable to the results of our study. We observed a statistically significant decrease in exhaled NO levels after methacholine provocation in both the subjects who responded with a fall in FEV1 of more than 20% and in those who did not. Furthermore, the decreases in exhaled NO and in FEV1 after inhalation of methacholine were not significantly correlated.
It is difficult to know which mechanism is responsible for the decrease in the single breath exhaled NO concentration after the methacholine provocation test in asthmatic children, but there are several possibilities. A number of studies have shown that repeated forced expiratory manoeuvres can reduce exhaled NO levels for a few hours.16,17 However, we did not find any significant difference in the percentage reduction in exhaled NO in the 15 patients who had high bronchial reactivity and in whom the provocation test was stopped after a few doses of methacholine and a low number of spirometric tests compared with the 15 patients who had lower reactivity and who therefore completed most or all of the steps of the bronchial provocation test (p=0.77, NS). The mechanisms by which methacholine and exercise induce bronchial constriction are different, and different hypotheses may be advanced to explain the observed decrease in single breath NO in our study population.
Methacholine is a direct pharmacological agent which induces transient bronchoconstriction accompanied by a moderate fall in Pao2 caused by ventilation/perfusion mismatch with an intrapulmonary shunt.18 On this basis we can hypothesise, although not demonstrate, that the observed decrease in single breath exhaled NO could be due to the effect of areas of altered ventilation/perfusion caused by local peripheral airway obstruction. It is indeed tempting to speculate that NO originating in constricted hypoventilated airways may be trapped in the bronchi and not exhaled. The lack of correlation between the fall in exhaled NO levels and in FEV1 after provocation may be due to a maldistribution in ventilation. This has previously been suggested to be responsible for the better correlation between airway resistance and ventilation/perfusion than airway flux (FEV1).19
In conclusion, although we are unable to demonstrate the mechanisms, our results show a decrease in the concentration of exhaled NO after the methacholine provocation test in children with mild to moderate asthma. We suggest that the methacholine test should not be used immediately before NO measurement in asthmatic children.
Acknowledgments
The authors thank Valeas for supplying the NO analyser used in the study.