Article Text

Abstract
Background: Patients with chronic obstructive pulmonary disease (COPD) are prone to frequent exacerbations which are a significant cause of morbidity and mortality. Stable COPD patients often have lower airway bacterial colonisation which may be an important stimulus to airway inflammation and thereby modulate exacerbation frequency.
Methods: Twenty nine patients with COPD (21 men, 16 current smokers) of mean (SD) age 65.9 (7.84) years, forced expiratory volume in 1 second (FEV1) 1.06 (0.41) l, FEV1 % predicted 38.7 (15.2)%, FEV1/FVC 43.7 (14.1)%, inhaled steroid dosage 1.20 (0.66) mg/day completed daily diary cards for symptoms and peak flow over 18 months. Exacerbation frequency rates were determined from diary card data. Induced sputum was obtained from patients in the stable state, quantitative bacterial culture was performed, and cytokine levels were measured.
Results: Fifteen of the 29 patients (51.7%) were colonised by a possible pathogen: Haemophilus influenzae (53.3%), Streptococcus pneumoniae (33.3%), Haemophilus parainfluenzae (20%), Branhamella catarrhalis (20%), Pseudomonas aeruginosa (20%). The presence of lower airway bacterial colonisation in the stable state was related to exacerbation frequency (p=0.023). Patients colonised by H influenzae in the stable state reported more symptoms and increased sputum purulence at exacerbation than those not colonised. The median (IQR) symptom count at exacerbation in those colonised by H influenzae was 2.00 (2.00–2.65) compared with 2.00 (1.00–2.00) in those not colonised (p=0.03). The occurrence of increased sputum purulence at exacerbation per patient was 0.92 (0.56–1.00) in those colonised with H influenzae and 0.33 (0.00–0.60) in those not colonised (p=0.02). Sputum interleukin (IL)-8 levels correlated with the total bacterial count (rho=0.459, p=0.02).
Conclusion: Lower airway bacterial colonisation in the stable state modulates the character and frequency of COPD exacerbations.
- chronic obstructive pulmonary disease
- exacerbation frequency
- bacterial colonisation
Statistics from Altmetric.com
Some patients with chronic obstructive pulmonary disease (COPD) are prone to frequent exacerbations which are a major cause of morbidity and mortality and an important determinant of health related quality of life.1 The mechanisms modulating exacerbation frequency in patients with COPD are largely unknown. Reduction of exacerbation frequency may have significant benefits, although few interventions are currently effective.
A significant proportion of patients with COPD have lower airway bacterial colonisation with a spectrum of pathogens including non-typeable Haemophilus influenzae, Streptococcus pneumoniae, and Branhamella catarrhalis.2,3 Risk factors for colonisation include the degree of airways obstruction2 and current smoking.4 The presence of bacteria in the lower airways of patients with COPD implies a breach of host defence mechanisms which sets up a vicious cycle of epithelial cell damage, impaired mucociliary clearance, mucus hypersecretion, increased submucosal vascular leakage and inflammatory cell infiltration, thereby promoting further dysfunction of host defences and bacterial adherence and growth.5,6 Bacterial colonisation may also contribute directly to airway inflammation.7–9 We have recently shown that patients with frequent exacerbations have higher induced sputum levels of interleukins IL-6 and IL-8 in the stable state than patients with infrequent exacerbations.10 This suggests that patients with frequent exacerbations may have a higher incidence of bacterial colonisation. However, the role of bacterial colonisation in modulating airway inflammation in patients with frequent exacerbations is unknown.
This study was designed to evaluate the relation between bacterial colonisation in stable patients and exacerbation frequency, character, and time course. Sputum samples were obtained from patients followed in the East London COPD cohort. These patients completed daily diary cards for changes in symptoms and peak flow and reported exacerbations to the study team as previously described.11 A validated exacerbation frequency was calculated for each patient and this was related to the detection of bacterial colonisation and airway cytokine levels when patients were stable. The symptoms at exacerbation and the recovery from exacerbations were also compared in colonised and non-colonised patients.
METHODS
Study subjects
Twenty nine stable patients with moderate to severe COPD were recruited as volunteers from those in the East London COPD Study, which is a prospective cohort based study of COPD exacerbations. COPD was defined as forced expiratory volume in 1 second (FEV1) of less than 70% predicted for age and height, β2 agonist reversibility on predicted FEV1 of less than 15% and/or 200 ml, with airflow obstruction as evidenced by a ratio of FEV1 to forced vital capacity (FVC) of less than 70%. Patients with a history of asthma, bronchiectasis, carcinoma of the bronchus, or other significant respiratory disease, or those unable to complete diary cards were excluded and all patients received influenza vaccination as recommended for this group. Subjects were recruited when stable, without any evidence of an exacerbation for at least 3 weeks. At recruitment baseline measurements were made of height, weight, FEV1, FVC, and peak expiratory flow rate (PEFR) by rolling seal spirometer (Sensor Medic Corp, Yorba Linda, USA). Reversibility to 400 μg inhaled salbutamol was determined using a metered dose inhaler via spacer, and arterialised ear lobe blood gases were analysed for arterial oxygen and carbon dioxide partial pressures.12 Smoking habits (current smoking status, years of smoking, and number of packs of 20 cigarettes smoked per day), drug history, daily stable respiratory symptoms (baseline symptoms), and history of exacerbations were also noted.
COPD exacerbations
All patients maintained daily diary cards on which they recorded their indoor PEFR measured with a mini-Wright peak flow meter (Clement Clarke International Ltd, Harlow, UK) after their morning medication. Patients also noted any appearance or increase in intensity of “major” symptoms (dyspnoea, sputum purulence, sputum amount) or “minor” symptoms (nasal discharge/congestion, wheeze, sore throat, cough) over their chronic (stable) symptoms on their diary cards. A member of the study team saw patients within 48 hours of the detection of deterioration in symptoms and the diagnosis of an exacerbation was confirmed in each case. Exacerbations were identified according to defined criteria of any two major symptoms or one major and one minor symptom, as described above, on two consecutive days, the first of which was taken as the day of onset of exacerbation.1,10,11 Exacerbation numbers were calculated from diary cards for an 18 month period of follow up comprising the 12 month period before sampling and the following 6 months.
Sputum induction
Stable patients attended the research clinic in the morning for baseline sputum sampling. They were questioned and diary cards were examined to confirm the absence of an exacerbation over the preceding 3 weeks, as defined by our previously validated criteria.11 Measurement of oxygen saturation (Minolta Pulsox 7, DeVilbiss Healthcare, Heston, Middlesex, UK) and spirometric tests were performed on arrival and repeated 10 minutes after premedication with 200 μg inhaled salbutamol via a metered dose inhaler. Patients were instructed to blow their noses and rinse their mouths out with water before sputum induction was performed. This was done using the DeVilbiss UltraNeb2000 nebuliser (DeVilbiss Healthcare) with 3% saline as described previously.13 This nebuliser produced an aerosol output of approximately 2 ml/min with a mean particle size of 0.5–5 μm in diameter. After 7 minutes of nebulisation, measurements of oxygen saturation and spirometric tests were performed and, if no sputum was produced, nebulisation was continued for a further 7 minutes if the FEV1 had not fallen by more than 20%.
Sputum examination
Sputum samples were examined as soon as possible within 2 hours of collection using methods adapted from evaluated protocols.13 One third of the sample was taken for quantitative bacterial culture while the remainder was separated from contaminating saliva by macroscopic examination using disposable plastic forceps. Half of the selected portion of the sputum was mixed with four times its weight of 0.1% dithiothreitol (DTT) solution, vortexed for 15 seconds, and then rocked for 15 minutes. A weight of Hank's balanced salt solution (HBSS) equal to that of the sputum plus DTT was then added and the whole mixture was rocked for a further 5 minutes. The suspension was filtered through 50 μm nylon gauze to remove mucus and debris and centrifuged at 790g (2000 rpm) at 4°C for 10 minutes. This resulted in the formation of a cell pellet and supernatant solution. The other half of the selected portion of the sputum was mixed with nine times its weight of phosphate buffered saline (PBS) and agitated with siliconised glass beads 1–2 mm in diameter (BDH Chemicals Ltd, Poole, Dorset, UK). This was then filtered and centrifuged as before to provide a cell pellet and supernatant. The supernatants from both processes were decanted and stored at –70°C. The cell pellet from the DTT processed part of the sample was resuspended in 800–1600 μl HBSS and the total cell count was determined with a Neubauer haemocytometer using the tryptan blue exclusion method to determine cell viability. The absolute number of non-squamous cells per g of original sputum sample was determined and the percentage of viable and non-viable cells obtained. The cell suspension was diluted with HBSS to obtain a count of 0.6–1.0 × 106 cells/ml and cytospins were made using a Cytotek centrifuge. The cytospin slides were stained with Diffquik to obtain differential cell counts.
Estimation of induced sputum inflammatory markers
Levels of IL-6 and IL-8 in the DTT processed supernatants and secretory leucoprotease inhibitor (SLPI) in the PBS processed supernatants were measured using quantitative sandwich immunoassay techniques (R&D Systems Europe, Abingdon, Oxon, UK).
Quantitative identification of bacteria
Sputum samples were processed by adding an equal weight of sputolysin (Sputasol; Unipath, Hampshire, UK) and several glass beads (1–1.5 mm in diameter) and incubated for 30 minutes at 37°C during which they were vortexed for 5–10 seconds intermittently. Tenfold serial dilutions of the homogenised sample were made in brain heart infusion broth and 100 μl aliquots were plated out onto the surface of a range of different media including blood agar, chocolate agar, MacConkey agar, and cysteine lactose electrolyte deficient agar. These were incubated for 18 hours at 37°C in an atmosphere of air + 5% CO2. After incubation, bacterial colonies were counted and subcultured for identification by standard methods.14 The number of colony forming units/g sputum was calculated from the number of colonies obtained and the dilution of the sputum.
All estimations of inflammatory mediators and bacterial colonisation were performed by observers blind to the clinical characteristics of the patients in the study.
Statistical analysis
Normally distributed data are presented as mean (SD) values and skewed data as median (interquartile range, IQR) values. Continuous variables with normal distributions were compared by two tailed unpaired t tests while those with non-normal distributions were compared by the Mann-Whitney U or Wilcoxon signed ranks test as appropriate. Sputum IL-8 levels and total bacterial counts were correlated using Spearman's rank correlation. Categorical binary variables were compared using the χ2 test and the odds ratio was calculated. The median exacerbation frequency for this group was 2.58 per patient per year, in agreement with previously published results,1 and this was taken as the cut off point to divide patients into either frequent or infrequent exacerbators. The sum of the number of symptoms, of the major and minor symptoms listed above, gave the symptom count for each day of an exacerbation. The mean value for the specific and total symptom counts for the exacerbation was calculated for each patient. These non-normally distributed values were compared between patients with and without bacterial colonisation. The time course for recovery of symptoms and lung function was analysed as above to ascertain any relationship between recovery time for exacerbations and the presence of bacterial colonisation in the stable state. Data analysis was performed using SPSS for Windows version 10 for STATA 5.0.
RESULTS
Patients
Table 1 shows the baseline physiological characteristics of the 29 patients studied; 27 patients were on inhaled steroids, 16 were current smokers, and 19 were daily sputum producers. Table 2 compares the physiological characteristics of the frequent (n=14) and infrequent (n=14) exacerbators; the two groups were similar except the infrequent exacerbators were significantly older (p=0.02). One patient who left the study shortly after being sampled was excluded from the exacerbation analysis and therefore prospective data were not available on his exacerbations.
Mean (SD) baseline physiological characteristics of the patients sampled (n=29)
Mean (SD) baseline physiological characteristics of the patients grouped by exacerbation frequency
Exacerbations
Diary card data were analysed to confirm that the peak flow and symptoms were at baseline on the day of sampling. The median time from the last exacerbation to the date of sputum sampling was 23 weeks (range 3.7–66.7). The median time to recovery of peak flow after the last exacerbation was 3.5 days (range 1–39). Patients sampled had recovered their pre-exacerbation peak flow at the time of sampling and had no symptoms of an ongoing exacerbation.
Ninety four exacerbations were documented over the study period of which four (in three patients) required hospital admission. Fifty one (54.3%) of the 94 exacerbations were treated with oral antibiotics and 20 (21.3%) were treated with oral prednisolone.
Bacterial isolates
Figure 1 shows the possible pathogens recovered in induced sputum. Fifteen of the 29 induced sputum samples (51.7%) yielded a positive culture of one or more potentially pathogenic microorganisms as previously defined.3 Pathogens recovered included Haemophilus influenzae (8/15, 53.3%), Streptococcus pneumoniae (5/15, 33.3%), Haemophilus parainfluenzae (3/15, 20%), Branhamella catarrhalis (3/15, 20%), and Pseudomonas aeruginosa (3/15, 20%). Seven of the 15 colonised patients had multiple organisms. “Non-specific growth” (NSG) was defined as the isolation of non-pathogenic microorganisms which are not usually involved in respiratory infections in immunocompetent hosts (Streptococcus viridans group, Neisseria spp, Corynebacterium spp, and coagulase negative staphylococci).15 The total bacterial count was significantly higher in those specimens colonised by a possible pathogen; the mean bacterial count was 107.90 cfu/ml in colonised samples and 107.03 cfu/ml in samples with non-specific growth (p=0.004).
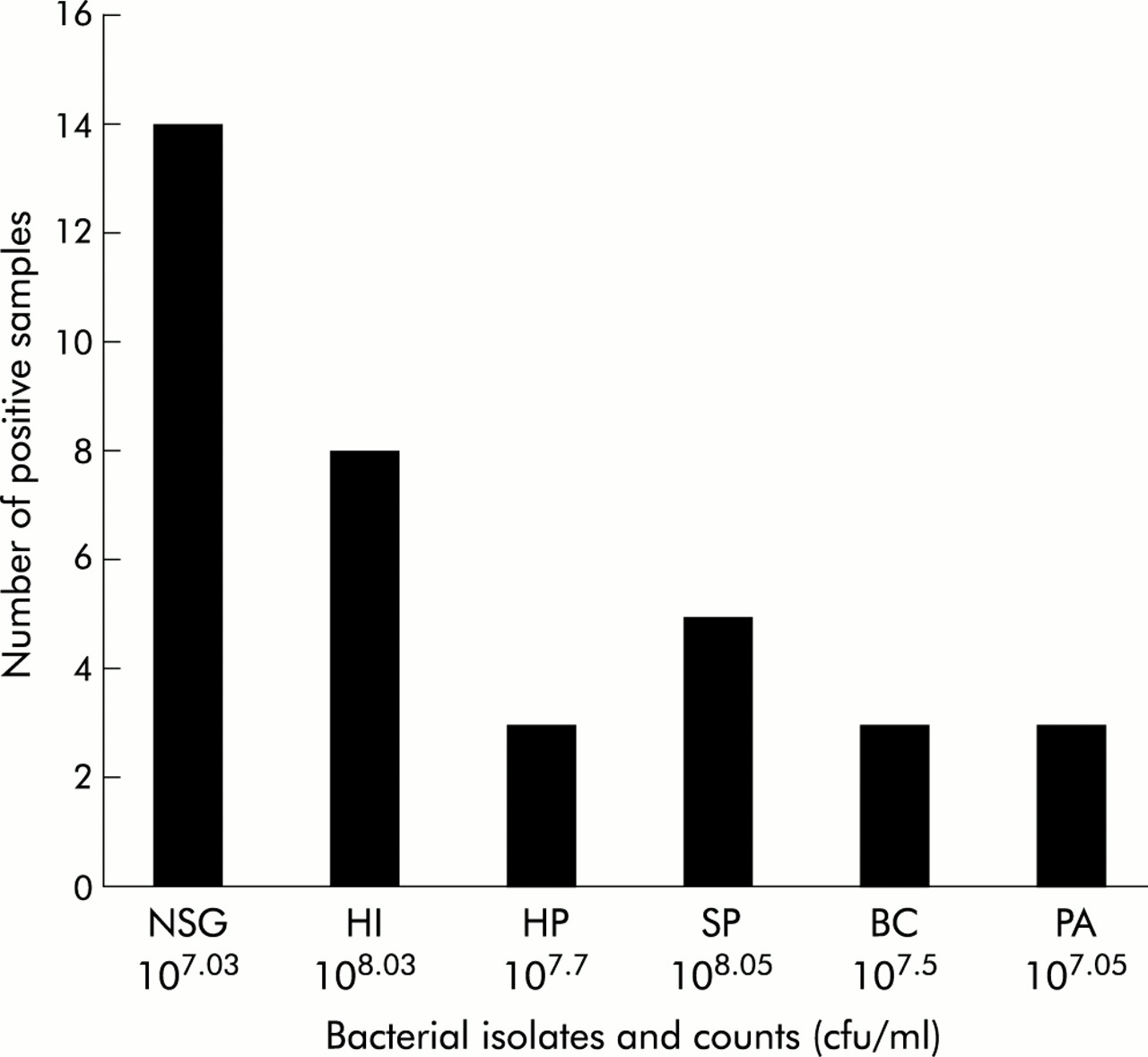
Possible pathogens recovered in induced sputum. Mean bacterial counts (colony forming units per ml, cfu/ml) in each group are expressed below isolates. NSG=non-specific growth; HI=Haemophilus influenzae; HP=Haemophilus parainfluenzae; SP=Streptococcus pneumoniae; BC=Branhamella catarrhalis; PA=Pseudomonas aeruginosa.
Bacterial colonisation and exacerbation frequency
Patients were followed up for a median (IQR) of 529 (168–546) days and exhibited a median annual exacerbation rate of 2.58 (0.70–3.68) per year. Analysis of diary cards showed that colonisation with any possible pathogen was associated with increased exacerbation frequency (p=0.023, χ2 test, odds ratio 6.25, fig 2). Bacterial colonisation in the stable state showed a trend towards association with symptoms of daily dyspnoea (p=0.058, χ2 test). Colonisation was not related to daily sputum production, current smoking, or airways obstruction, and no differences were found between colonised and non-colonised patients in terms of symptoms at exacerbation or exacerbation severity as measured by fall in peak flow, recovery, or hospital admission.

Relationship between lower airway bacterial colonisation (LABC) by a possible pathogen in induced sputum and frequent (>2.58 exacerbations per year; n=14) and infrequent exacerbations (<2.58 exacerbations per year; n=14) with 95% confidence intervals.
Haemophilus influenzae colonisation and symptoms
Analysis of diary card data showed that patients colonised by H influenzae in the stable state reported more symptoms and increased sputum purulence at exacerbation than those not colonised (table 3). Patients colonised with H influenzae also had more cough and a longer time to recovery of peak flow at exacerbation than those not colonised, although these findings just failed to reach statistical significance. There was no difference between the two groups in the fall in peak flow at exacerbation. Colonisation by H influenzae was not related to smoking status or inhaled steroid treatment; however, a trend was seen towards a relationship between colonisation and mean FEV1 % predicted (43.6 (17.3)% in patients not colonised with H influenzae and 34.0 (10.8)% in those colonised, p=0.09).
Symptom characteristics at exacerbation of patients colonised by Haemophilus influenzae in the stable state
Airways inflammation and bacterial colonisation
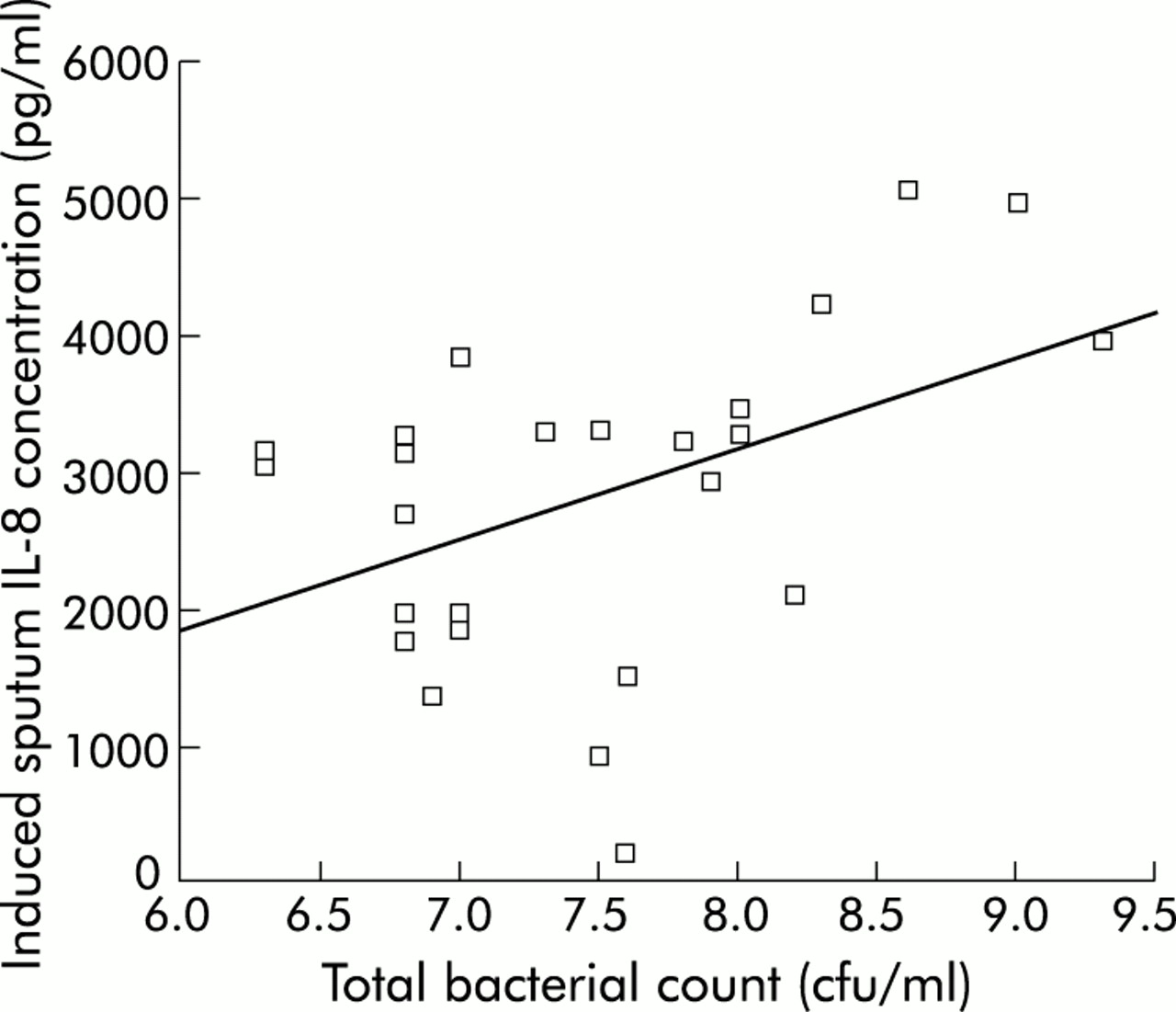
Induced sputum IL-8 levels correlated with the total bacterial count (rho=0.459, p=0.02; fig 3). The median (IQR) IL-8 level in colonised samples was 3301 (2126–4262) pg/ml and in non-colonised samples was 2476 (1712–3212) pg/ml (p=0.07). SLPI levels were lower in induced sputum samples colonised with a possible pathogen (median (IQR) 2.68 (0.85–3.68) pg/ml) than in non-colonised samples (3.92 (2.72–4.99) pg/ml (p=0.04)). IL-6 levels were not related to bacterial colonisation (median (IQR) 103.5 (56.6–166.8) pg/ml in colonised samples v 113.2 (76.2–127.0) pg/ml in those not colonised, p=0.78).

{kind=link}
{kind=link}
{kind=link}
Relationship between total bacterial count (colony forming units/ml) and induced sputum IL-8 levels (Spearman's rho=0.459, p=0.02). The bacterial count data have been logarithmically transformed.
DISCUSSION
This study was designed to evaluate the relationship between bacterial colonisation and the character and frequency of exacerbations in COPD. The presence of bacterial colonisation in the stable state was associated with increased exacerbation frequency over the study period. Colonisation by non-typeable H influenzae in the stable state was associated with increased total symptom count and sputum purulence at exacerbation.
Exacerbation frequency is now being recognised as an important feature of the natural history of COPD, with important implications for health related quality of life1 and hospital admission.16 Our patients filled in daily diary cards for peak flow and symptoms over an 18 month period. They were seen 3 monthly for spirometric tests and diary card review and within 48 hours of developing an exacerbation. A carefully validated exacerbation frequency was calculated for each patient according to our previously defined criteria,11 enabling relationships between baseline sputum bacteriology and exacerbation frequency to be examined.
Our group has shown previously that patients with frequent exacerbations have heightened airway inflammation when stable as measured by induced sputum IL-6 and IL-8 levels.10 We postulated that this might be due to the presence or load of bacteria in the lower airways. In this study we have confirmed that the bacterial count is related to the sputum level of IL-8, a neutrophil chemoattractant. COPD is characterised by predominantly neutrophilic airway inflammation and enhanced neutrophil chemotactic responses.17–19 While this is thought to represent an exaggerated response to tobacco smoking,20,21 there is also evidence that bacterial products affect neutrophil migration22 and may independently modulate airway inflammation.23 Bacterial numbers are related to sputum levels of IL-8 and leucocyte elastase activity in chronic bronchitis.8 In addition, Soler et al recently showed that bacterial colonisation in the distal airways is associated with increased polymorphonuclear cells and tumour necrosis factor (TNF-α) in bronchoalveolar lavage fluid from patients with COPD.7 Our finding that SLPI levels were lower in induced sputum samples colonised with a possible pathogen is consistent with those of other reports which have found lower levels of SLPI in spontaneous sputum samples from patients with stable chronic bronchitis colonised by Pseudomonas aeruginosa.8 Further work is required to evaluate factors that modulate the expression and secretion of SLPI by epithelial cells.
Bacterial products have also been shown to stimulate mucin secretion.24 Chronic mucus hypersecretion is associated with increased sputum neutrophilia, accelerated decline in lung function,25 and increased likelihood of death from pulmonary infections in patients with COPD.26 Despite this evidence, the impact of bacterial colonisation on the natural history of COPD remains unclear. This is the first study to show that patients with bacterial colonisation have increased numbers of exacerbations, suggesting that the presence of bacteria in the lower airways in this patient group is clinically relevant.
Previous authors have identified the degree of airways obstruction2 and current smoking4 as risk factors for bacterial colonisation in COPD. We did not find these relationships in this study, although a trend towards a relationship with airways obstruction was seen in patients colonised by H influenzae. Our patients all had relatively severe COPD with a mean (SD) FEV1 of 38.7 (15.2)% predicted which minimised the chances of finding significant correlations between lesser and greater degrees of airways obstruction and bacterial colonisation. Indeed, this may also explain the relatively high prevalence of bacterial colonisation observed in our cohort of patients (51.7%) compared with that described in other studies. Similarly, only one third of the 29 patients studied were current smokers, which may explain why this parameter did not relate to bacterial colonisation.
The mechanisms by which bacterial colonisation modulates exacerbation frequency are not known. In this study the aetiology of the exacerbations was not investigated. We have previously shown that a significant proportion of exacerbations in our cohort of COPD patients have a viral aetiology, most commonly human rhinovirus infection.27,28 Superadded bacterial infection, possibly by colonising organisms, is often assumed and this informs common clinical decisions to treat exacerbations with antibiotics. There is evidence that viral infection can facilitate the adherence and spread of bacteria including S pneumoniae and H influenzae in the respiratory tract of normal subjects,29,30 and that interactions between viruses and bacteria occur in patients with chronic bronchitis.31 Human rhinovirus attaches to airway epithelium through ICAM-1,32 and H influenzae endotoxin has been shown to stimulate the expression of ICAM-1 by cultured human bronchial epithelial cells.33 It is therefore possible that lower airway bacterial colonisation modulates the response to a viral infection in COPD.
We have previously shown that patients with frequent COPD exacerbations have worse symptom scores resulting in impaired health related quality of life.1 Colonised patients tended to report more baseline dyspnoea in the stable state and this is therefore the first study to suggest an association between symptoms and bacterial colonisation in COPD. Bacterial products and the chronic inflammatory response they elicit in the airway cause epithelial cell damage34,35 which, in the small airways, may contribute to the respiratory bronchiolitis and progressive airway obstruction seen in COPD.36
Patients colonised with H influenzae in the stable state reported more sputum purulence and total symptoms during exacerbations. This is consistent with the finding that exacerbations of COPD in which this organism has been isolated have higher sputum levels of IL-8, neutrophil elastase, and TNF-α,37 and are associated with greater functional impairment.38 Stockley et al39 have shown that sputum purulence is associated with the detection of a bacterial pathogen at exacerbation. It is therefore likely that patients who were colonised at baseline by H influenzae were more likely to develop bacterial exacerbations. Endogenous reinfection with H influenzae strains has been shown at exacerbation in patients with COPD.40 Patients colonised with H influenzae in the stable state also had longer times to recovery of their peak flow after an exacerbation, suggesting that lower airway bacterial colonisation may contribute to decline in lung function in COPD.
Patients were sampled at one time point and the resulting data were related to the number and character of exacerbations over the study period. While it is known that bacteria persist in the lower airway, there is also evidence that bacterial colonisation is a dynamic process with variations in bacterial surface antigens occurring over time.41 It is therefore possible that the bacterial populations and counts were not constant over the period of follow up. However, the relationship with exacerbation frequency was found with colonisation with any pathogen, and not with one particular organism. There have been no reported eradication treatment studies in COPD, and it is not known whether, once colonised, the lower airways can be rendered sterile.
A recent study found that 29% of patients with a primary care diagnosis of COPD had evidence of bronchiectasis on high resolution CT scanning.42 The clinical relevance of this finding, and of any relationships that may exist between bacterial colonisation, unrecognised bronchiectasis, and exacerbation frequency in COPD, are not known. The findings of this study suggest that this is an area that would merit further investigation.
Bacterial infection has been implicated in the pathogenesis and long term progression of diseases such as cystic fibrosis and bronchiectasis, although its role in COPD is only now being clarified. This study has shown a relationship between lower airway bacterial colonisation and exacerbation frequency, a major determinant of health related quality of life. Longitudinal studies with repeated sampling and molecular typing are now required to examine the dynamics and time course of bacterial colonisation more closely and to relate the organisms present in patients with COPD when stable and during exacerbations to levels of airway inflammation and exacerbation frequency.
Acknowledgments
The authors thank Dr Mark Roland for assistance with data collection and sampling and Angela Whiley for performing the quantitative bacteriology. The study was supported by the Joint Research Board of St Bartholomew's Hospital.