Article Text

Abstract
Background: Patients with chronic obstructive pulmonary disease (COPD) have increased numbers of neutrophils and macrophages in their lungs. Growth related oncogene-α (GROα) attracts neutrophils, whereas monocyte chemoattractant protein-1 (MCP-1) attracts monocytes that can differentiate into macrophages. The aim of this study was to determine the concentration of GROα and MCP-1 in bronchoalveolar lavage (BAL) fluid and sputum from non-smokers, healthy smokers and patients with COPD, and to see if there was a correlation between the concentrations of these chemokines, lung function, and numbers of inflammatory cells.
Methods: BAL fluid and sputum from non-smokers (n=32), healthy smokers (n=36), and patients with COPD (n=40) were analysed for the presence of GROα and MCP-1 using ELISA. Cells counts were performed on the samples and correlations between the concentrations of these chemokines, lung function, and inflammatory cells observed.
Results: Median (SE) GROα and MCP-1 levels were significantly increased in sputum from patients with COPD compared with non-smokers and healthy smokers (GROα: 31 (11) v 2 (2) v 3 (0.8) ng/ml; MCP-1: 0.8 (0.4) v 0.2 (0.1) v 0.1 (0.04) ng/ml, p<0.05), but not in BAL fluid. There were significant negative correlations between both GROα and MCP-1 levels in sputum and forced expiratory volume in 1 second (FEV1) % predicted (GROα: r=–0.5, p<0.001; MCP-1: r=–0.5, p<0.001), together with significant positive correlations between GROα and MCP-1 and neutrophil numbers in sputum (GROα: r=0.6, p<0.001; MCP-1: r=0.4, p<0.01).
Conclusion: These results suggest that GROα and MCP-1 are involved in the migration of inflammatory cells, thus contributing to the inflammatory load associated with COPD.
- chronic obstructive pulmonary disease
- GROα
- MCP-1
Statistics from Altmetric.com
Patients with chronic obstructive pulmonary disease (COPD) have increased numbers of neutrophils in bronchoalveolar lavage (BAL) fluid1 and induced sputum2 compared with healthy controls. Moreover, macrophage numbers are also increased 5–10 times in BAL fluid of patients with COPD compared with normal subjects.1 These macrophages might be responsible for the continued proteolytic activity in the lungs of patients with COPD with emphysema.1 Furthermore, macrophages may play an important role in driving the inflammatory process by recruiting neutrophils via the release of neutrophil chemotactic factors.1
Monocytes are derived from undifferentiated haemopoietic stem cells in the bone marrow.3 Myeloid progenitors in the bone marrow differentiate into promocytes and then into blood monocytes. Cells from this circulating pool migrate through the blood vessel walls into various organs and then differentiate into macrophages.3 Macrophages are the predominant defence cell in the normal lung and are increased during conditions associated with chronic inflammation such as COPD. In non-smokers macrophages are the major host defence cells in the lower airspace. Cigarette smoking is associated with a 5–10 fold increase in the total cells recovered from BAL fluid with macrophages comprising 95–98% of the total cell count.4
Leucocytes, including monocytes and neutrophils, migrate in response to a number of chemotactic stimuli which include chemokines. Monocyte chemoattractant protein-1 (MCP-1) is an 8.7 kDa CC chemokine produced by monocytes, T lymphocytes, fibroblasts, endothelial cells, smooth muscle cells, and keratinocytes.5 It is an activating factor of both monocytes and T lymphocytes and can act as a chemoattractant.5 It is expressed in various tissues including the lungs, where it is expressed by macrophages, endothelial, bronchial epithelial, and smooth muscle cells.5 Capelli et al6 reported increased concentrations of MCP-1 in BAL fluid from smokers with or without chronic bronchitis compared with healthy non-smoking subjects, suggesting that this chemokine might play a role in the inflammatory cell recruitment associated with cigarette smoking.
Growth related oncogene-α (GROα) is a CXC chemokine first reported as an endogenous growth factor for human melanoma cells.7 It is produced by a variety of cells including monocytes, endothelial cells, fibroblasts, and synovial cells. It can be induced by tumour necrosis factor (TNF)-α in human bronchial epithelial cells and by lipopolysaccharide in alveolar macrophages.8 GROα is structurally related to interleukin 8 (IL-8) and is a powerful activator of neutrophils, demonstrating chemotactic ability for neutrophils, T lymphocytes and basophils.7,9 The inducibility of GROα in the airway by inflammatory stimuli would suggest a role for this chemokine in the recruitment of inflammatory cells such as neutrophils and lymphocytes in diseases such as COPD.
The aim of this study was to determine the concentration of GROα and MCP-1 in BAL fluid and induced sputum from non-smokers, healthy smokers, and patients with COPD, and to see if there was a correlation between the concentrations of these chemokines, lung function, and inflammatory cells in the lungs of these subjects.
METHODS
Patients
Subjects with stable COPD were recruited from the outpatient department of the Royal Brompton Hospital and from a general practice database by searching for smokers over the age of 40. All subjects had a smoking history of at least 20 pack years. Inclusion criteria for entry were forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio of <0.7, FEV1 % predicted <70%, reversibility with inhaled bronchodilators of <15% of predicted FEV1; all criteria were required. Subjects who had taken inhaled or oral steroids or who had suffered an exacerbation of their airway disease in the previous 6 weeks were excluded.
Non-smokers and healthy smokers were recruited from patients undergoing investigations for other reasons and from within the Department of Thoracic Medicine at the National Heart and Lung Institute. Inclusion criteria for non-smokers were no history of respiratory or allergic disease, normal baseline spirometric parameters as predicted for age, sex and height, normal bronchial reactivity as evidenced by a concentration of methacholine provoking a fall in FEV1 of 20% or more (PC20 methacholine) of >64 mg/ml, no evidence of atopy on skin prick testing to common aeroallergens (grass pollen, cat hair, house dust mite or Aspergillus fumigatus), no smoking history, no history of upper respiratory tract infection in the preceding 6 weeks, and not taking any regular medication. Inclusion criteria for healthy smoking subjects was the same as for the non-smokers but they were required to have a smoking history of at least 10 pack years. Although the non-smokers and healthy smokers were not age matched with the COPD patients, no relationship between age and chemokine expression in the airways has been reported. No subject underwent both bronchoscopy and sputum induction.
All subjects gave written informed consent and the study was approved by the East Berkshire ethics committee and the Royal Brompton Hospital ethics committee.
Materials
96-well ELISA plates were purchased from Nunc, Paisley, UK; all antibodies and chemokines were purchased from R&D Systems Ltd (Abingdon, UK). Strepavidin-horse radish peroxidase was purchased from Zymed Laboratories (San Francisco, CA, USA). Microcon YM-3 filters were purchased from Millipore (Watford, UK). All other reagents were purchased from Sigma Chemical Co (Poole, UK) or BDH (Poole, UK).
Bronchoscopy and bronchoalveolar lavage
Bronchoscopy, BAL fluid collection and processing were performed as previously described.10 Subjects were pretreated with atropine (0.6 mg intravenously) and midazolam (5–10 mg intravenously). Throughout the procedure oxygen (3 l/min) was administered via nasal prongs. After induction of local anaesthesia to the upper airways and larynx, a fibreoptic bronchoscope was passed through the nasal passages into the trachea. Bronchoalveolar lavage was performed on the right middle lobe using four successive aliquots each of 60 ml of warmed 0.9% (w/v) NaCl.10 Patients abstained from smoking for 2 hours prior to bronchoscopy.
Sputum induction and processing
Induced sputum samples from non-smokers, healthy smokers, and patients with COPD were collected and processed. Subjects inhaled 3.5% (w/v) saline for 15 minutes via an ultrasonic nebuliser (DeVilbiss 2000; DeVilbiss Co, Heston, UK) with a calibrated mass median diameter of 4.5 μm and output setting of 4.5 ml/min. Before inhalation and before each expiration subjects discarded saliva into a separate bowl and mouthwashed thoroughly. Any secretions collected during the first 5 minutes were discarded to minimise squamous buccal epithelial cell contamination. Secretions expectorated over the subsequent 10 minutes, hereafter referred to as sputum, were analysed. Fresh samples were kept at 4°C for no more than 2 hours before processing.
Whole sputum samples were diluted in Hank's balanced salt solution (HBSS) containing 0.05% (w/v) dithiothreitol (DTT), with a final DTT concentration of 0.05% (w/v), and were gently vortexed at room temperature. When homogeneous, the volume was recorded and the sample was further diluted with HBSS to 5–10 ml and centrifuged at 300g for 10 minutes. The supernatant was separated and stored at –70°C.11
Neutrophil and macrophage cell counts in BAL fluid and sputum
Differential cell counts were performed as previously described.11,12 Total cell counts were determined on a haemocytometer slide using Kimura stain, and slides were prepared using a cytospin (Shandon, Runcorn, UK) and stained with May-Grunwald-Giesma.
Measurement of GROα
GROα was measured using an enzyme linked immunosorbent assay (ELISA). Plates were washed between incubations with phosphate buffered saline (PBS) containing 0.05% (v/v) Tween 20. Monoclonal anti-human GROα (4 μg/ml) was coated onto 96-well plates and incubated overnight at room temperature (RT). The plates were blocked for 1 hour at RT using 1% (w/v) sucrose, 5% (w/v) bovine serum albumin (BSA) in PBS. A standard curve was generated using serial dilutions of recombinant human GROα. Standards and samples (100 μl) were incubated for 2 hours at RT. 100 μl biotinylated anti-human GROα (200 ng/ml) was added to each well and incubated for a further 2 hours at RT. The plates were then incubated with streptavidin-horseradish peroxidase for 20 minutes and the colour developed by the addition of 3,3`,5,5`-tetramethylbenzidine for 30 minutes. The reaction was stopped using 1 M H2SO4 and absorbance measured at 450 nm. Unknown samples were determined from the standard curve by interpolation. The lower limit of detection of the assay was 39 pg/ml. The assay was linearly affected by DTT, therefore for sputum measurements all standards were prepared using the equivalent concentration of DTT.
Measurement of MCP-1
MCP-1 was measured using an ELISA in essentially the same manner as GROα. The coating antibody was monoclonal anti-human MCP-1 (2 μg/ml). The detection antibody was biotinylated antihuman MCP-1 antibody (200 ng/ml). The lower limit of detection of this assay was 16 pg/ml. Since BAL fluid samples contained very low levels of MCP-1, all samples were concentrated fivefold using Microcon YM-3 filters (3000 molecular weight cut off) before analysis. As for the measurement of GROα in sputum, this assay was also linearly affected by DTT so for sputum analysis all standards were prepared using the equivalent concentration of DTT.
Statistical analysis
Significant differences were assessed by Kruskal-Wallis analysis followed by Dunn's post test for ANOVA analysis. Where relevant, Mann-Whitney t tests were performed. Correlation coefficients were obtained using Spearman's rank correlation; p values of 0.05 were considered significant.
RESULTS
Characteristics of subjects
The characteristics of the three subject groups are shown in table 1. FEV1 % predicted and FEV1:FVC ratio were significantly lower in patients with COPD than in non-smokers and healthy smokers.
Demographic data of subjects
BAL fluid cell counts
Differential cell counts of BAL fluid are shown in table 2. Significantly less BAL fluid was recovered from patients with COPD than from healthy smokers. A significantly higher number of inflammatory cells was recovered per ml BAL fluid from patients with COPD than from non-smokers and healthy smokers, but no difference was observed between the latter two groups. This was reflected by significantly more neutrophils and macrophages recovered per ml BAL fluid from COPD patients than from non-smokers and healthy smokers. A significantly higher percentage of neutrophils was recovered from non-smokers than from healthy smokers, but the number of neutrophils per ml BAL fluid recovered from the two groups did not differ. The percentage of macrophages recovered from the BAL fluid of healthy smokers was significantly higher than from non-smokers.
Differential and total cell counts in BAL fluid from non-smokers, healthy smokers, and patients with COPD
Induced sputum cell counts
Differential cell counts in induced sputum are shown in table 3. Significantly more inflammatory cells were recovered from the induced sputum of healthy smokers and patients with COPD than of non-smokers. Again, this was reflected by significantly more neutrophils in the induced sputum of both healthy smokers and COPD patients than of non-smokers. Furthermore, significantly more neutrophils were recovered from the induced sputum of patients with COPD than from healthy smokers. Similarly, significantly more macrophages were recovered from the induced sputum of patients with COPD than from non-smokers.
Differential and total cell counts in sputum from non-smokers, healthy smokers, and patients with COPD
GROα
GROα was detected in BAL fluid samples from non-smokers, healthy smokers, and patients with COPD with significantly less GROα in samples from healthy smokers than from non-smokers (1 (1) v 0.9 (0.4) v 2 (1) ng/ml, respectively, p<0.05; fig 1A). GROα was also detected in induced sputum samples from non-smokers, healthy smokers, and patients with COPD with significantly more GROα in samples from COPD patients than from non-smokers or healthy smokers (31 (11) v 2 (2) v 3 (0.5) ng/ml, respectively, p<0.05; fig 1B).

(A) Concentration of GROα in BAL fluid samples from non-smokers (n=14), healthy smokers (n=24) and patients with COPD (n=21). (B) Concentration of GROα in induced sputum samples from non-smokers (n=17), healthy smokers (n=12) and patients with COPD (n=16). *p<0.05, **p<0.01. Horizontal bars indicate median values.
MCP-1
MCP-1 was detected in BAL fluid samples from non-smokers, healthy smokers, and patients with COPD, but there was no difference in the levels of MCP-1 detected in samples from the three subject groups (26 (9) v 22 (7) v 32 (6) pg/ml; fig 2A). MCP-1 was also present in induced sputum samples from non-smokers, healthy smokers, and patients with COPD, with significantly more MCP-1 in samples from COPD patients than from non-smokers or healthy smokers (0.8 (0.4) v 0.2 (0.1) v 0.1 (0.04) ng/ml, respectively, p<0.05; fig 2B).
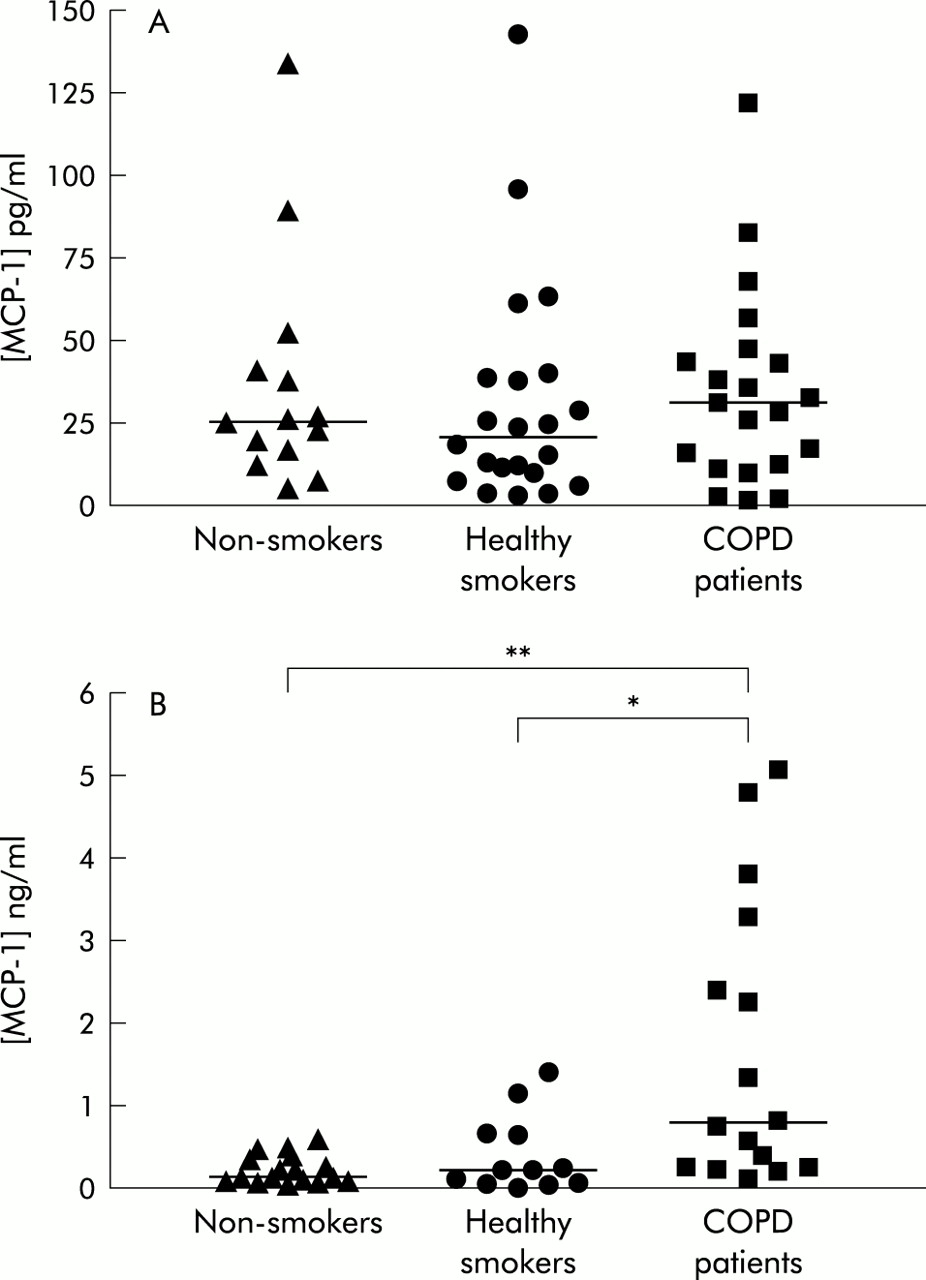
(A) Concentration of MCP-1 in BAL fluid samples from non-smokers (n=14), healthy smokers (n=22) and patients with COPD (n=21). (B) Concentration of MCP-1 in induced sputum samples from non-smokers (n=17), healthy smokers (n=12), and patients with COPD (n=16). *p<0.05, **p<0.01. Horizontal bars indicate median values.
Correlations between GROα levels and FEV1, neutrophils, and macrophages
Since GROα is known to be chemotactic for inflammatory cells,7,9 the relationship between this chemokine and inflammatory indices in the airway was examined. There was no correlation between GROα levels in BAL fluid and FEV1 % predicted, neutrophil or macrophage numbers recovered from BAL fluid. There was a significant negative correlation between GROα levels in induced sputum and FEV1 % predicted (r=–0.5, p<0.001; fig 3A). There was also a significant positive correlation between GROα levels in induced sputum and neutrophil numbers (r=0.6, p<0.001; fig 3B), but not with macrophage numbers. However, these correlations were not maintained within the COPD patient group alone.
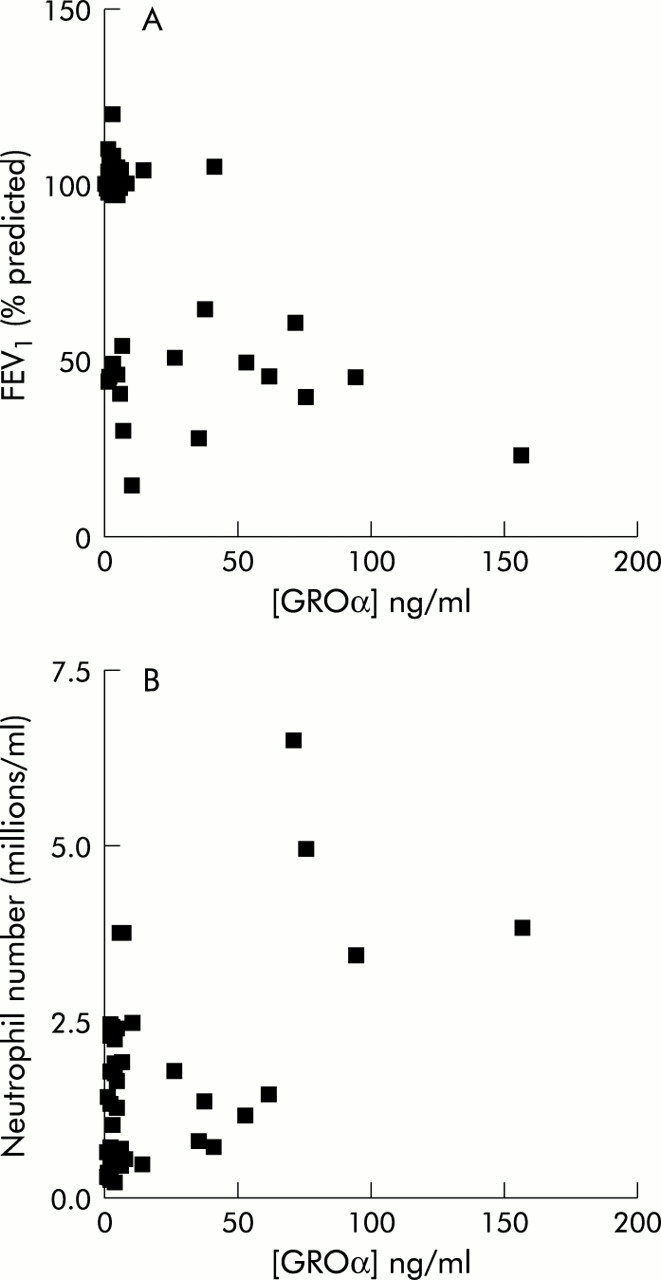
Correlation between concentration of GROα in induced sputum and (A) FEV1 % predicted (n=45, r=–0.5, p<0.001) and (B) neutrophil number (n=45, r=0.6, p<0.001) from the induced sputum of non-smokers, healthy smokers, and patients with COPD.
Correlations between MCP-1 levels and FEV1, neutrophils, and macrophages
There was no correlation between MCP-1 levels in BAL fluid and FEV1 % predicted, neutrophil or macrophage numbers. However, there was a significant negative correlation between MCP-1 levels in induced sputum and FEV1 % predicted (r=–0.5, p<0.001; fig 4A). Again, there was a significant positive correlation between MCP-1 levels in induced sputum and neutrophil numbers (r=0.4, p<0.01; fig 4B), but not with macrophage numbers. These correlations were not maintained within the COPD patient group alone.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between concentration of MCP-1 in induced sputum and (A) FEV1 % predicted (n=45, r=–0.5, p<0.001) and (B) neutrophil number (n=45, r=0.4, p<0.01) from the induced sputum of non-smokers, healthy smokers, and patients with COPD.
DISCUSSION
Airway inflammation in patients with COPD is associated with increased numbers of neutrophils and macrophages which contribute to the inflammatory process. GROα is a CXC chemokine which exerts its effects via CXCR2 receptors on neutrophils and monocytes, and MCP-1 is a CC chemokine which exerts its effects via CCR2 receptors on monocytes and T and B lymphocytes.13 The presence of these chemokines in the airways of patients with COPD therefore suggests that they could play an important role in the recruitment and activation of inflammatory cells in the airways of patients with COPD.
This study compares, for the first time, the presence of GROα and MCP-1 in BAL fluid and induced sputum samples from non-smokers, healthy smokers, and patients with COPD. Patients with COPD expressed significantly higher concentrations of GROα and MCP-1 in induced sputum but not in BAL fluid than non-smokers and healthy smokers. One possibility for this observation is that the healthy smokers and non-smokers are younger than the COPD group, although there is overlap in the age ranges. Spontaneous sputum production is a feature of COPD, but it is not always feasible to obtain samples of spontaneous sputum from patients for analysis. Induced sputum has been used as a model of spontaneous sputum production,14 and it has been reported that there are no differences between spontaneous and induced samples from patients with COPD when comparing total and differential cell counts.15 Induced sputum may therefore reflect some of the indices of inflammation in the upper airways (sixth generation of branching16) associated with COPD. This procedure is non-invasive, repeatable, and is well tolerated by patients with severe airflow limitation.17
Although increased levels of chemokines were found in induced sputum from patients with COPD, we found no difference in the levels of GROα and MCP-1 in BAL fluid but there was a significant increase in the levels of GROα in the BAL fluid from non-smokers compared with healthy smokers. Studies by Morrison et al18 examining the levels of GROα in BAL fluid from non-smokers and healthy smokers did not find a significant increase in GROα, even though the levels were higher for non-smokers than for healthy smokers. However, the levels of ENA-78, another neutrophil chemoattractant, were increased in the BAL fluid from non-smokers compared with healthy smokers. They did not find any differences between the levels of GROα in BAL fluid from chronic and acute smokers, which suggests that the immediate smoking history does not alter GROα levels in BAL fluid.18 The lack of a difference in the chemokine levels when comparing COPD patients with either non-smokers or healthy smokers might reflect the fact that BAL samples the lower respiratory tract.19 There are problems associated with the procedure for obtaining BAL fluid as it results in dilution of chemokines in the sample and often cannot be standardised because of clinical constraints.20 Significantly less BAL fluid was recovered from patients with COPD than from healthy smokers, and this may reflect the fact that patients with COPD have increased lung permeability resulting in loss of the introduced fluid into the surrounding tissues and an increased leakage of soluble components from the blood capillaries and tissues into the alveolar epithelial lining fluid (ELF).20 These factors may also account for the lack of correlation between the concentrations of GROα or MCP-1 in BAL fluid and FEV1 % predicted or neutrophil and macrophage numbers. This may also be due to the fact that a significantly higher percentage of neutrophils was recovered from the BAL fluid of non-smokers than from healthy smokers, although this is unlikely to be the case as there was no difference in the number of neutrophils per ml BAL fluid recovered. The apparent discrepancy in the percentage of neutrophils recovered from the BAL fluid of non-smokers compared with healthy smokers might be a reflection of the sampling technique employed in this study. Alternatively, this may reflect the fact that the cohort of smokers recruited to the study had fewer pack years than other published studies.6,18
MCP-1 might be involved in the recruitment and activation of monocytes in the airways and, since it is increased in patients with COPD, this chemokine might have an important role in the recruitment of inflammatory cells in this disease. GROα is thought to be a neutrophil chemoattractant and is likely to be involved in the recruitment and activation of neutrophils in the airways of patients with COPD. Previous studies of another neutrophil chemoattractant (IL-8) in induced sputum also found increased levels in patients with COPD,17 although the levels of GROα found in the present study exceed those of IL-8 in previous studies (11–20 ng/ml).11,17 Both GROα and IL-8 might therefore be involved in the recruitment of other inflammatory cells including monocytes. The relationship between the chemokine levels and inflammatory cell recruitment is complex and is dependent upon the regulation and desensitisation of the specific chemokine receptors. Until these mechanisms are clarified, it is difficult to predict the relative importance of each chemokine in inflammatory cell recruitment.
This study showed a significant correlation between the concentrations of both GROα and MCP-1 in sputum and FEV1 % predicted, but there were no significant correlations with either GROα or MCP-1 in the COPD group alone. This may be due to the relatively small sample size of the COPD group and should be more fully addressed in a larger study. However, since GROα correlates with FEV1, and FEV1 relates to neutrophils, then GROα will also relate to neutrophil number. Nevertheless, the correlation between chemokine concentrations and airway obstruction indicates that, as airway obstruction in COPD progresses, the levels of these chemokines increase which may reflect increasing levels of underlying inflammation. These chemokines may be responsible for the increase in inflammatory cells in the airways. This is supported by a significant positive correlation between the concentrations of GROα and MCP-1 in induced sputum and neutrophil numbers. The correlation between MCP-1 and increased neutrophil numbers may reflect enhanced monocyte migration followed by secretion of the neutrophil chemoattractants IL-8 and GROα,7,21 as MCP-1 itself has not been reported to be a chemoattractant for neutrophils.22 However, no correlation was found between the concentrations of GROα and MCP-1 in induced sputum and macrophage numbers. This does not necessarily mean that MCP-1 does not have a role to play in recruiting cells into the lungs, but other chemokines present may contribute to cell recruitment. The lack of correlation might be due to recruitment of monocytes into the tissue where they differentiate into macrophages at the site of proteolytic tissue destruction. Examination of tissue macrophage numbers might therefore be a better corollary with MCP-1, but this is beyond the scope of this study.
Capelli et al6 reported that MCP-1 was increased in BAL fluid from patients with chronic bronchitis. This conflicts with this study, as MCP-1 was not found to be increased in the BAL fluid of patients with COPD. Furthermore, Capelli et al found that MCP-1 levels were raised in healthy smokers compared with non-smokers.6 The reason for the discrepancy between the present study and that of Capelli et al6 may be explained by different sampling techniques. In the present study the amount of saline used to obtain BAL fluid was 100 ml more than that used by Capelli et al.6 This apparent dilution of any MCP-1 in the airway may account for differences in the data. Chronic bronchitis is an important feature of COPD, but many patients with COPD suffer a wider range of symptoms and may not elicit mucus hypersecretion to the extent of that exhibited by patients with chronic bronchitis. The healthy smokers recruited to the study of Capelli et al6 had a higher average number of pack years than those in this study (42 (21) v 17 (2) pack years) which again may account for the discrepancies between the two studies.
In summary, the increased levels of chemokines in induced sputum would suggest an involvement of CXC (GROα) and CC (MCP-1) chemokines in the inflammatory processes associated with COPD. This hypothesis is further supported by increased levels of IL-8 in both the induced sputum from healthy smokers and COPD patients17 and the BAL fluid of patients with COPD.23 These chemokines are therefore likely to be involved in the migration of monocytes and neutrophils into the airway contributing to the increased inflammatory load associated with this disease.
Acknowledgments
This work was supported by grants from Boeringer Ingelheim, MRC (UK), British Lung Foundation and Pharmacia.