Article Text

Abstract
Background: The rising prevalence of asthma in developed nations may be associated with the rising prevalence of obesity in these same nations. The relationship between body mass index (BMI) and the development of an objective marker for asthma, methacholine airway hyperresponsiveness (AHR), was investigated in adult men.
Methods: Sixty one men who had no AHR at initial methacholine challenge testing but who developed AHR about 4 years later and 244 matched controls participated in the study. The effects of initial BMI and change in BMI on development of AHR were examined in conditional logistic regression models.
Results: Initial BMI was found to have a non-linear relationship with development of AHR. Compared with men with initial BMI in the middle quintile, men with BMI in the lowest quintile (BMI=19.8–24.3 kg/m2) and those with BMI in the highest quintile (BMI >29.4 kg/m2) were more likely to develop AHR: OR=7.0 (95% CI 1.8 to 27.7) and OR=10.0 (95% CI 2.6 to 37.9), respectively. These results remained significant after controlling for age, smoking, IgE level, and initial FEV1. In addition, there was a positive linear relationship between change in BMI over the period of observation and the subsequent development of AHR.
Conclusions: In this cohort of adult men, both a low BMI and a high BMI were associated with the development of AHR. For men with a low initial BMI the increased risk for development of AHR appears to be partly mediated by a gain in weight. The effect of BMI on AHR may suggest mechanisms in the observed associations between obesity and asthma.
- bronchial hyperresponsiveness
- asthma
- body mass index
- obesity
Statistics from Altmetric.com
It has been observed that the rising prevalence of asthma in developed nations has coincided with the rising prevalence of obesity. Cross sectional studies in children have found that obesity is more prevalent in asthmatic subjects than in non-asthmatic controls.1,2 A survey of 19 126 Dutch adults showed that women with a body mass index (BMI) of ≥30 kg/m2 had 1.8 times the risk for having asthma than leaner women.3 This relationship was not found among men. Because of the cross sectional nature of these studies, it is not known whether obesity confers risk for the development of asthma or whether asthmatics become obese after the onset of the disease.
A prospective analysis conducted in women participating in the Nurses' Health Study was the first to show a relationship between a high BMI and subsequent doctor's diagnosis of asthma.4 However, since this study used questionnaire data to ascertain an asthma diagnosis, there is scepticism about the results.5 In addition, potential mechanisms for the association of obesity and asthma remain speculative.
We therefore sought to investigate the relationship between BMI and the development of airway hyperresponsiveness (AHR) to methacholine, a central and objective feature of asthma, in men participating in a longitudinal study of aging.
METHODS
Population
The Normative Aging Study is a longitudinal study of aging established by the Veterans Administration in 1961.6 The initial cohort of study subjects consisted of 2280 community dwelling men from the Greater Boston area who were 21–80 years of age at the time of entry into the study between 1961 and 1969.
Since entry, volunteers have reported for periodic examinations, each consisting of a uniform medical history and physical examination, together with blood and urine tests and spirometric tests. Beginning in 1984, subjects have also been studied with a detailed respiratory symptom and smoking questionnaire, methacholine challenge test, allergy skin tests, and serum IgE measurements. Internal evaluations have shown that, since its inception, the Normative Aging Study has incurred an attrition rate from all causes of <1% annually. Although the men participating in the Normative Aging Study are predominantly white, analyses performed in 1988–90 showed that the educational status and causes of death appear representative of the US population.
Participation in this study was approved by the Human Studies Subcommittee of the Research and Development Committee, VA Medical Center, Boston, Massachusetts. Written informed consent was obtained from all subjects.
Definition of cases and controls
Cases and controls were selected from participants who returned for their regularly scheduled examinations between May 1984 and November 1991 , and had at least two examinations with methacholine challenge test data during that time period. A subject was designated a case if he had a negative response at the initial methacholine challenge test but had a positive response (defined below) at the follow up examination. Controls were selected from those who had negative responses to methacholine challenge test at the initial and follow up examinations. Four controls were matched to each case according to the date of the first examination of cases.
Body mass index (BMI)
Weight and height of each subject were measured at each periodic examination as previously described7 and the BMI (weight in kilograms divided by the square of height in metres) was calculated for each subject. The BMI taken at the first examination was labelled the initial BMI. The change in BMI per year was calculated as the follow up BMI minus the initial BMI divided by the number of years between examinations.
Questionnaire data
Information on smoking habits was obtained from standard questionnaires based on the American Thoracic Society DLD-78 questionnaire.8 Current smokers, former smokers, and never smokers were identified based on their responses to the questionnaire. The number of pack years smoked was calculated from the information in the questionnaires.
Spirometric testing and methacholine challenge protocol
Spirometric and methacholine challenge tests were performed as previously reported.9 Subjects underwent a methacholine challenge protocol adapted from that of Chatham and colleagues.10 Subjects were considered to have a positive methacholine challenge test (AHR) when the forced expiratory volume in 1 second (FEV1) declined by 20% from the postsaline value at or before one inhalation of 25 mg/ml methacholine (equivalent to a cumulative dose of 16.8 μmol methacholine based on previous determination of nebuliser output by weight9). Subjects were defined as having a negative methacholine challenge test if no such decline occurred. Sixty one men were identified as cases (negative methacholine challenge test at the initial examination but a positive test at the next examination), 32 of whom (52.5%) had a 20% decline in FEV1 from the postsaline value at or before four inhalations of 5 mg/ml methacholine (equivalent to a cumulative dose of 8.58 μmol methacholine).
Statistical analysis
Univariate relationships between dependent and independent variables were explored using t tests for normally distributed variables, non-parametric Wilcoxon rank sum test for skewed variables, and χ2 tests for categorical variables. To deal with the matching of cases and controls, univariate and multivariable conditional logistic regression models were created using the NLIN procedure in SAS.11 All analyses were performed with the SAS statistical software package (SAS Institute Inc, Cary, NC, USA).
RESULTS
Sixty one men were identified with a negative initial methacholine challenge test and a positive methacholine challenge test (AHR) on subsequent testing. Two hundred and forty four controls who had negative methacholine challenge tests both at the initial and follow up examinations were matched to the cases on the basis of the date of the initial examination. The mean time between initial and follow up examinations did not differ between cases and controls (mean (SD) 3.78 (1.63) years and 3.72 (1.53) years, respectively; p>0.05). Baseline characteristics of the study subjects are shown in table 1. Cases had lower initial lung function and higher initial BMI than controls. The prevalence (current smokers) and intensity (in pack years) of smoking was greater in cases than in controls, although these differences were not statistically significant.
Baseline characteristics of study subjects
Table 2 shows the results of univariate and multivariable conditional logistic regression models evaluating the relationship between initial BMI and incident AHR. This relationship is non-linear, with the lowest and highest quintiles representing the greatest risk for AHR compared with the middle quintile. This relationship was maintained even after controlling for age, smoking (both prevalence and intensity), log10 IgE (log transformed serum IgE levels), and initial FEV1 values. We considered whether the association between initial BMI and development of AHR could be mediated by level of lung function. As shown in table 3, there were no statistically significant differences in percentage predicted values of either FEV1 or forced vital capacity (FVC) between quintiles of BMI in cases or controls. In fact, cases in the lowest quintile of initial BMI had somewhat higher lung function than those in the second, third, and fifth quintiles.
Conditional logistic regression models for the association between initial BMI and incident AHR
Pulmonary function according to quintiles of initial BMI
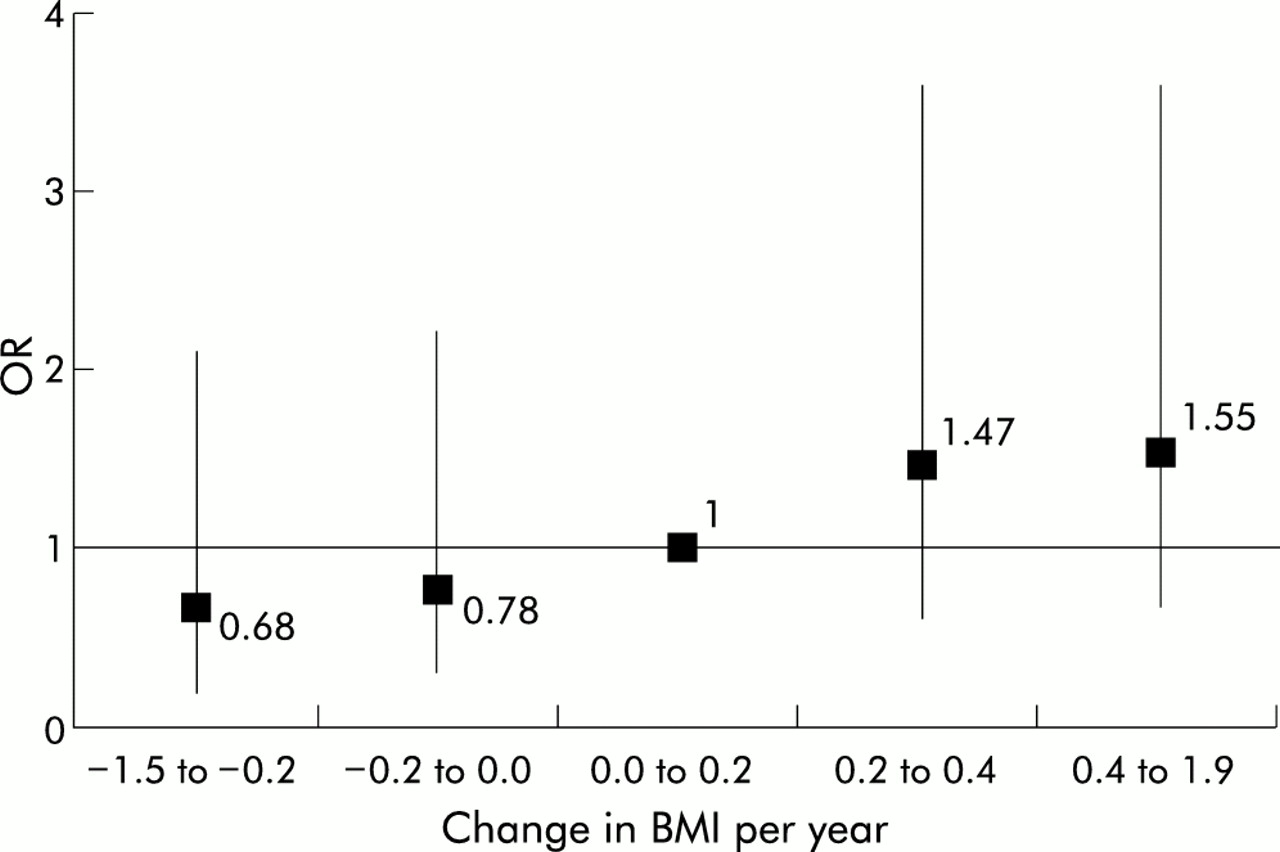
Figure 1 shows the relationship between the mean change in BMI/year (in quintiles) and incident AHR. Although not one of the changes in BMI/year quintiles was statistically significant on its own compared with the third quintile (change in BMI/year=0.0–0.2), the relationship was strongly positive and linear. Incorporating a categorical variable for quintiles of change in BMI/year in the model as a test for a linear trend was statistically significant (p=0.02), so there was increasing risk for AHR with increasing BMI. These results were unchanged when adjusted for age, baseline BMI, smoking, log10 IgE, and initial FEV1 values.
{kind=link}
Odds ratios from a conditional logistic regression model for the association between change in body mass index (BMI) per year (in quintiles) with development of airway hyperresponsiveness (AHR).
Table 4 shows the relationship between initial BMI and change in BMI. For all quintiles except the middle quintile, cases gained more weight than controls. Among the cases, those in the lowest quintile of baseline BMI had the greatest gain in weight per year (0.34 BMI units per year) during the period of observation.
Mean (SD) change in BMI per year in cases and controls by quintiles of baseline BMI
All the analyses were repeated using the stricter definition of AHR (a positive response at a cumulative dose of 8.58 μmol methacholine) and similar results were obtained.
DISCUSSION
The results of our analyses show a significant association between initial BMI, measured about 3.74 years earlier, and the development of methacholine AHR in older adult men. Our results also suggest that weight gain over this same time interval may be associated with an increased risk for the development of methacholine AHR, and this weight gain among cases in the lowest quintile of initial BMI may partly explain the increased risk associated with having a low BMI.
Over the past few years there have been increasing numbers of reports documenting the relationship between obesity and asthma across several age groups. In children the prevalence of asthma1,2,12 and wheeze12 were found to be greater in children who are overweight and obese. In adults two studies have found a relationship between obesity and reported asthma in women, but these studies did not find a significant relationship in men. The first study was a survey of 19 126 Dutch adults ranging in age from 20 years to over 65 years.3 Severely overweight women (BMI ≥30) were found to be 1.8 times more likely than women in the reference category (BMI=20.0–24.9) to have asthma. A second study was performed on 8960 adults aged 26 years who were part of the 1970 British Cohort Study13 and an increasing risk for asthma was observed for each quintile of BMI compared with the lowest quintile in women. Although the investigators observed an increased risk for asthma in the highest quintile in the men, this was not statistically significant. Because of the cross sectional nature of these studies, it is difficult to say whether obesity increases the risk for asthma or whether subjects became obese after their asthma became active. The relationship between obesity and asthma was investigated in a prospective analysis among nurses participating in the Nurses Health Study.4 The risk for incident asthma over the 4 year follow up period increased in a linear fashion with increasing BMI measured at the start of follow up, and subjects who gained weight after the age of 18 were at increased risk for developing asthma. However, the limitation of these clinical and epidemiological studies remains the difficulty in objectively measuring asthma.5
An alternative to defining asthma is to use an associated objective marker such as AHR. Studies in children and adolescents have shown that both obese asthmatic14 and obese non-asthmatic14,15 subjects have greater degrees of exercise induced bronchospasm than their non-obese counterparts. To date, no other studies have investigated this phenotype in adults.
We found a U-shaped relationship between baseline BMI and the development of methacholine AHR. Our results are consistent with a previous Italian survey that investigated BMI and the prevalence of chronic diseases. Using data on 72 284 individuals aged 15 or over from the 1983 Italian National Health Survey, Negri et al16 found that men with BMI <20 kg/m2 had an associated relative risk for asthma of 1.42 (95% CI 1.15 to 1.76) compared with men with BMI of 20–24.9 kg/m2. The risk was also increased for men with BMI ≥30 kg/m2 (RR 1.70, 95% CI 1.42 to 2.02). For women the association between BMI and asthma was more linear, consistent with previous findings among women. Interestingly, for both men and women in this study the association between BMI and emphysema or respiratory insufficiency was also found to be U-shaped. Nutritional factors may play a role in the risk for AHR and obstructive airway disease among those with a low BMI. In animal models, protein and calorie restriction during the prenatal and early postnatal periods can result in permanent abnormalities in lung structure and function, including emphysema-like lesions.17,18 In humans, experiments on volunteers showed a negative effect of starvation on various indices of ventilatory function.19,20 AHR was not measured in these early studies, and we are not aware of any other study which has reported an association between low BMI and AHR. Although we are quite certain that none of the men in our study was on a starvation diet, it may be that undernourishment in itself could have an effect on respiratory function. However, based on this analysis, at least part of the risk for development of AHR in the low BMI category appears to have been mediated by a gain in weight, as seen in table 4. Cases in the low BMI category had the greatest rate of change of BMI of 0.34/year. However, since the mean BMI in this category was 23.1, obesity per se would not explain all of this risk since subjects in this category would have ended up with a mean BMI still within the normal range.
We considered whether the men in our study with a BMI in the lowest quintile had COPD or poor lung function. The data presented in table 3, however, suggest that this is not the case since respiratory function among men in the lowest quintile was as good as or even better than those in the middle quintiles. Thus, we hypothesise that the mechanism(s) for the development of AHR in lean men may be different from the mechanisms occurring in obese men, leading to a non-linear association. This non-linear association between BMI and AHR in men may be one reason why many studies have found associations between BMI and asthma in women but not in men.
Our results also suggest that weight gain may be associated with an increased risk for development of AHR. Various mechanisms have been proposed to explain the association between weight gain and AHR and/or asthma. Weight gain resulting in obesity has been shown to result in reductions in lung volumes21 resulting in decreased airway calibre, which is a known factor in AHR.22 As a further mechanical consequence of obesity, breathing at lower tidal volumes leads to greater contractile responses of airway smooth muscle.23 The argument has also been made that obesity is a marker for decreased physical activity, a sedentary lifestyle and spending more time indoors,4,24 resulting in greater exposure to indoor allergens. Another plausible link could be with diet, especially with recent data suggesting that an increase in dietary fat may be associated with both AHR25 and asthma.26 There is emerging recognition that systemic inflammation occurs in the obese state, as evidenced by increased levels in the circulation of acute phase reactants27 and of proinflammatory cytokines.28,29 These proinflammatory cytokines are known to contribute to airway inflammation in asthma30 and provide a possible mechanism by which obesity may predispose to AHR or asthma. Additionally, the finding that leptin, the protein of the putative OB gene, upregulates inflammatory immune responses in a murine model31 strengthens the plausibility of this hypothesis. Whether or not significant inflammation occurs in formerly lean individuals who gain some weight is not known. Other potential mechanisms include autonomic pathways32,33 which may be common to both obesity and asthma, and genetic factors such as β2 adrenergic receptor polymorphisms34,35 that may predispose an individual to have both conditions. More studies are needed to clarify the mechanisms involved in this association.
Several limitations are recognised in this study. The number of cases that we were able to identify was relatively small. However, despite this, we were able to detect significant effects of BMI on the development of AHR. We also recognise that there may be variability in the response to methacholine, and going from a negative test to a positive test at a cumulative dose of 16.8 μmol methacholine may be part of this variability. However, restricting the analysis to a stricter definition of a positive test (cumulative dose of 8.58 μmol methacholine) yielded similar results. Another limitation was the fact that the second measurements of BMI and methacholine AHR occurred at the same examination at the end of the time interval of interest. Thus, for the cases the onset of AHR may have occurred at any time during the interval and may have preceded weight gain. Because of the relatively short time interval between observations, however, we feel that, for most of the cases, the onset of AHR occurred close to the time of the second examination. In addition, since no measures of physical activity or diet were used, we are unable to comment on the role of these exposures in the current analysis. The participants in our study were all middle aged to older white men with adult onset AHR; our findings may not be generalisable to younger men or to those of non-white ethnic origin.
In conclusion, we have shown that baseline BMI is associated with development of methacholine AHR in older men and that this association is non-linear. This finding may be one reason why previous studies, while finding linear associations between BMI and asthma in women, have not found significant associations between obesity and asthma in men. We have also shown a strong positive linear relationship between weight gain over the period of observation and development of AHR.
REFERENCES
Footnotes
-
Grant support: KO8-HL03870 from the National Institutes of Health; HL34645 and HL03870 from the National Heart, Lung, and Blood Institute.
-
Dr Litonjua is a recipient of an American Lung Association Research Grant RG-024-N.
-
Dr Sparrow is a Research Career Scientist of the Medical Research Service of the Department of Veterans Affairs.
-
The Normative Aging Study is supported by the Cooperative Studies Program/ERIC of the US Department of Veterans Affairs and is a component of the Massachusetts Veterans Epidemiology Research and Information Center (MAVERIC).