Article Text

Abstract
Background: Aspirin intolerant asthma (AIA) is a clinically distinct syndrome characterised by the precipitation of asthma attacks following the ingestion of aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs). The prevalence of AIA among Australian asthmatic patients has not previously been reported.
Methods: Three populations were surveyed to establish the prevalence of AIA among Australian asthmatics. Two surveys were completed in patients recruited from the metropolitan area in Perth, Western Australia, one comprising 150 recruited from hospital based sources (hospital cohort) and the second comprising 366 from the membership of the Asthma Foundation of Western Australia (Asthma Foundation cohort). In a third study 1298 individuals were randomly selected from the rural community of Busselton in Western Australia.
Results: The prevalence of AIA in the hospital and Asthma Foundation cohorts was found to be 10.7% and 10.4%, respectively. Univariate analyses in the Asthma Foundation cohort indicated that AIA was associated with more severe asthma (OR = 2.4, 95% CI 1.18 to 4.86), nasal polyposis (OR=3.19, 95% CI 1.52 to 6.68), atopy (OR=2.96, 95% CI 1.48 to 5.89), sulfite sensitivity (OR=3.97, 95% CI 1.87 to 8.41), and sensitivity to wine (OR=3.27, 95% CI 1.65 to 6.47). Multivariate analyses indicated that atopy (OR=2.80, 95% CI 1.38 to 5.70), nasal polyposis (OR=3.39, 95% CI 1.57 to 7.29), and the number of asthma attacks in the previous 12 months (OR=1.20, 95% CI 1.02 to 1.42) were independent predictors for AIA, as was wine sensitivity (OR=2.20, 95% CI 1.02 to 4.72). The prevalence of AIA among asthmatic patients in the Busselton cohort was 10.9%. In addition, 2.5% of non-diagnosed asthmatics in this cohort reported asthma symptoms following aspirin ingestion.
Conclusion: The prevalence of respiratory symptoms triggered by aspirin/NSAID use was found to be 10–11% in patients with asthma and 2.5% in non-asthmatics. Aspirin sensitivity appears to be a significant problem in the community and further investigations of the mechanisms of these responses and the possible link between this syndrome and other food and chemical sensitivities are required.
- aspirin
- non-steroidal anti-inflammatory drugs
- asthma
Statistics from Altmetric.com
Aspirin intolerant asthma (AIA) is a clinically distinct syndrome characterised by the precipitation of asthma attacks following the ingestion of aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs).1 In most patients the symptoms first occur during the third or fourth decade of life and follow a characteristic course.2,3 Over several months chronic nasal congestion, anosmia, rhinorrhea and nasal polyps frequently develop. Bronchial asthma usually evolves next, after which aspirin and/or NSAIDs trigger acute asthma attacks. These attacks generally occur within an hour of aspirin ingestion and are typically accompanied by profuse rhinorrhoea, conjunctival irritation, and flushing of the head and neck.4 Importantly, sensitivity remains long term and the patient's asthma in these individuals runs a protracted course, despite avoidance of aspirin and NSAIDs.5
A limited number of worldwide studies have provided estimates of the prevalence of AIA that ranges from 1–2% up to 20%.6–9 The exact prevalence of AIA therefore remains uncertain. Much of this uncertainty appears to be attributable to variations in the method of diagnosis but, more critically, because of the different populations assessed. Although Australia has one of the highest reported prevalence rates for asthma in the world,10 there are no published data describing the prevalence of AIA in Australia. We report the prevalence and characteristics of AIA in two populations of Australian asthmatics using a detailed food allergy questionnaire which addresses food, food chemical, and drug sensitivities.11 We also report the prevalence of asthmatic responses to aspirin and NSAIDs in a third randomly selected rural Australian population using a second broader based asthma questionnaire. This population contained both asthmatic and non-asthmatic subjects.
METHODS
Subjects and study design
Food allergy questionnaire surveys
Two surveys reported in this paper relate to the administration of a previously designed food allergy questionnaire.11 In the first survey the questionnaire was administered to 150 diagnosed asthmatics recruited from Sir Charles Gairdner Hospital, Perth, Western Australia. Patients were recruited over 6 months and consisted of those who attended or were admitted to hospital for worsening asthma (35 patients) and those recruited from a hospital based asthma clinical trials unit (115 patients). Patients received the questionnaire together with a stamped self-addressed envelope for its return. Reminder phone calls were made at 2 and 4 weeks and questionnaires were accepted up to 6 weeks after the initial delivery.
In the second survey the food allergy questionnaire was mailed out to a random sample of 1500 members of the Asthma Foundation of Western Australia. The Asthma Foundation is a community based group which offers support and information to asthma patients in Western Australia. Responses were sought from those members who were doctor diagnosed asthmatics and over the age of 18. The questionnaire was used to select subjects and their responses were then analysed in detail. A reminder letter was posted to all non-responders 6 weeks after the initial mailing and responses were collected for an additional 6 weeks.
Rural population survey (Busselton)
Residents of the town of Busselton in the south west of Western Australia have been involved in a series of whole population health surveys since 1966. Surveying this population has involved the completion of a number of cross sectional studies using questionnaires, blood tests, and various medical assessments. In one such survey conducted in 1991 a screening questionnaire was posted to 9000 people on the voter registration rolls. A random selection was then asked to make one visit to the study centre to complete a self-administered questionnaire which included questions relating to the presence of sensitivities to aspirin and NSAIDs.
Questionnaire design
Food allergy questionnaire
The design of the questionnaire is described in detail elsewhere.11,12 Briefly, it collected demographic data and confirmed a medical diagnosis of asthma. Asthma characteristics were obtained, including duration of asthma, severity, atopic status, triggers, and current medications. The questionnaire also addressed sensitivities to alcoholic drinks, sulfite-containing foods, and aspirin and NSAIDs. An additional section of the questionnaire asked respondents about specific food and chemical triggers for asthma. Importantly, patients were only deemed to have positive sensitivity to alcohol, sulfites, or aspirin/NSAIDs if they reported two or more independent episodes of reactivity to these agents. In the section addressing sulfite sensitivity, respondents were asked about their reactivity to a panel of foods containing sulfite (specifically dried fruits and preserved vegetables),11 but were unaware of the purpose of this part of the questionnaire.
The section addressing aspirin/NSAID sensitivity provided a list of the major aspirin, aspirin-containing medicines, and NSAIDs on the market using both generic and trade names to help subjects identify relevant exposures. Respondents were questioned regarding the side effects triggered by these medicines and those specifically indicating asthmatic responses were questioned regarding the frequency, time of onset, duration, and severity of response.
Asthma severity in the food allergy questionnaire was assessed in a limited fashion by three separate questions collecting information on the respondent's asthma in the previous 12 months. The first of these addressed the number of attacks of asthma experienced, the second addressed the number of times a GP or specialist had been seen for active asthma symptoms, and the third involved a self-assessment of asthma severity. Scores were assigned for the responses to each of these questions. The number of asthma attacks in the last 12 months was given a score of 1 to 4 for between 0–1 and >7 attacks. Visits to the GP/specialist were similarly scored. Self-assessment of asthma severity was scored as follows: mild = 1, moderate =2, severe = 3, and very severe = 4. The three individual severity scores were averaged for each patient; a mean score of ≤2.5 was designated as “mild to moderate” asthma while a score of >2.5 was assigned as “severe to very severe” asthma. Atopic status in this questionnaire was assessed by individuals reporting the result of skin tests performed in the last 10 years.
Busselton questionnaire
The questionnaire administered to the randomly selected Busselton cohort included sections addressing demographics, respiratory symptoms, and aspects of the home environment. Also included were questions relating to occupationally related exposures to dust or fumes, smoking, respiratory illnesses, colds, allergies, other illnesses, and medication.13 Individuals were classified as asthmatic if they indicated the presence of wheeze in the previous 12 months and had a physician's diagnosis of asthma.14,15 In addition, all subjects received a modified histamine provocation test as described by Yan et al16 to help confirm the diagnosis of asthma. In the section addressing AIA, subjects were questioned as to whether they had consumed aspirin previously and whether they had ever experienced any “allergic” side effects associated with either aspirin and/or NSAIDs. Importantly, the number of questions relating to sensitivities to aspirin and NSAIDs was limited as this was part of a whole of health survey.
Data analysis
Simple descriptive statistics were used to generate mean values, percentage frequencies, and ranges. Fisher's exact tests were used to investigate associations between binary variables. Logistic regression analysis was used to analyse the association between AIA and variables relating to both demographic data and asthma disease status. A backward conditional stepwise protocol was used in multivariate analyses. A two sided p value of <0.05 was regarded as significant for all tests. Data were analysed using the SPSS software package.
Ethics
All three projects were approved by the Committee for Human Rights of the University of Western Australia and all subjects provided informed consent prior to participating.
RESULTS
Response rates and characteristics of subjects
Of the 1470 questionnaires delivered to members of the Asthma Foundation, 787 were returned (response rate 53.54%), of which 366 met the entry criteria and were analysed. A total of 5020 individuals responded to the screening questionnaire in the Busselton survey (response rate 55.78%). Of these, a random selection of 1298 (708 women) were assessed by self-administered questionnaire following attendance at the study centre. The demographic features of the three cohorts surveyed in this study are summarised in table 1. A more detailed characterisation of the features of asthma in individuals surveyed with the food allergy questionnaire was completed and is summarised in table 2.
Demographic and major outcome variables of surveyed populations
Selected asthma characteristics of the hospital and Asthma Foundation cohorts
Aspirin intolerant asthma
Food allergy questionnaire surveys
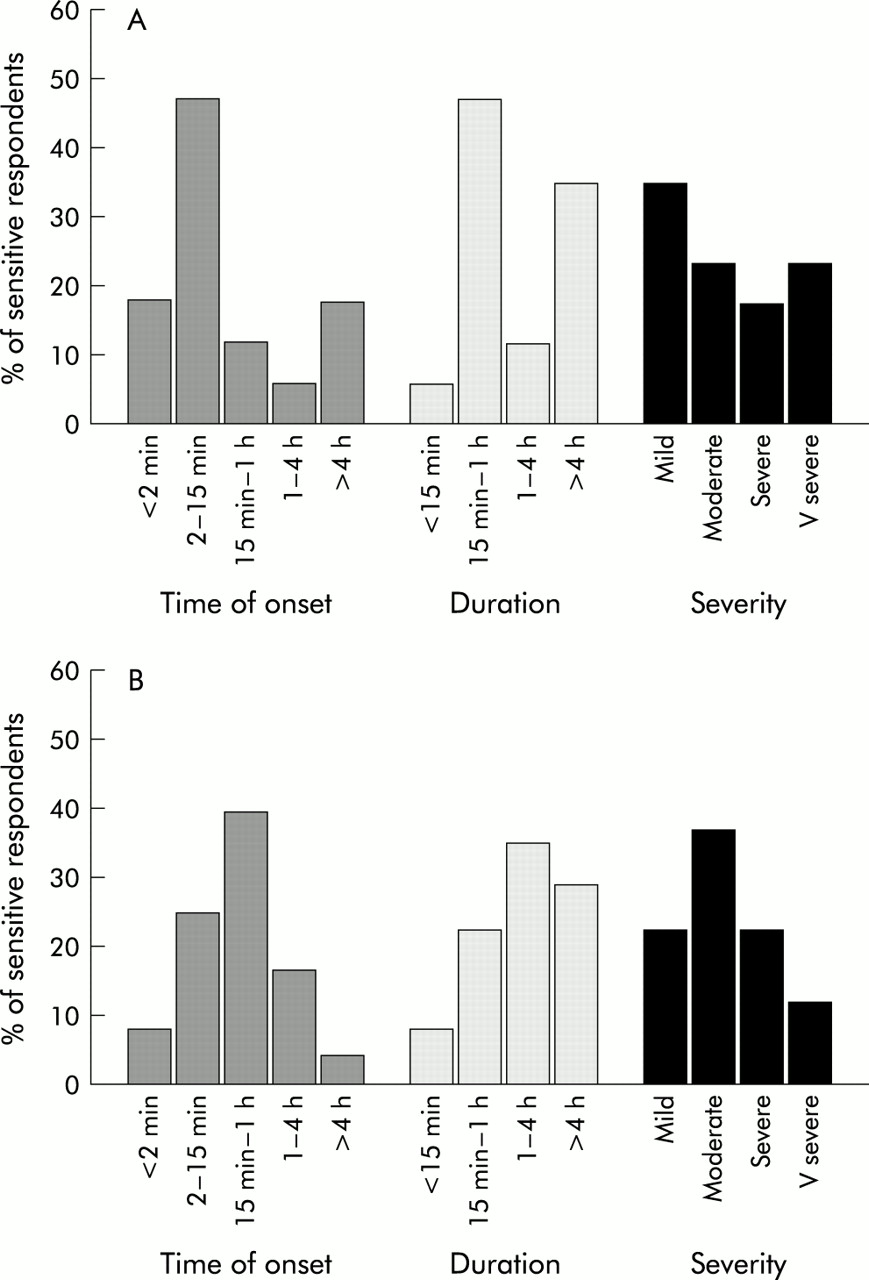
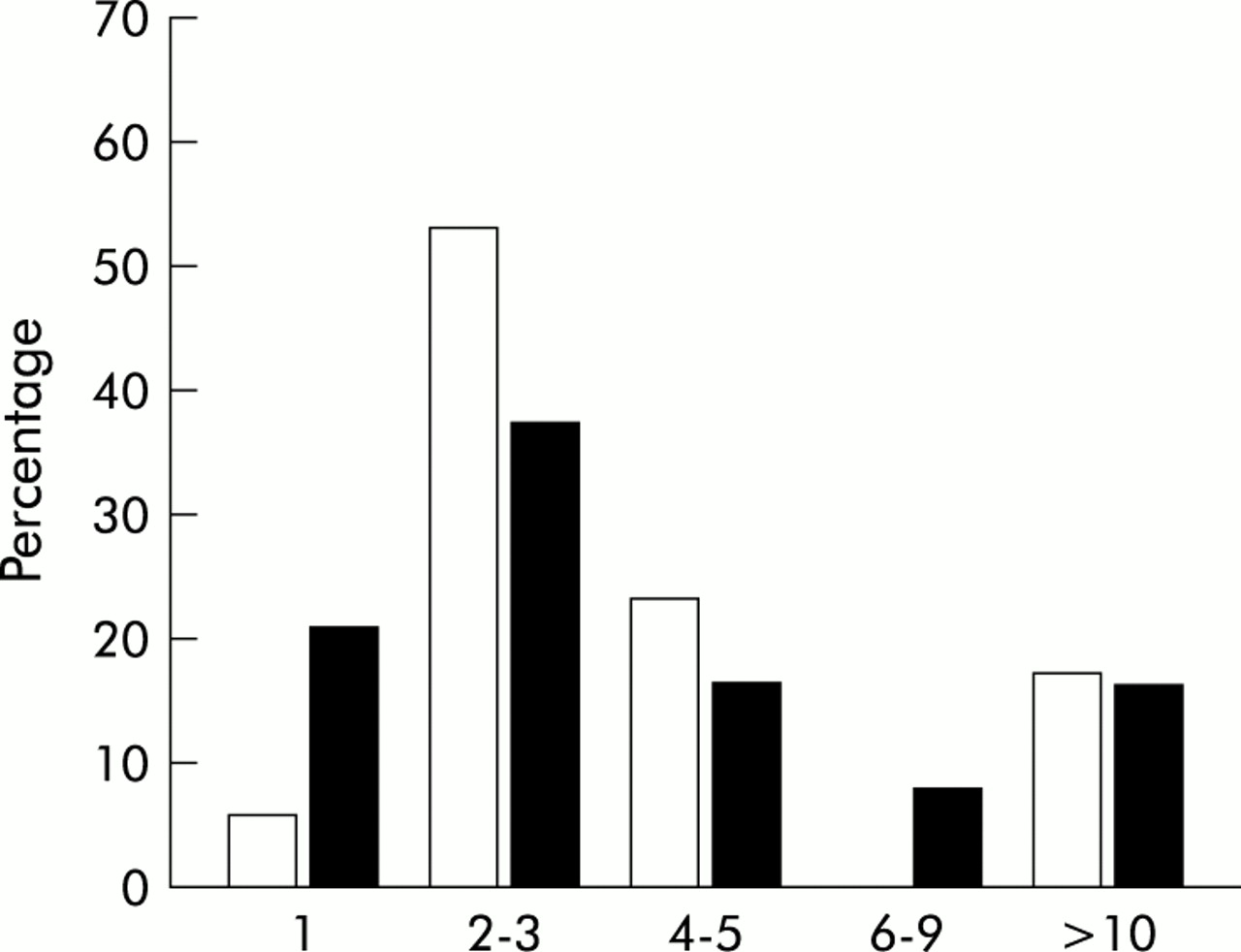
Major outcome measures relating to aspirin sensitivity in the hospital and Asthma Foundation cohorts are summarised in table 1. While a variety of side effects were associated with aspirin and NSAID ingestion, asthma was clearly the most commonly reported side effect (fig 1). The majority of aspirin sensitive asthmatics experienced three or fewer episodes of aspirin triggered asthma, although in both cohorts approximately 15% of respondents reported more than 10 previous episodes (fig 2). Using the preordained definition of AIA for the food allergy questionnaire (requiring at least two prior episodes of aspirin induced asthma), prevalence rates of 10.7% (n=16, 95% CI 5.8 to 15.6) and 10.4% (n=38, 95% CI 7.3 to 13.5) for this syndrome were observed in the hospital and Asthma Foundation cohorts respectively (table 1). Asthma triggered by aspirin and/or NSAIDs most commonly occurred within 1 hour of aspirin ingestion, and many individuals reported severe to very severe responses to these medicines (fig 3).
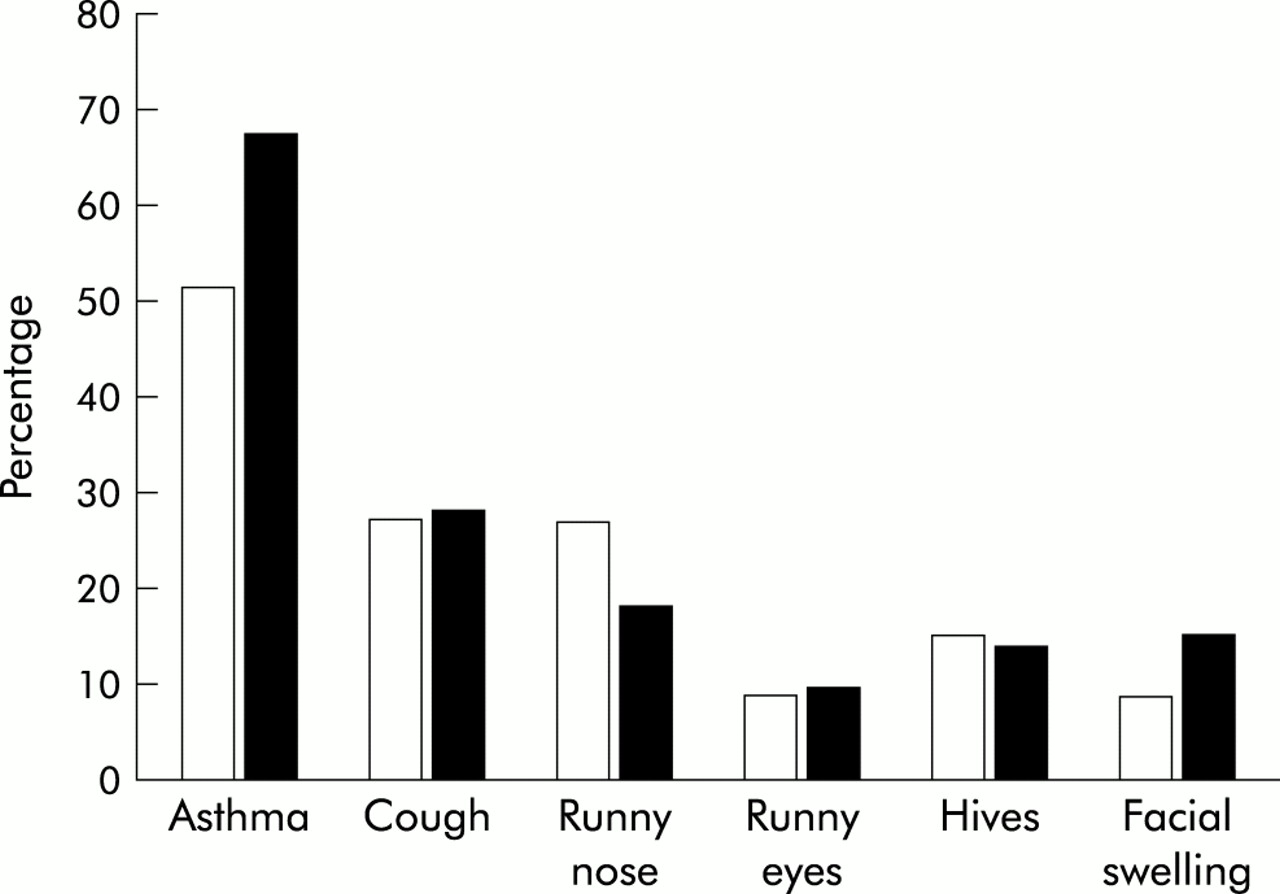
Percentage of asthmatics sensitive to aspirin who reported the triggering of specific allergic symptoms following the ingestion of aspirin and/or NSAIDs in the hospital (□) and Asthma Foundation (▪) cohorts

Distribution of the number of previous episodes of asthma triggered by aspirin among aspirin sensitive asthmatic patients in the hospital (□) and Asthma Foundation (▪) cohorts
{kind=link}
{kind=link}
{kind=link}
Characteristics of asthmatic responses among aspirin sensitive asthmatic patients in (A) the hospital cohort (n=17) and (B) the Asthma Foundation cohort (n=48).
Univariate analyses investigating the association between AIA and various parameters were completed in the larger Asthma Foundation cohort (table 3). Patients with aspirin intolerant asthma appeared to have more severe and unstable asthma than those who were aspirin tolerant, as assessed by a number of parameters including the number of asthma attacks, number of doctor visits, and self-rated asthma severity over the previous 12 months. Logistic regression analyses confirmed the association between AIA and nasal polyposis and atopy demonstrated in univariate analyses (table 4). In contrast, the number of asthma attacks in the previous 12 months was the only asthma severity parameter that remained in the logistic model and was predictive for the presence of AIA. After adjustment for the presence of nasal polyps, atopy, and the number of asthma attacks in the previous 12 months, wine sensitivity was confirmed to be a predictor for AIA, while sulfite sensitivity also appeared likely to be an independent predictor but just failed to meet the criteria for statistical significance (p=0.059).
Characteristics of respondents reporting asthmatic reactions to aspirin in the Asthma Foundation cohort
Results from multiple logistic regression analysis of aspirin intolerant asthma
Busselton survey
Of the 1298 individuals who completed the self-administered questionnaire, 1019 (78.5%) reported having previously consumed aspirin containing medicines. A total of 128 individuals (9.9%) in this cohort were diagnosed with asthma (table 1). Fifty individuals (3.9%) reported adverse reactions to aspirin. Ten of these had asthma and, of these, nine (7.0% of diagnosed asthmatics) reported respiratory symptoms following aspirin ingestion and were therefore classified as having AIA. Reactions to NSAIDs (in the absence of sensitivities to aspirin) were reported in 87 individuals (6.7% of the surveyed population), of whom 12 were asthmatic and five (3.9% of the diagnosed asthmatic population) reported respiratory symptoms and were therefore classified as having AIA. Allowing for those who reported asthmatic responses to both aspirin and NSAIDs, the prevalence of AIA among asthmatic patients in the Busselton cohort was 10.9% (95% CI 5.5 to 16.3). Interestingly, 13 of the 40 non-asthmatic individuals (1.1% of the non-asthmatic population) who indicated “allergic” reactions to aspirin reported the induction of respiratory symptoms suggesting the presence of an AIA like syndrome among subsets who were deemed non-asthmatic. Similarly, 16 of 75 non-asthmatic individuals (1.4%) who reported sensitivities to NSAIDs (in the absence of sensitivities to aspirin) reported respiratory symptoms, producing a combined prevalence of respiratory sensitivity to aspirin and NSAIDs among non-asthmatics of 2.5% (95% CI 1.6 to 3.4).
DISCUSSION
In three separate independent studies in which the assessment of the presence of AIA was based on a prior history of asthmatic responses to aspirin and/or NSAIDs we found that the prevalence of this syndrome was 10–11%. Two populations were recruited from the Perth metropolitan area in Western Australia and were surveyed using a food allergy questionnaire which addressed various food, food chemical, and drug sensitivities.11,12 In the third survey a truly random selection of individuals was recruited from the rural community of Busselton in Western Australia and administered a separate questionnaire which assessed a number of health related issues including the presence of sensitivities to aspirin and/or NSAIDs.
Other studies using similar criteria to assess the presence of AIA have reported prevalences of 3–9%.9,17–19 Our data suggest that the prevalence of AIA in Australia may be slightly higher than in North America and Europe. Interestingly, our estimates of the prevalence of AIA in the hospital and Asthma Foundation cohorts were very similar to estimates of the prevalence of AIA in the Busselton cohort, despite the obvious differences in patient selection and the fact that a different assessment tool was used. One would have expected the hospital and Asthma Foundation cohorts to have provided higher prevalence estimates since AIA has been associated with more severe asthma.20–22 Similarly, since there was a preponderance of women in the Asthma Foundation cohort and AIA has been reported to be more common in women,1,18,20,22 an increased estimate of the prevalence of AIA may have been expected. Importantly, other parameters which may have influenced the prevalence of AIA—such as the level of aspirin and NSAID exposure and the ages of respondents—were similar in all three cohorts.
Challenge studies suggest that the prevalence of AIA may be much higher than estimates based on history have indicated, and that it may be as high as 20%.6,8,23 One explanation for this disparity is recall bias, although a lack of significant exposure among many asthmatics is equally likely. We found that 20–25% of individuals in our studies had not consumed aspirin or NSAIDs previously, and thus it was impossible to ascertain whether a sensitivity to these medicines was present. Equally, reactions to these medicines may be subclinical and therefore aspirin and NSAIDs may not be recognised as specific triggers. The lack of recognition of aspirin/NSAID intolerances may have significant consequences for some individuals, since aspirin/NSAIDs may have a destabilising effect on asthma and, in some patients, have the potential to trigger severe or life threatening asthma attacks.24,25
In both univariate and multivariate analyses of the Asthma Foundation cohort nasal polyposis was found to be associated with AIA, which is in agreement with the well described aspirin triad.1 In this study the prevalence of nasal polyposis among those with AIA ranged from 31% to 34%, which is similar to that reported elsewhere.17–19 We also found a significant association between AIA and suspected atopy in this study. The significance of this association is unclear as sensitivities to aspirin and NSAIDs do not appear to be mediated through an immunological pathway, but rather through the shared pharmacological inhibition of cyclooxygenase.26 The exact relationship between the presence of atopy and AIA is unclear. Although early studies suggested that aspirin intolerance occurred less frequently in atopic individuals,1,7,17 more recent data are contradictory.22,27 The observed association between AIA and sensitivity to wine in this study may be explained by the presence of naturally occurring salicylates in these drinks; however, the capacity for natural salicylates in foods to trigger asthma has yet to be clearly established.28 Similarly, the significance of the possible association between AIA and sulfite sensitivity is unclear. Although aspirin intolerant and sulfite sensitive asthmatics appear to share some clinical features,29 there is little supportive evidence for cross sensitivity between aspirin and sulfites. It is possible, however, that a common pathophysiological abnormality exists in individuals sensitive to these agents.
Interestingly, several individuals in the Busselton cohort who were not diagnosed as asthmatic reported respiratory symptoms with aspirin and/or NSAID use. Overall, 2.5% of the non-asthmatics in this cohort reported respiratory symptoms such as difficulty in breathing or wheezing with aspirin or NSAIDs. The triggering of respiratory symptoms in these individuals is an important observation and requires further investigation. Presumably they only suffer asthmatic symptoms with aspirin and/or NSAIDs, subsequently avoid these medicines, and are then not considered to have asthma. Whether more chronic asthma symptoms develop in these individuals as time progresses is not known.
In summary, surveys of three separate populations suggest that the prevalence of AIA in Australia is 10–11%. In assessing the accuracy of the data generated, it is important to note that the estimates of AIA for each of our surveys were in close agreement and that response rates of more than 50% were achieved in the mailing surveys. Our estimate of the prevalence of AIA appears to be slightly higher than those reported in Europe and North America in which similar criteria for assessment have been used. However, the prevalence of AIA in Australia may be even higher than suggested by these surveys, and only the direct challenging of asthmatics with aspirin will ascertain if this is the case. The inhalation challenge method is a reliable and safe way to identify those individuals with AIA, and there is clearly a need for this to be performed more frequently.22 The identification of these asthmatics is important for a number of reasons, not least of which is the fact that AIA appears to represent a distinct asthma subtype characterised by more severe and persistent asthma, an increased reliance on corticosteroid therapy,22 as well as an increased production of leukotrienes,30 and thus may have important treatment implications. Further assessment of the clinical and laboratory features of AIA is likely to increase our understanding of the pathophysiology of asthma as well as factors that influence disease severity.
Acknowledgments
The authors thank Dr Richard Parsons, Mr Kieran McCaul, Dr Jenny Peat, Dr Geoffrey Stewart, Mr Wei Xuan, Mr John Spijker, Mr Rene van den Berg, Dr Neil Misso, Dr Alan James, Professor Ann Woolcock and both the Busselton Foundation of Western Australia and the Asthma Foundation of Western Australia for their assistance.