Article Text

Abstract
Background: As there is controversy about changes in lung function in primary pulmonary hypertension (PPH), lung mechanics were assessed with a focus on expiratory airflow in relation to pulmonary haemodynamics.
Methods: A cross sectional study was performed in 64 controls and 171 patients with PPH (117 women) of mean (SD) age 45 (13) years, pulmonary artery pressure (PAPmean) 57 (15) mm Hg, and pulmonary vascular resistance 1371 (644) dyne.s/cm5.
Results: Mean (SD) total lung capacity was similar in patients with PPH and controls (98 (12)% predicted v 102 (17)% predicted, mean difference –4 (95% confidence interval (CI) –7.89 to –0.11); residual volume (RV) was increased (118 (24)% predicted v 109 (27)% predicted, mean difference 9 (95% CI 1.86 to 16.14); and vital capacity (VC) was decreased (91 (16)% predicted v 102 (10)% predicted, mean difference –11 (95% CI 15.19 to –6.80). RV/TLC was increased (117 (27)% predicted v 97 (29)% predicted, mean difference 20 (95% CI 12.3 to 27.8)) and correlated with PAPmean (r=0.31, p<0.001). In patients with PAPmean above the median of 56 mm Hg, RV/TLC was further increased (125 (32)% predicted v 111 (22)% predicted, mean difference –14 (95% CI –22.2 to –5.8)). Expiratory flow-volume curves were reduced and curvilinear in patients with PPH.
Conclusions: Peripheral airway obstruction is common in PPH and is more pronounced in severe disease. This may contribute to symptoms. Reversibility of bronchodilation and relation to exercise capacity need further evaluation.
- pulmonary hypertension
- airway obstruction
- lung mechanics
Statistics from Altmetric.com
Primary pulmonary hypertension (PPH) is a rare and deleterious pulmonary vascular disease of unknown origin.1 The functional limitations of patients with PPH are mainly caused by progressive right heart failure and impaired pulmonary gas exchange. It is, however, unclear whether PPH may also be associated with changes in lung mechanics.
Considering the proximity of the pulmonary vasculature and the peripheral airways, it is possible that the latter may be affected either by mechanical encroachment of dilated vessels or by mediators of increased smooth muscle tone or proliferation.1,2 Experimental models of pulmonary hypertension induced by chronic hypoxia or monocrotaline indicate that structural changes in the pulmonary vasculature also extend to the airways, resulting in increased airways resistance.3,4 In humans, however, data on pulmonary function in PPH reported in small series of patients or case reports have been contradictory, with normal lung volumes,5 a restrictive ventilatory pattern,6–8 and airway obstruction9–11 being reported. In the national PPH registry in the USA a mild restrictive defect was found but no data on airflow were included.12
A cross sectional study was therefore designed to assess respiratory mechanics in a large well characterised European cohort of PPH patients recruited by the German PPH Study Group.11,13,14 Expiratory airflow limitation and premature airway closure were found to be common in patients with PPH compared with reference values and controls.
METHODS
One hundred and seventy one patients (117 women) with PPH15 were enrolled at eight centres after written informed consent was obtained and approval by the local ethics committees. Four patients were active smokers and 12 had smoked in the past. None of the patients was on bronchodilator treatment or had a history or signs of lung disease (chronic obstructive or interstitial lung disease, lung cancer, extensive tuberculosis). In 32% of the patients PPH treatment included iloprost inhalation. Patients with clinical or radiological signs of cardiopulmonary decompensation were not included. Since reported reference values for expiratory flow may vary substantially,16 64 non-smoking volunteers without pulmonary or cardiac dysfunction and matched for age and sex were included.
Lung function testing and haemodynamic measurements
Spirometric tests and body plethysmography (Erich Jaeger, MasterLabPro 4.2, Wuerzburg, Germany) were performed according to standard protocols.17 Lung function reference values corrected for sex, age, and height were used.17 Right heart catheterisation at rest was performed during the week before or after lung function testing, including measurement of cardiac output (CO) by the thermodilution method or the Fick principle.18
Statistical analysis
The data are presented as mean (SD) values. Data analysis consisted of the two tailed Student's t test, the two sample proportion test, or linear regression analysis using the least squares method.19 For subgroup analysis a split around the median value was used. A p value of <0.05 was considered significant.
RESULTS
The patient population did not differ significantly from the controls in sex (68% v 60% women), age (45 (13) v 46 (13) years), height (167 (10) v 170 (8) cm), or body weight (68 (14) v 71 (13) kg). Patients with PPH were classified according to the New York Heart Association (NYHA) functional classes II (23% of patients), III (61%), and IV (16%), mean 2.9 (0.6).
In PPH patients the mean pulmonary artery pressure (PAPmean) was increased to 57 (15) mm Hg (range 27–134), CO was reduced to 3.3 (1.2) l/min (range 1.4–8.2), and central venous pressure (CVP) was increased to 8 (5) mm Hg. The pulmonary capillary wedge pressure (PCWP) obtained in 151 patients was normal (7 (3) mm Hg) and the pulmonary vascular resistance (PVR) was increased to 1371 (644) dyne.s/cm5 (range 308–4250).
Total lung capacity (TLC) in patients with PPH (5.5 (1.2) l) was close to reference values and to controls (table 1). However, inspiratory vital capacity (VC, 3.4 (0.9) l) and forced expiratory volume in 1 second (FEV1, 2.5 (0.7) l) were reduced compared with predicted values and controls. Thus, there was moderate lung hyperinflation in PPH as indicated by an increase in residual volume (RV) and in the RV/TLC ratio (table 1). In control subjects TLC (6.0 (1.0) l), VC (4.0 (0.8) l), and FEV1 (3.4 (0.7) l) were close to reference values (table 1).
Mean (SD) values of lung function indices in 171 patients with PPH and 64 controls
In patients with PPH there were weak but significant linear correlations between the RV/TLC ratio, an index of lung hyperinflation, and the following parameters of airway obstruction: total airway resistance (Rtot; r=0.24; p=0.002), FEV1/VC (r=0.22; p=0.002), maximal expiratory flows at 50% and 75% of exhaled VC (MEF50: r=0.43, p<0.001; MEF25: r=0.32, p<0.001). For the PPH patients as a whole, Rtot did not differ significantly from reference values or from controls (table 1). However, increased Rtot values were found in a substantial proportion of patients with PPH with values of >0.36 kPa.s/l (>120% of reference value) in 49 patients (29%) and six controls (9%; p<0.001, two sample proportion test) and >0.45 kPa.s/l (>150%) in 23 patients (14%) and in none of the controls (p<0.001).
The FEV1/VC ratio in patients with PPH was significantly reduced compared with controls (table 1). Moreover, the prevalence of airway obstruction with an FEV1/VC ratio of <70% or <60% was significantly increased in patients with PPH (<70% in 37 patients (22%) and no controls, p<0.01; <60% in 10 patients and no controls, p<0.01).
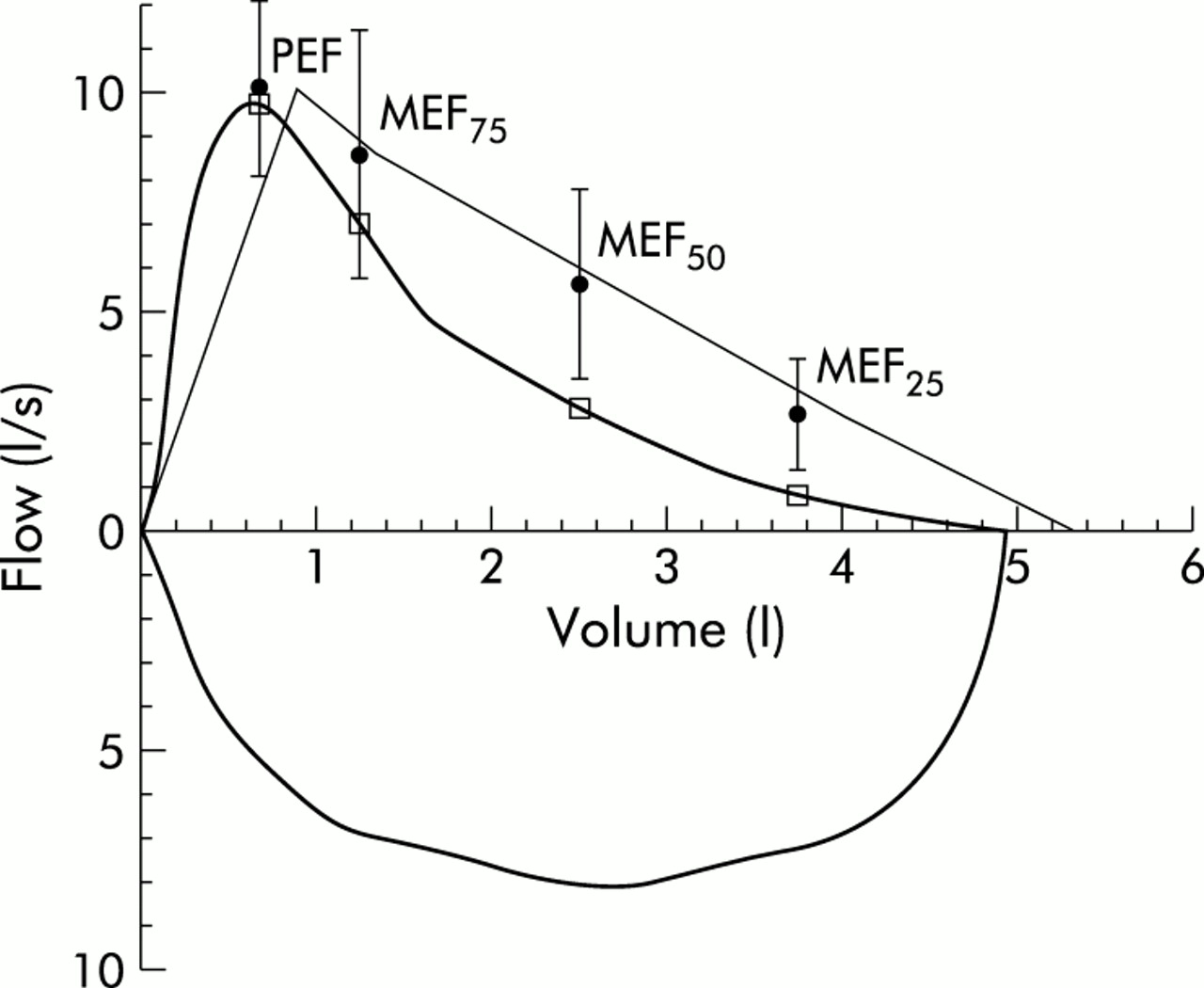
A representative example of the expiratory flow-volume curves with an abnormal curvilinear shape is shown in fig 1. Mean expiratory flow rates are shown in fig 2. A significant reduction in peak expiratory flow (PEF), MEF75, MEF50, and MEF25 was seen compared with predicted values (table 1) and control subjects (fig 2).

Flow-volume curve of a 27 year old non-smoking man with primary pulmonary hypertension (PPH, bold line). Predicted values (thin line) and predicted values corrected for individual vital capacity (dots ±2 SD) are also shown.
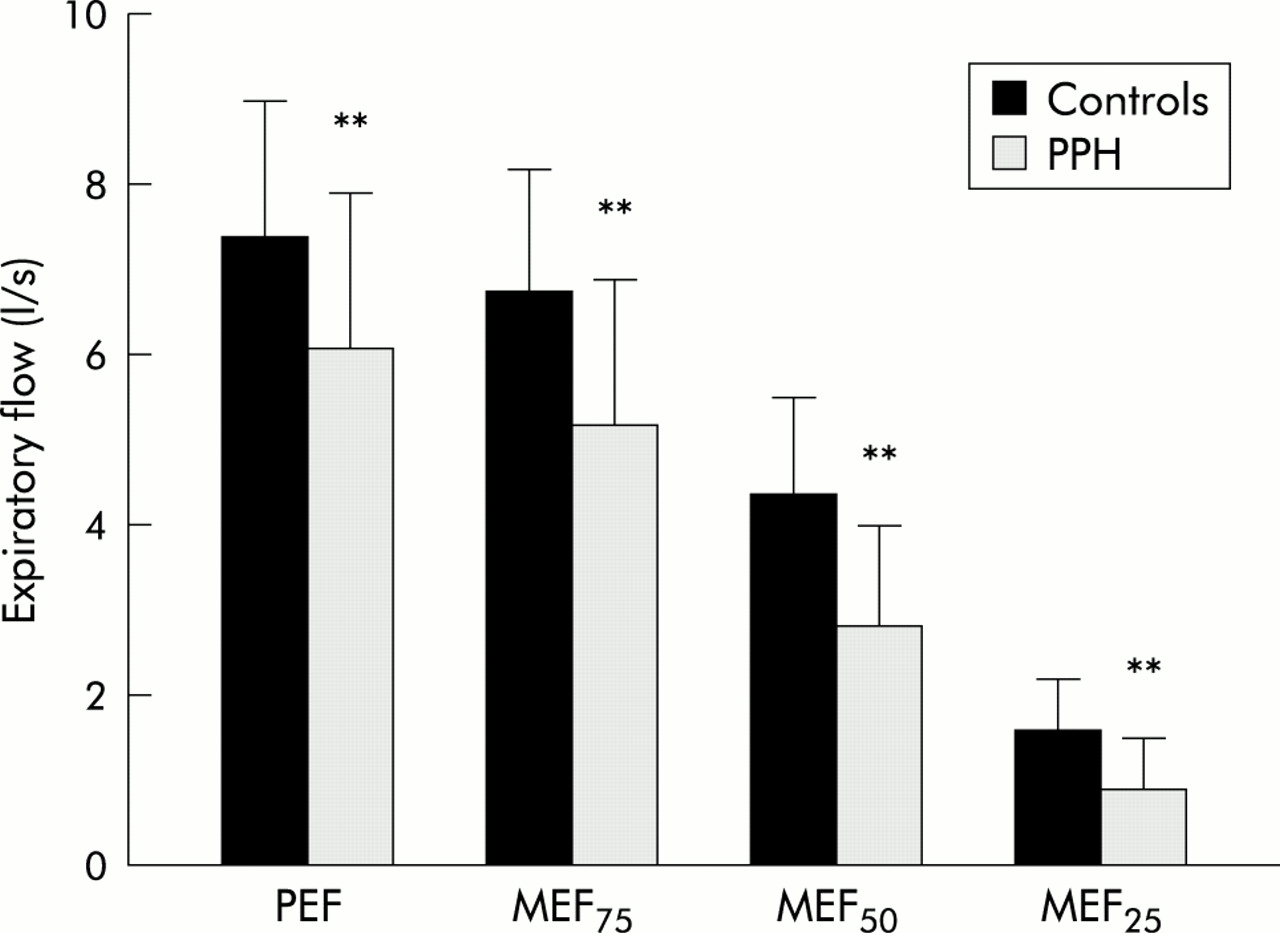
Expiratory airflow in 171 patients with PPH and 64 controls. Expiratory airflow was significantly decreased in PPH. The reduction in airflow was most prominent during the lower part of vital capacity (MEF50 and MEF25), indicating obstruction of peripheral airways in PPH. **p<0.01 v controls (Student's t test).
Airflow limitation was more pronounced at lower values of VC. MEF75, MEF50, and MEF25 were reduced by 18%, 34%, and 54%, respectively, from predicted values and by 11%, 37%, and 44% compared with controls (fig 2).
To account for the decreased VC in patients with PPH, flow rates were also corrected for individual VC values. The ratio of expiratory flow rates and remaining fractions of VC showed a similar highly significant reduction during end expiration (fig 3).

{kind=link}
{kind=link}
{kind=link}
To correct for differences in vital capacity (VC), a ratio of MEF75, MEF50, and MEF25 and the respective fraction of remaining VC, e.g. MEF75 × (0.75 × VC)−1 was calculated for 171 PPH patients and 64 controls. The progressive reduction in MEF during end expiration was independent of the reduced VC in patients with PPH. *p=0.04 and **p<0.001 v controls (Student's t test).
When patients were divided according to median PAPmean, RV/TLC was significantly higher in patients with a PAPmean above the median, but expiratory airflow parameters, Rtot, and FEV1/VC did not differ (table 2). Similarly, RV/TLC showed a weak linear correlation with PAPmean (r=0.31; p<0.001) whereas the other indices of lung function were independent of pulmonary haemodynamics (data not shown).
Mean (SD) lung function and haemodynamic indices in 171 patients with PPH subdivided into groups according to median mean pulmonary artery pressure (PAPmean)
Since smoking may affect small airways function, the 16 patients with PPH who had a smoking history were analysed separately. In this subgroup the results of right heart catheterisation, spirometric testing, and body plethysmography did not differ from the total patient population except for a reduction in RV/TLC (100 (31)% predicted, p=0.02 v total group) and MEF25 (33% predicted; p=0.03).
DISCUSSION
The main finding of this study was significant peripheral airway obstruction in patients with PPH as indicated by end expiratory airflow limitation and premature airway closure leading to a reduction in VC.
Previous studies, including the US PPH registry, failed to demonstrate airway obstruction in patients with PPH.5,12,20 Similarly, the frequently used criteria for airway obstruction (FEV1/VC <70%, Rtot >0.3 kPa.s/l) were not met by our patient group as a whole. However, the FEV1/VC ratio was significantly reduced in the patients with PPH compared with the controls. Moreover, the proportion of patients with an FEV1/VC ratio of <70% or <60% together with increased Rtot was significantly higher than in the control group. These findings indicate airway obstruction in PPH.
Since subtle changes in the airway characteristics may be missed by using only the FEV1/VC ratio or Rtot,9 flow-volume curves were used to analyse expiratory flow rates. Expiratory airflow was markedly decreased in patients with PPH, particularly during the effort independent end expiratory portion of the flow-volume curve obtained at lower values of VC. This resulted in a curvilinear curve, indicating peripheral airway obstruction, whereas the expiratory flow-volume loop is linearly reduced throughout expiration in a purely restrictive pattern of ventilation.21 Moreover, although VC was mildly reduced in patients with PPH, the reduction in end expiratory flow remained significant after correction for VC. These findings are in agreement with previous observations in small groups of PPH patients.9,10 The indices of premature airway closure (RV and RV/TLC) were significantly increased in PPH, as reported earlier.9 Our data show a significant correlation of expiratory airflow limitation with premature airway closure in PPH. With TLC remaining unchanged, the increase in RV encroaches on VC, resulting in VC reduction. In patients with chronic congestive heart failure (CHF) due to ischaemic or dilated cardiomyopathy we have found a similar reduction in VC, but without an increase in RV and obstruction.22,23 While in CHF cardiac enlargement may contribute to a reduction in VC, in PPH small airway obstruction predominantly affects VC by premature airway closure and lung hyperinflation.
There was no correlation between expiratory airflows and haemodynamic parameters in our patients, and MEF75, MEF50, and MEF25 did not differ between patients with a PAPmean above and below the median. These findings suggest that airflow limitation may occur independently of the severity of PPH. However, as RV/TLC was correlated with PAPmean, peripheral airflow obstruction may reflect the underlying vascular disease and its haemodynamic consequences. This concept is supported by experimental data3,4 and by a small study9 in 11 patients with PPH showing that airflow limitation at the lower part of VC was associated with airway narrowing, bronchial wall thickening, and lymphocyte infiltrates.
It might be speculated that the increased production of cytokines and growth mediators in the pulmonary vasculature in PPH also causes proliferation in adjacent small airways.1 Moreover, in PPH there is decreased endothelial synthesis of the vasodilator nitric oxide (NO)24 and increased levels of the vasoconstrictor endothelin-1 (ET-1)25 which might also affect peripheral airway function since both mediators have similar effects on vascular and airway smooth musculature.26,27 Coupling between pulmonary blood vessels and airways has been attributed to mechanical forces due to shared structural changes in vessels and airways, or to vascular rigidity leading to an impairment of lung elastic recoil.2 It remains to be determined whether the presence of vasoconstrictive and proliferative mediators such as ET-1 or the lack of vasodilatory and antiproliferative mediators such as NO and prostacyclin may directly affect the function of peripheral airways in PPH.
In PPH the airway obstruction may be unidentified if only FEV1/VC or Rtot are measured, so measurement of expiratory flow is recommended during the routine evaluation of patients with PPH. Since expiratory airflow limitation may contribute to symptoms and exercise limitation in patients with PPH, pharmacological reversal of small airways dysfunction might be beneficial. Preliminary observations suggest reversibility of airway obstruction with salbutamol.28 This observation is supported by a recent study in children with PPH and the Eisenmenger's syndrome in which inhalation of albuterol resulted in reversibility of airflow obstruction.29 It also corresponds to data from patients with pulmonary hypertension secondary to CHF in whom the inhalation of ipratropium bromide improved FEV1, expiratory flow rates, and exercise limitation without affecting haemodynamics.30,31 Further evaluation of reversibility of peripheral airway obstruction and possible beneficial effects on exercise capacity and symptoms in patients with PPH is required.
Acknowledgments
The authors acknowledge Professor Neil B Pride, National Heart and Lung Institute, Hammersmith Hospital/Royal Brompton Hospital, London for most valuable and helpful discussions.