Article Text

Abstract
Background: The number of patients with tuberculosis has been increasing slowly in England and Wales since the late 1980s. HIV infection has been a contributory factor to increases in tuberculosis in a number of comparable industrialised countries. This study investigated the extent of tuberculosis and HIV co-infection in England and Wales in 1993 and 1998, and estimated its contribution to the increase in tuberculosis observed during this period.
Methods: Patients aged 16–54 years old at diagnosis on the 1993 and 1998 National Tuberculosis Survey databases were matched with those on the HIV/AIDS patient database. A coded process maintained patient confidentiality. Primary outcome measures were the increase between 1993 and 1998 in the numbers with both infections reported and an estimate of the proportion of the increase in tuberculosis during this period attributable to HIV co-infection.
Results: In 1993 61 (2.2%) tuberculosis patients aged 16–54 years matched with patients reported to the HIV database, increasing to 112 (3.3%) in 1998 (p=0.08; OR 1.35; 95% CI 0.97 to 1.87). Patients co-infected with HIV contributed an estimated 8.5% of the increase in number of tuberculosis patients between 1993 and 1998 nationwide (11% in London). In both years prevalence of co-infection was greatest in London and in patients of white and black African ethnic groups.
Conclusions: In 1998 the number of tuberculosis patients co-infected with HIV in England and Wales, though still small, had nearly doubled since 1993, with most of the increase occurring in London. As HIV infection may be undiagnosed in patients with tuberculosis, and tuberculosis may be unreported in patients with diagnosed HIV infection, the true extent of co-infection will have been underestimated by this study. In addition, constraints in coded matching make it inevitable that some reported co-infections are missed. Routine HIV testing of all patients with tuberculosis should now be considered, particularly in patients of white or black African ethnic origin under 55 years of age.
- tuberculosis
- HIV
- AIDS
- co-infection
Statistics from Altmetric.com
Recent routine annual notification data and laboratory reports show rising numbers of patients with tuberculosis in England and Wales, particularly in London (Notification of Infectious Diseases database, Public Health Laboratory Service Communicable Disease Surveillance Centre (PHLS CDSC), 1988–1998; CDSC LabBase data, 1988–1998). Five-yearly national tuberculosis surveys in England and Wales have been carried out since 1978, and the last three surveys (1988, 1993, 1998) have reflected these increases.1–3
The association between HIV infection and tuberculosis is well established4–8 and, in many countries, the HIV epidemic has played a large part in the rise of tuberculosis.7 Although some estimates have been made previously on local9–11 as well as national2,12 prevalence of co-infection in England and Wales, it is not known to what extent HIV infection has contributed to the most recent national increase in tuberculosis. We examined this by investigating the extent of the overlap of tuberculosis (as reported to the 1993 and 1998 national surveys) and HIV infection (using diagnosed HIV infections reported to the PHLS CDSC).
METHODS
In June 2000, reports on patients in England and Wales aged 16–54 years diagnosed with tuberculosis in 1993 and 1998 were selected from tuberculosis survey databases for those years. These named patient data were then “Soundex” coded—that is, the surnames were replaced by their initial letter followed by a three digit coding of subsequent letters.13 Other variables selected were date of birth, sex, ethnic group, and health authority (HA) of residence. The HIV/AIDS database contains Soundex coded data for individuals with a laboratory diagnosis of HIV infection (since 1984, when tests became available) and those with a clinical diagnosis of AIDS (since 1982). Variables selected from this database were Soundex code, sex, date of birth, ethnic group, area of report, and likely route of HIV infection.
The HIV and STI Division of CDSC carried out the matching of the extracted tuberculosis dataset to the HIV/AIDS database using Soundex code, sex, and date of birth. Where matching was in doubt, additional survey data were compared with HIV data to confirm the match—for example, HA/area of report, ethnic group. After further consideration, an additional co-infected case for 1998 was excluded from these analyses (resulting in a different overall figure from that published previously3).
Aggregate data from the matched patient reports for 1993 and 1998 were produced; these were summarised and compared to observe changes over time. Logistic regression analysis was performed to investigate the association between the independent variable (number of co-infected patients) and the predictor variables (year of survey, sex, ethnic group, and geographical area). Interactions between predictor variables were investigated.
RESULTS
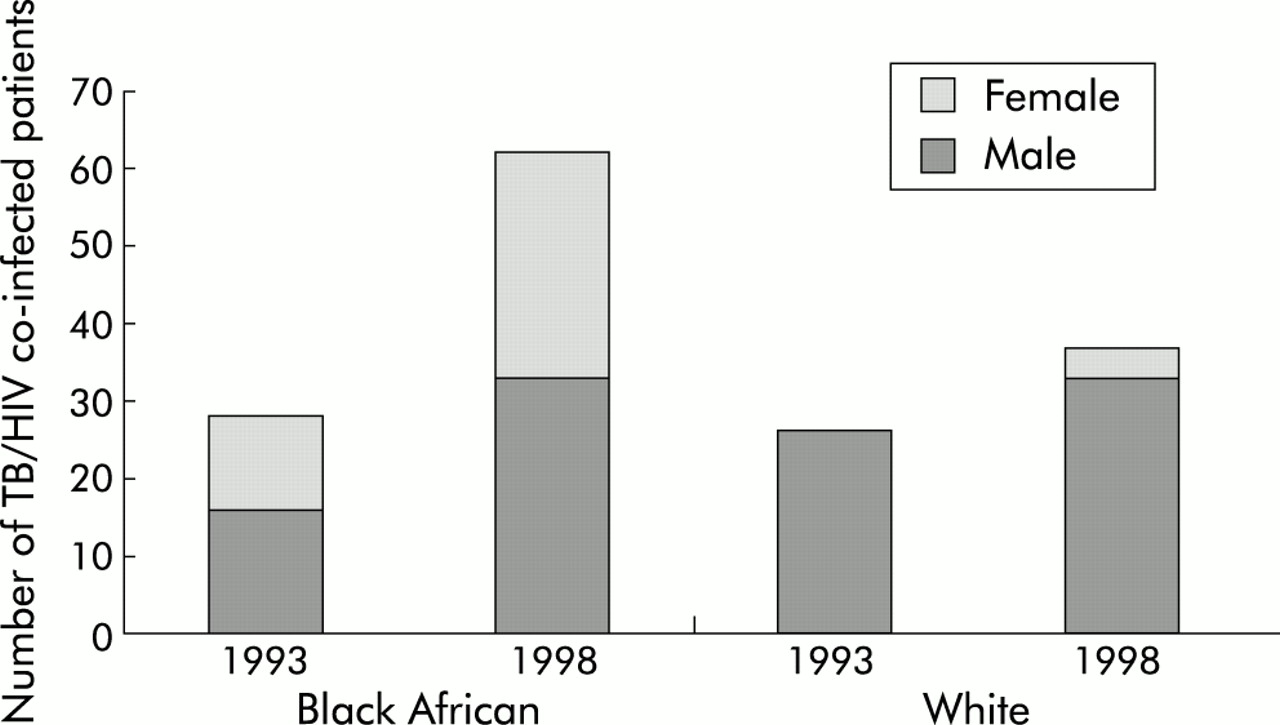
A total of 2833 tuberculosis patients aged 16–54 years in England and Wales were included in the 1993 tuberculosis survey database. In 1998 this increased by 21% to 3432. For 1993, 61 (2.2%) tuberculosis patients in this age group could be matched to the HIV database, compared with 112 (3.3%) for 1998. For both years most of those matched were male, of black African or white ethnicity (fig 1), and were reported from London (table 1). In a logistic regression analysis, taking into account the effects of sex, ethnic group, and geographical location on the distribution of tuberculosis, there was only weak evidence of an overall increase in co-infection in England and Wales between 1993 and 1998 (p=0.08, odds ratio (OR) 1.35; 95% CI 0.97 to 1.87).
Sex, ethnic group, and geographical distribution of cases of tuberculosis aged 16–54 years at diagnosis and those co-infected with HIV, 1993 and 1998

{kind=link}
Distribution of sex by main ethnic groups for adult tuberculosis patients (aged 16–54 years at diagnosis) co-infected with HIV in England and Wales, 1993 and 1998.
Geographical location
In the 16–54 age group for both years, a sizeable proportion (though less than half) of tuberculosis patients were reported from London (41% in 1993; 46% in 1998). Co-infected patients, however, were predominantly reported from London (64% in 1993; 77% in 1998).
Tuberculosis and HIV co-infection: London
Between 1993 and 1998 the number of patients with tuberculosis in the 16–54 year age group increased by 36%, while the number with both tuberculosis and HIV infection more than doubled (table 1). During this time national tuberculosis surveys showed that the number of white patients with tuberculosis decreased while the number in the black African ethnic group nearly doubled.3 In contrast, for the same period the number of co-infected patients of white ethnicity increased by about two thirds, while co-infected patients of black African origin increased by a factor of 2.5 (table 1).
The proportion of white patients with tuberculosis aged 16–54 years co-infected with HIV nearly doubled between 1993 and 1998 (from 5.2% to 9.8%), while the proportion of black African patients with tuberculosis who were co-infected increased by about one third (from 7.4% to 10%). Taking into account any differences between 1993 and 1998 in a logistic regression analysis, female black African patients with tuberculosis were more likely to be co-infected with HIV than white female patients (OR 7.1; 95% CI 2.4 to 20.7), but this was not the case for men (OR 0.84; 95% CI 0.52 to 1.32).
Tuberculosis and HIV co-infection: outside London
The number of patients with tuberculosis aged 16–54 years reported from outside London increased by 11% between 1993 and 1998 and in both years most were of Indian subcontinent (ISC: India, Pakistan and Bangladesh) ethnic origin. In both years approximately half of all patients with tuberculosis in this age group were women. During the same period the number of 16–54 year old patients co-infected with HIV reported from outside London increased by 18% and most were of white ethnicity. However, despite their higher numbers, there was a smaller proportion of co-infection in white than in black African patients with tuberculosis in both years. In contrast to patients reported from London, the proportion of tuberculosis patients co-infected with HIV of white ethnic origin outside London only slightly increased between 1993 and 1998 (from 1.8% to 2.0%) while the proportion of those of black African ethnic origin decreased (from 15% to 10%). Very few co-infected patients outside London were women (3/22 in 1993 and 5/26 in 1998; table 1).
Likely route of HIV infection
Among the men with tuberculosis co-infected with HIV in 1993, 47% (mostly black African) acquired HIV through heterosexual encounters and 45% (mostly white) through sex between men (table 2). Injecting drug users comprised only a small proportion of men co-infected with HIV (6.1%), all of whom were white. All co-infected women were of black African ethnic origin and were reported to have acquired HIV heterosexually. In 1998 the proportion of co-infected men with heterosexually acquired HIV increased to 55% (as in 1993, most were of black African ethnicity). Only one third of the men had homosexually acquired HIV infection and, again, most of these were white. Again, injecting drug users accounted for a small proportion of co-infected patients (6.3%), and 95% of women had acquired HIV through heterosexual contact.
Sex, HIV exposure category, and ethnic group for patients aged 16–54 years at diagnosis co-infected with tuberculosis and HIV in 1993 and 1998
Estimate of contribution of HIV to increase in tuberculosis
Between 1993 and 1998 the number of patients with tuberculosis in England and Wales in the 16–54 year age group increased by 599 (from 2833 to 3432). Reports from London contributed 415 (69%) to this increase. The number of patients in this age group known to be infected with both tuberculosis and HIV increased by 51 for England and Wales (47 from London). Thus, HIV infection is estimated to have contributed to 8.5% (95% CI 6.4 to 11.0) of the increase in tuberculosis between 1993 and 1998 in England and Wales. The estimate of the contribution of HIV infection was 11% (95% CI 8.4 to 14.8) in London and only 2.2% (95% CI 0.6 to 5.5) outside London.
DISCUSSION
Nearly twice as many patients with tuberculosis aged 16–54 years were known to be co-infected with HIV in 1998 than in 1993. Most dually infected patients were reported from London, where the majority of the increase in co-infection during this period was observed. A large proportion of co-infected patients were of white or black African ethnic group and very few were of ISC origin. In contrast, many patients with tuberculosis alone were of ISC ethnicity and fewer were of black African origin.2,3 The ethnic distribution of co-infected patients, rather than mirroring that of tuberculosis patients, therefore appears to reflect the ethnic mix of adults with HIV infection in England and Wales (PHLS AIDS and STD Centre, CDSC & SCIEH, AIDS/HIV quarterly surveillance tables to end June 2000, unpublished). The sex distribution of co-infected patients of black African (approximately equal) and white ethnicity (predominantly men) also mirrors the patterns observed for those with HIV infection rather than tuberculosis.
Although it is easier to investigate smaller local databases which contain patients' names, results from such studies are difficult to extrapolate for the country as a whole as both tuberculosis and HIV infection are unevenly distributed across the nation. Matching two large national databases, however, is also problematic. Errors can arise during Soundex coding, recording and transcribing date(s) of birth or through missing data, inhibiting recognition of matched reports.
Many HIV infections are undiagnosed and therefore unreportable and local anonymised HIV seroprevalence studies of tuberculosis patients in London have estimated higher overall proportions of co-infection than reported here,9,11 but comparable co-infection rates to ours for patients of white (5% v 4.2%) and black African (14% v 10%) origin.11 Although care must be taken before extrapolating local study results to a wider geographical area, the likelihood is that estimates reported by this study do not reflect the full extent of co-infection. In addition, although notification of tuberculosis is a statutory requirement in the UK, undernotification of tuberculosis in patients co-infected with HIV is known to occur.14–17
The national tuberculosis notifications survey carried out in 1993 investigated HIV co-infection by matching patients reported to the PHLS AIDS centre with the tuberculosis patient register and by anonymous HIV testing of notified tuberculosis patients.2 The different methodology used in the current study has resulted in an estimate of the proportion of co-infected patients for 1993 (2.2% overall; 3.3% in London) which differs slightly from earlier published results (2.3% overall; 4.3% in London). In the current study, use of the same method to estimate the proportions co-infected in 1993 and 1998 was therefore more appropriate for observation of changes in co-infection, even though the method was likely to underestimate its extent.
In Africa the most common route of HIV infection is via heterosexual intercourse while, in the UK, homosexual transmission is the most often reported route.5,18–20 All of the co-infected patients of black African ethnic origin in this study for whom place of birth was known were born in Africa (data not shown), and for the majority the reported route of HIV acquisition was heterosexual. It is likely that most of this group of patients were exposed to both tuberculosis and HIV before entry to the UK.
Homosexually acquired HIV is likely to be diagnosed earlier in disease progression than heterosexually acquired HIV21 as a result of risk recognition in the former group. When HIV is diagnosed early, multi antiretroviral treatments widely available in the UK since the mid 1990s can delay the onset of AIDS-defining conditions, including tuberculosis.
In England and Wales the demographic shift observed in tuberculosis patients towards patients born abroad and the delay in disease progression among those with early diagnosed HIV infection mean that an increasing proportion of tuberculosis and HIV co-infected patients may now present to non-genitourinary medicine physicians unaware of their concomitant HIV infection. Any physician in London who may diagnose a case of either tuberculosis or HIV must be made aware of the greater likelihood of co-infection in this region, and should consider testing patients for the other infection when one is recognised. In addition to testing, however, the aim must be notification of all tuberculosis patients with diagnosed HIV infection and reporting of HIV infection in all tuberculosis patients.
This study has found an estimated minimum prevalence of HIV infection in tuberculosis patients in 1998 of 1 in 19 in those aged 16–54 years in London (1 in 10 for those of black African and white ethnic groups) and 1 in 70 for those in the remainder of England and Wales (1 in 10 and 1 in 50 for those of black African and white ethnic groups). This should be sufficient to recommend that all tuberculosis patients in England and Wales up to the age of 55 years should be tested for HIV infection. The added burden this would create (especially in high prevalence areas where resources may already be stretched), and potential language and cultural issues involved must be considered alongside the difficulties which may arise from targeted HIV testing of tuberculosis patients from specific ethnic groups. Current UK guidance22 recommends HIV testing with counselling and informed consent only if the tuberculosis patient is considered to be from a high risk area or background. In view of the findings from this study, this guidance should be reviewed.
Acknowledgments
The authors would like to thank Nichola Goddard for initial work in matching the tuberculosis to the HIV/AIDS database, Barry Evans for advice and comments on the final draft, and all clinical and public health practitioners for reporting cases of both HIV and tuberculosis. The study was performed using existing data from the 1993 and 1998 national tuberculosis surveys and the HIV/AIDS patient database. There are no conflicts of interest.