Article Text

Abstract
Background: Exhaled nitric oxide has been proposed as a marker for airway inflammation in asthma. The aim of this study was to compare exhaled nitric oxide levels with inflammatory cells and mediators in bronchoalveolar lavage fluid from asthmatic and normal children.
Methods: Children were recruited from elective surgical lists and a non-bronchoscopic bronchoalveolar lavage (BAL) was performed after induction of anaesthesia. Exhaled nitric oxide (parts per billion) was measured by two techniques: tidal breathing and restricted breath.
Results: Median (interquartile range) exhaled nitric oxide measured by restricted breath was increased in asthmatics compared with normal children (24.3 (10.5–66.5) v 9.7 (6.5–16.5), difference between medians 14.6 (95% CI 5.1 to 29.9), p=0.001). In asthmatic children exhaled nitric oxide correlated significantly with percentage eosinophils (r=0.78, p<0.001 (tidal breathing) and r=0.78, p<0.001 (restricted breath)) and with eosinophilic cationic protein (r=0.53, p<0.01 (restricted breath)), but not with other inflammatory cells in the BAL fluid. The area under the receiver operator characteristic curves for the prediction of the presence of eosinophilic airways inflammation by exhaled nitric oxide (tidal and restricted) was 0.80 and 0.87, respectively.
Conclusions: Exhaled nitric oxide correlates closely with percentage eosinophils in BAL fluid in asthmatic children and is therefore likely to be a useful non-invasive marker of airway inflammation.
- asthma
- nitric oxide
- eosinophils
- children
Statistics from Altmetric.com
Exhaled nitric oxide (eNO) is known to be increased in both adult and childhood asthma.1–4 Patients with acute asthma have high levels of eNO which decrease with oral corticosteroid treatment.5 Inhaled corticosteroids are known to reduce eNO levels in asthmatic subjects not previously treated with them,6,7 and recently a leukotriene receptor antagonist has been shown to reduce eNO levels in asthmatic children.8,9 Several, but not all, studies have shown negative correlations between eNO levels and PC20 methacholine/histamine,10–13 and forced expiratory volume in 1 second (FEV1).4,7,11,12,14,15 There is a correlation between eNO and the percentage of eosinophils in induced sputum from both adults10,12 and children16,17 with asthma, but the relationship between eNO levels and the percentage of eosinophils in bronchoalveolar lavage (BAL) fluid in children has not been reported. This study examines direct measures of airway inflammation in BAL fluid with eNO concentrations in children.
METHODS
Participants
Seventy one children (29 atopic asthmatics, 15 atopic normal controls, and 27 non-atopic normal controls) attending the Royal Belfast Hospital for Sick Children for elective surgical procedures were recruited. BAL was performed using a non-bronchoscopic technique immediately after induction of anaesthesia, as described previously.18,19 Parental written informed consent was obtained and the study was approved by the research ethics committee.
Exhaled nitric oxide measurement
Exhaled NO was measured online by both restricted breath analysis and the tidal breathing technique according to the recommendations of the American Thoracic Society20 using a chemiluminescence analyser (NOA 280, Sievers Instruments Inc) with a sensitivity of 0.5 parts per billion (ppb), a detection range of 0.5–500 000 ppb, and a response time of 200 ms. Briefly, for the restricted breath technique the subject was instructed to inhale through the mouth to total lung capacity and immediately exhale through the mouthpiece against a fixed resistance. Maintenance of a constant flow was achieved using a visual analogue feedback on the computer screen. A flow rate of 50 ml/s was used which corresponded to a mouth pressure of 17 cm H2O. An exhalation of at least 6 seconds with a plateau of at least 2 seconds duration was required to calculate the NO plateau. The tidal breathing technique was an online breath by breath analysis and the mean NO plateau was calculated from at least five breaths. If the ambient NO level was greater than 20 ppb, subjects inspired room air through a nitric oxide scrubber.
Subject classification
A detailed respiratory/atopy questionnaire was administered to parents of all children.19 Subjects were classified as asthmatic if they had a history of wheezing on different occasions (precipitated by respiratory infection, exercise, or exposure to allergens) and if a physician or general practitioner had diagnosed them with asthma. All children were assessed by the anaesthetist and were deemed sufficiently stable to undergo a general anaesthetic. Details of asthma medication and medication compliance were also obtained. Atopy was defined as in previous publications18,19 as either a personal history of atopic disease or two first degree relatives with atopic disease or a raised total IgE. All subjects were free of current respiratory infection.
Bronchoalveolar lavage and assessment of airway inflammation
BAL fluid was centrifuged (200g, 5 min, 4°C) and cytospin preparations produced by a modification of the coverslip method.19 Cells were stained with Diff-Quik for differential cell counting (minimum of 1000 cells) or toluidine blue for mast cell counting (3000–5000 cells).18 Supernatants from the BAL fluid were stored at –70°C until measurement of eosinophil cationic protein (ECP) or histamine using commercially available radioimmunoassays (Pharmacia Upjohn Diagnostics and Immunotech, respectively). Total serum IgE was measured using a commercially available radioimmunoassay (Pharmacia Upjohn Diagnostics). The percentage of blood eosinophils was also quantified.
Analysis of data
All values are quoted as median and interquartile range (IQR). Spearman's correlation was used to compare inflammatory cells and mediators with eNO. The Mann-Whitney U test (Hodges-Lehmann difference between medians) and the Kruskal-Wallis test (with multiple comparisons adjustment) were used to compare eNO levels between subgroups. Receiver operating characteristic curves were generated to investigate the sensitivity, specificity, and positive likelihood ratio of eNO and blood eosinophils to predict the presence of raised eosinophils in the BAL fluid (≥0.86%, our upper normal reference limit18). Statistical analyses were performed using Unistat 5 (Unistat Ltd, London, UK).
RESULTS
Twenty nine children with atopic asthma, 15 atopic normal control children, and 27 non-atopic normal children underwent both BAL and measurement of eNO levels. The median ambient level pf NO was 4.0 ppb (range 0.3–43.0). Demographic data, eNO values, and percentage BAL fluid eosinophils for the three groups are shown in table 1. Nine asthmatic subjects were taking inhaled corticosteroids and all had been on this treatment for at least 3 months. Eight children were treated with 200–800 μg/day inhaled corticosteroids (budesonide, n=5; beclomethasone, n=2; fluticasone, n=1). One child was taking nebulised budesonide at a dose up to 4 mg/day.
Baseline demographic characteristics, eNO values, and percentage BAL fluid eosinophils in the three groups (n=71)
Exhaled NO levels
Median (IQR) eNO values (ppb) for the combined non-asthmatic control subjects (atopic and non-atopic) were 6.0 (3.6–8.9) using the tidal breathing method and 9.7 (6.5–16.5) with the restricted breath technique. The levels of eNO were significantly higher in asthmatic than in non-asthmatic children using both the tidal breathing method (difference between medians 3.4 ppb (95% CI 0.9 to 6.8), p=0.01) and restricted breath analysis (difference between medians 14.6 ppb (95% CI 5.1 to 29.9), p=0.001).
When the non-asthmatic control group was divided into atopic and non-atopic controls, there was no difference between the subgroups in median eNO levels measured by the tidal breathing method. However, the non-atopic controls had significantly lower levels than the asthmatic group (difference between medians 2.8 (95% CI 0.8 to 7.8), p=0.01, fig 1A). With the restricted breath method there was also no difference between atopic and non-atopic non-asthmatic controls but again there was a statistically significant difference between non-atopic controls and the asthmatic children (difference between medians 14.8 (95% CI 5.7 to 34.2), p<0.001, fig 1B).
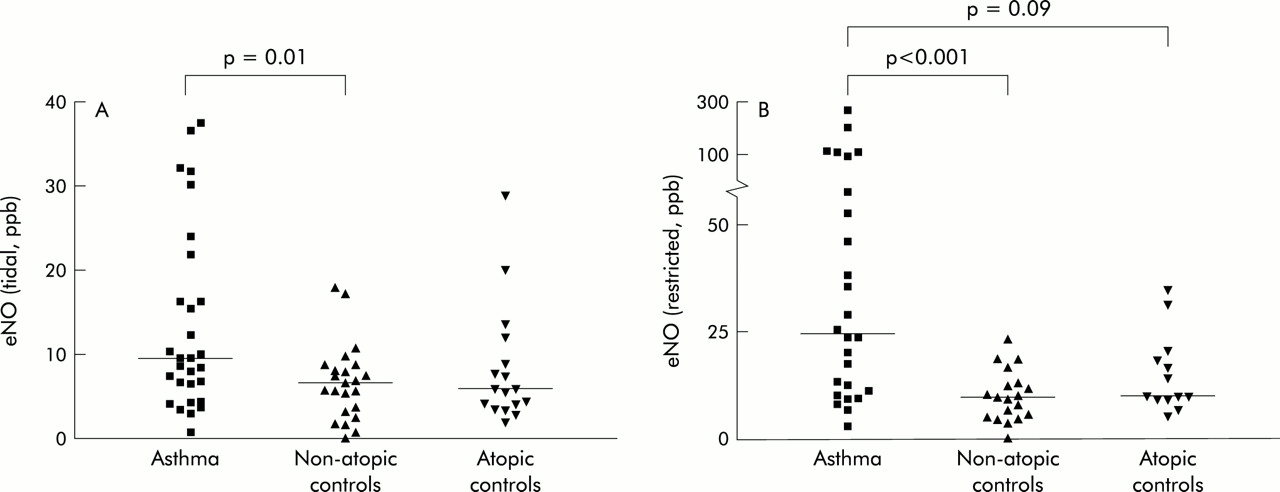
Exhaled NO levels in asthmatic patients, non-atopic controls, and atopic controls measured by (A) the tidal breathing method and (B) restricted breath analysis. Horizontal bars represent median values (Mann-Whitney U test).
When eNO levels (measured by the tidal breathing method or by restricted breath analysis) and percentage BAL fluid eosinophils in the asthmatic subjects were analysed according to whether or not the subject was receiving inhaled corticosteroids, no significant differences were found (data not shown).
Correlation analyses
The levels of eNO correlated with percentage eosinophils in BAL fluid using both the tidal breathing technique (r=0.78, p<0.001, fig 2A) and restricted breath analysis (r=0.78, p<0.001, fig 2B) in asthmatic children but not in non-asthmatic controls (tidal breathing: r=–0.01, p=0.99; restricted breath: r=0.28, p=0.13). In the subgroup of asthmatics taking inhaled corticosteroids, the correlation between percentage BAL eosinophils and eNO remained (tidal breathing: r=0.78, p=0.01; restricted breath: r=0.78, p=0.04) and was similar to that found in the steroid naïve asthmatic patients (tidal breathing: r=0.79, p<0.001; restricted breath: r=0.84, p<0.001). Exhaled NO levels did not correlate with percentage mast cells in asthmatic patients measured by tidal breathing (r=–0.18, p=0.52) or restricted breath analysis (r=0.08, p=0.79), nor did it correlate with any other cell type found in BAL fluid (data not shown). ECP was not detectable in BAL fluid from atopic control children, in 26 of 27 non-atopic control children (1.9 μg/l (1.9–1.9)) and 19 of 29 asthmatic children (1.9 μg/l (1.9–2.4)). Despite this, there was a significant positive correlation in asthmatic children between eNO levels and BAL fluid levels of ECP (tidal breathing: r=0.52, p=0.004; restricted breath: r=0.53, p=0.007). Furthermore, in asthmatic children there was a weak but non-significant correlation (tidal breathing: r=0.4, p=0.09; restricted breath: r=0.4, p=0.09) with blood eosinophil count (4.2% (2.6–7.9)). BAL fluid histamine concentrations in asthmatic children (3.3 nM (0.2–17.1)) correlated poorly with eNO levels (tidal breathing: r=0.25, p=0.31, restricted breath: r=0.35, p=0.19).

Spearman's correlations (r) between exhaled NO levels of asthmatic subjects measured by (A) tidal breathing and (B) restricted breath analysis and percentage BAL fluid eosinophils.
Receiver operating characteristic (ROC) curves
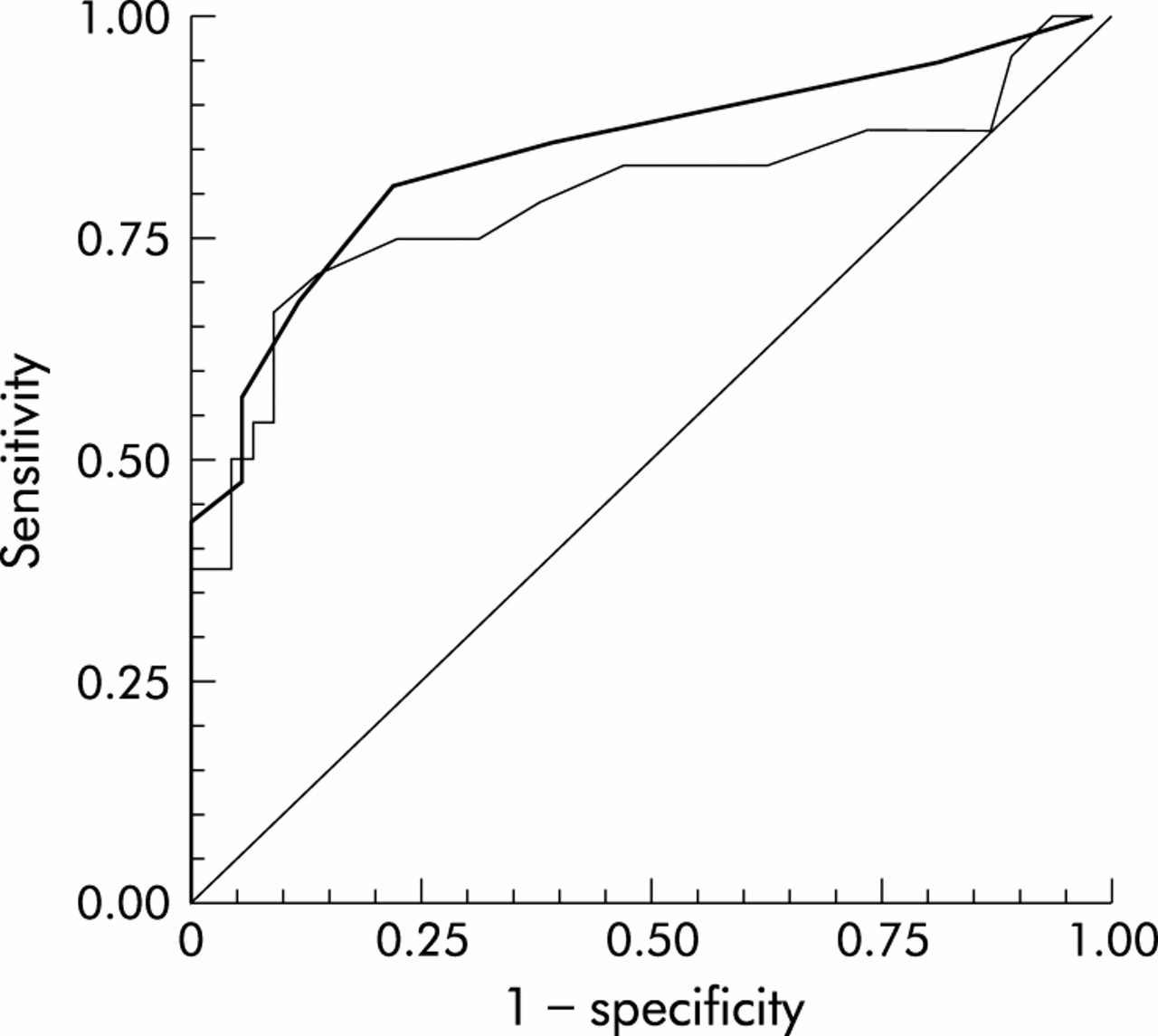
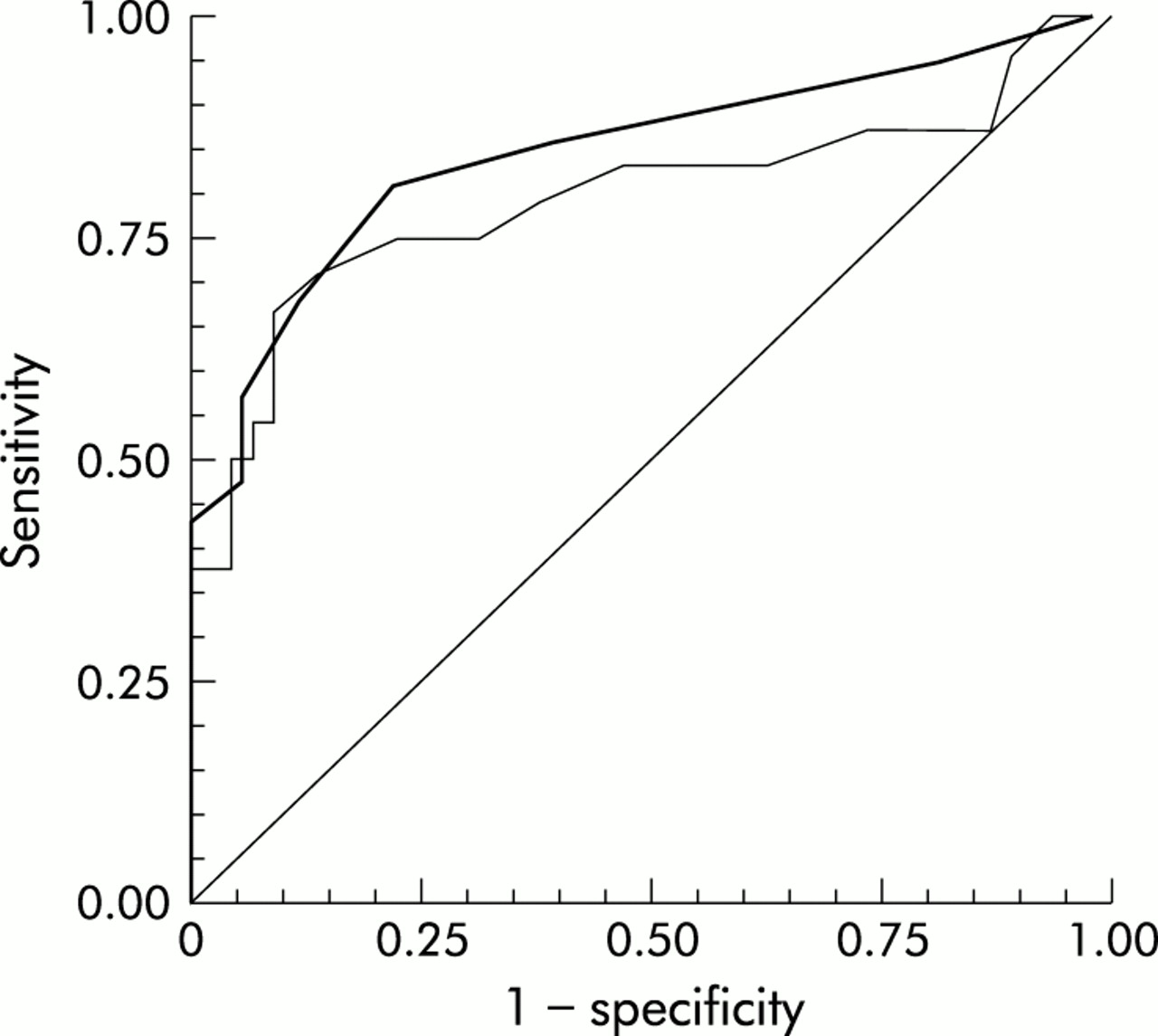
A BAL eosinophil value of 0.86% was defined as the cut off value for defining the presence or absence of eosinophilic airways inflammation as this value has been shown previously to be the upper 95% confidence interval for the 95th percentile in normal children.18 The ROC curves using eNO levels (measured by tidal breathing and restricted breath analysis) to predict airways inflammation are shown in fig 3. The area under the curve (AUC) and the best sensitivity, specificity, and positive likelihood ratio with corresponding cut off values for eNO levels and blood eosinophil count are shown in table 2. There was no significant difference in the AUC when eNO levels (measured by tidal breathing or restricted breath analysis) or blood eosinophil percentage were used to predict the presence of eosinophilic airways inflammation.
Comparison of the sensitivity, specificity, and likelihood ratio of a positive test for the prediction of airways inflammation with the corresponding cut off values for eNO (measured by tidal breathing (TB) or restricted breath analysis (RB)) and blood eosinophil count
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve for the presence of airways inflammation. Heavy line represents eNO levels measured by restricted breath analysis (area under curve (AUC)=0.87), lighter line represents eNO levels measured by tidal breathing (AUC=0.80); diagonal line is chance predictor (AUC=0.5).
DISCUSSION
Two different techniques were used to measure eNO levels in children and compared with inflammatory markers in BAL fluid. Restricted breath analysis could be successfully performed in children as young as 4 years and the tidal breathing technique was performed by children as young as 3 years. However, the former technique is likely to give more reliable results because it is less subject to the influence of nasal NO.21 The actual eNO values obtained in this study by restricted breath analysis are somewhat higher than in other published studies in children.16,17 The discrepancy may relate to the different flows generated at the mouth in each study. Plateau levels of eNO are known to increase with decreasing flow at the mouth.21 In our study the pressure at the mouth was 17 cm H2O and the flow was comparatively low at 50 ml/s, whereas other studies have used lower mouth pressures, typically 5 cm H2O, and higher flows.16,17
We have confirmed that asthmatic children have increased eNO levels compared with normal children, which is in keeping with other studies.3,4 Asthmatic children had significantly higher eNO levels than non-atopic non-asthmatic controls. Atopic non-asthmatic controls had intermediate eNO levels but there were no statistically significant differences in eNO levels between this group and either the non-atopic controls or asthmatics. There has been some debate as to whether atopy is an independent factor for increased eNO levels in non-asthmatic subjects. One large study of 157 children22 showed that eNO increased in relation to the number of positive skin prick reactions, but another study showed no difference in eNO levels between atopic and non-atopic normal children.23 Our study may lend support to the former, although the numbers in our subgroups are relatively small. One potential deficiency in our study is the absence of skin prick test data to help define atopy, but instead we classified children as atopic based on a personal and/or strong family history of atopy and total serum IgE concentrations. Only four children were classified as “atopic” based solely on having two atopic parents. Exclusion of these patients would not alter our results.
This study shows that, in asthmatic children but not in controls, eNO levels and BAL fluid eosinophil percentages correlate well regardless of the methods used to measure eNO. In contrast, no correlations were found between eNO levels and other inflammatory cells, particularly mast cells which are increased in the airways of asthmatic children.19 These findings are consistent with other studies comparing eNO with markers of airway inflammation in induced sputum both in adults and children.10,12,16,17 The value of eNO as a marker of eosinophilic inflammation in corticosteroid treated asthmatic subjects has been questioned as some unstable asthmatics treated with corticosteroids have normal eNO levels.12 In our study eNO levels correlated with percentage eosinophils in BAL fluid even in the corticosteroid treated group. The correlation in the corticosteroid treated subgroup was similar to that for the steroid naïve asthmatics and suggests that eNO may be a useful marker even in steroid treated asthmatics. This result is consistent with the study of Mattes et al who found a correlation between inflammatory markers in induced sputum and eNO levels in corticosteroid treated asthmatic children.16 By contrast, Piacentini et al found no correlation between eNO levels and sputum inflammatory markers in their corticosteroid treated asthmatic subjects.17 This discrepancy could be explained by the small numbers studied and the differences in clinical characteristics of the corticosteroid treated asthmatic subjects between studies. Although eNO levels and BAL histamine concentrations did not correlate, a significant correlation was found between eNO and ECP in BAL fluid in the asthmatic children. This is in agreement with the study by Mattes et al which showed a correlation between eNO and ECP levels (both serum and sputum)16 but contrasts with the findings of Piacentini et al.17 In the latter study the authors admit that the lack of correlation with sputum ECP levels is difficult to explain given the correlation with sputum eosinophils. The small numbers in their subgroups (10 steroid treated, 15 steroid naïve) may account for the lack of significant difference. Thus, as we have shown, eNO may not only serve as a non-invasive marker of airway eosinophil percentages but also as a marker of eosinophil activation within the airways.
The data obtained from plotting the ROC curves allow the clinical value of eNO as a non-invasive predictor of airways inflammation to be assessed and compared against blood eosinophil count. A cut off eNO value of 17 ppb measured by restricted breath analysis resulted in a sensitivity and specificity of 81% and 80%, respectively. Similar sensitivity and specificity results were obtained using a cut off eNO value of 9 ppb measured by tidal breathing. These results compare favourably with the results obtained with the blood eosinophil count. Similar results were obtained in a previous study in which blood eosinophils were examined as a non-invasive marker of airway inflammation.24 While no significant difference was seen when comparing the area under the curve for eNO levels and blood eosinophil count, we believe that eNO has advantages over the blood eosinophil count as it is minimally invasive and provides an immediate result which can be interpreted in a clinical context with the patient present.
In conclusion, we have shown that eNO measurement is a useful method of indirectly assessing eosinophilic airway inflammation in asthmatic children, whether or not they are taking inhaled corticosteroids at the time of measurement. It may also be a useful adjunct for diagnosing asthma (as recurrent wheezing plus eosinophilic airways inflammation), particularly in younger children where it is often difficult to get other objective measures of asthma.
Acknowledgments
The authors gratefully acknowledge the support of the National Asthma Campaign, UK, the Research and Development Office for Northern Ireland and Merck Sharpe & Dohme for an equipment grant.