Article Text

Abstract
Case reports of a short trachea with early branching of the main bronchi are uncommon. The case is presented of a 64 year old woman with upper airway obstruction due to this anatomical abnormality which caused breathlessness and wheezing that was misdiagnosed (and treated) as bronchial asthma for many years.
- short trachea
- upper airway obstruction
- misdiagnosis
Statistics from Altmetric.com
A 64 year old non-smoking woman with a diagnosis of bronchial asthma from the age of 12 was referred to our clinic in August 1999 with a diagnosis of difficult asthma characterised by persistent wheezing, chest tightness, and exertional dyspnoea. She had been treated for many years with inhaled and systemic glucocorticoids, theophylline, and long and short acting inhaled β2 agonists without satisfactory symptom control.
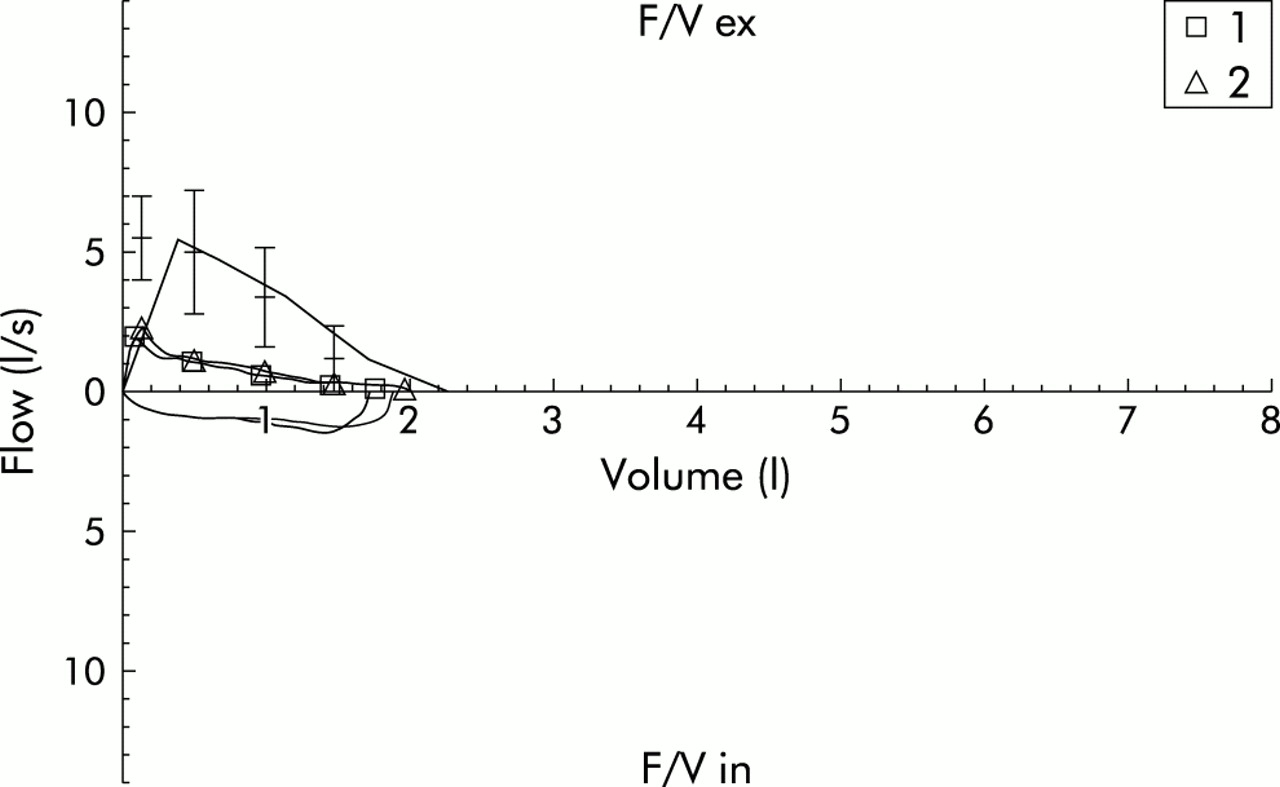
Physical examination showed a normal shaped chest and a mild retraction of the jugular “fossa” associated with the involvement of accessory muscles but was otherwise unremarkable. Auscultation revealed the presence of inspiratory wheezing without other pathological sounds and the chest radiograph was normal. Lung function tests showed forced expiratory volume in one second (FEV1) 1.06 l (56.3% of the predicted value), vital capacity (VC) 2.04 l (86.4% of the predicted value), peak expiratory flow rate (PEFR) 1.73 l/s (31.9% of the predicted value), and ratio of FEV1 to VCmax (FEV1/VCmax: Tiffenau index) 52.01% (67.6% of the predicted value). There was no improvement following inhalation of 200 μg salbutamol via metered dose inhaler. The flow-volume loop showed a remarkable decrease in airflow rates at all lung volumes on both forced inspiration and expiration, suggesting the presence of fixed upper airway obstruction (fig 1).

Flow-volume loops demonstrating a decrease in airflow rates at all lung volumes on both forced inspiration and expiration before (loop 1) and after (loop 2) inhalation of salbutamol, suggesting the presence of fixed upper airway obstruction.
A spiral computed tomographic (CT) scan of the thorax with 3D reconstruction was taken to study airway morphology. This revealed the presence of an anatomical anomaly consisting of a short trachea giving early origin to the main bronchi which were much longer than normal (fig 2). The diameters of the trachea and the right and left main bronchi measured on the CT scan were, respectively, 1.6 cm (normal range 1.3–2.3 cm), 0.85 cm (normal range 1.0–1.2 cm), and 0.70 cm (normal range 0.8–1.0 cm).1,2 The anatomical anomaly was confirmed by fibreoptic bronchoscopy. The tracheal length was 5 cm (normal length 12 cm) and it was possible to recognise only six cartilaginous rings (normal range 16–22).1 The carina was not widened and the orifices of the main bronchi appeared earlier in the tracheal lumen. The right main bronchus was 7.5 cm long (normal length <3 cm) and the left main bronchus length was 8 cm (normal length <5 cm).2 Video-assisted fibreoptic bronchoscopy also included detailed examination of the remaining bronchial tree and the origin of the right superior lobar bronchus showed a mild concentric stenosis. The remaining bronchial anatomy was normal.
{kind=link}
{kind=link}
Spiral CT scan of the thorax with 3D reconstruction showing the presence of a short trachea giving early origin to the main bronchi.
DISCUSSION
In many patients the clinical manifestations of upper airway obstruction are erroneously misdiagnosed as bronchial asthma, sometimes for long periods of time.3,4 Upper airway obstruction is called extrathoracic when a lesion obstructs the airway between the extrathoracic trachea and the nose, and intrathoracic when the lesion is distal to the thoracic inlet from the intrathoracic trachea down to the level of the 2 mm size airways.3,4 The symptoms referred by our patient (wheezing and exertional dyspnoea) can be caused by many different pathologies but the most common cause of expiratory and inspiratory wheezing is airflow obstruction.5 However, our study suggests again that wheezing should never be considered “a priori” due to bronchial asthma since it can be caused by any kind of airway obstruction.5,6 Data from many studies suggest that dyspnoea appears when there is an upper airway obstruction of less than 8 mm in adults.7 The clinical features of patients with upper airway obstruction are somewhat variable but are most often mistaken for those of asthma. The differential diagnosis of upper airway obstruction includes neoplastic and inflammatory diseases and bilateral vocal cord paralysis; however, it should also include congenital lower respiratory tract malformations.3 The classification of congenital lower respiratory tract malformations is very complex but, for practical purposes, they can be divided into two major categories: lesions that arise from the primitive foregut (cystic adenomatoid malformation) and those that originate in the pulmonary vasculature.8 The latter are often detected early in life because of signs and symptoms or other serious associated anomalies. Conversely, many of the lesions arising from the primitive foregut are asymptomatic and therefore not discovered until adulthood.8 Tracheobronchial malformations, particularly congenital tracheal and/or bronchial stenosis, are an extremely rare cause of upper airway obstruction in adults. However, abnormal bronchial branching patterns are so uncommon that they have not been included in a recent review on the adult outcome of congenital lower respiratory tract malformations.9 Despite an extensive search we could not find any other published case similar to the anomaly presented here.10
The diagnosis of upper airway obstruction is delayed in many patients despite the presence of symptoms, principally because of the low index of suspicion and many clinicians overlook the shape of the flow-volume loop. When the upper airway obstruction is fixed, both inspiratory and expiratory flows will be decreased whether the obstruction is intrathoracic or extrathoracic.3,4 Hence, the peculiar shape of the flow-volume loop (fig 1) gives the suspicion of upper airway obstruction. Once the diagnosis of upper airway obstruction is suspected, it can be confirmed by fibreoptic bronchoscopy and spiral CT scanning. We therefore suggest that an abnormal flow-volume loop should be a warning sign of upper airway obstruction and alert clinicians to diagnoses other than bronchial asthma.
Footnotes
-
Supported by Associazione per la Ricerca e la Cura dell'Asma (ARCA) Padua, Italy.