Article Text

Abstract
Background: Sarcoidosis is a systemic disease of unknown aetiology frequently affecting the lungs. CD4+ T cells, in particular, accumulate in the lungs, implicating them in the pathogenesis of the disease.
Methods: T cell receptor (TCR) variable (V) gene expression on bronchoalveolar lavage (BAL) fluid T cells and the HLA DR alleles of 121 Scandinavian patients with sarcoidosis was determined.
Results: As expected from our previous results, almost every DRB1*0301 (i.e. DR17) positive patient (67/69) had significantly increased numbers of AV2S3+ CD4+ T cells in the BAL fluid but normal levels in peripheral blood (that is, lung restricted expansions) compared with only six of 52 DRB1*0301 negative patients. Detailed genotypic HLA analysis showed that these six DRB1*0301 negative patients with lung restricted AV2S3+ T cell expansions had another HLA allele in common—the HLA-DRB3*0101 allele (also called DR52a)—which was not found in any other DRB1*0301 negative patient. A new group of sarcoidosis patients was therefore identified, characterised by a strict correlation between a distinct HLA allele and lung accumulated T cells expressing a particular TCR V segment. Furthermore, the HLA-DRB1*0301 and HLA-DRB3*0101 encoded molecules showed similarities, with identical amino acid sequences in regions important for antigen binding which may enable them to bind and present the same or similar antigenic peptides.
Conclusions: HLA-DRB3*0101 as well as DRB1*0301 positive sarcoidosis patients may have the capacity to present specific sarcoidosis associated antigens in such a way that AV2S3+ CD4+ T cells are stimulated preferentially, generating lung restricted AV2S3+ T cell expansions.
- T cell receptor
- HLA
- bronchoalveolar lavage
- sarcoidosis
Statistics from Altmetric.com
The general concept of the immunopathogenesis of sarcoidosis includes exposure to and subsequent presentation of antigen by antigen presenting cells (APC) to T lymphocytes which, in genetically predisposed individuals, results in exaggerated inflammation and disease.1 The interaction between APC, presenting peptides derived from the primarily exogenous antigens in the context of HLA class II molecules (HLA-DR, HLA-DP, HLA-DQ), and the T lymphocyte recognising the antigen-HLA complex using its T cell receptor for antigen (TCR) is of crucial importance for the subsequent immune response. During T cell development in the thymus the α and β variable regions of the TCR are constructed through a random DNA recombination by which V (variable), D (diversity), and J (joining) gene segments are rearranged.2
In most patients with sarcoidosis the lungs are involved, with accumulation of activated CD4+ T cells.3 These lung T cells can be analysed by bronchoalveolar lavage (BAL) and display a Th1 cytokine profile with increased production of interferon (IFN)γ and interleukin (IL)-2.4,5 We have described a positive correlation between the HLA-DRB1*0301 allele (DR17) and lung CD4+ T cells expressing TCR AV2S3 in a limited number of Scandinavian patients. HLA-DRB1*0301 positive Scandinavian patients with sarcoidosis were found to have large populations of AV2S3 expressing T cells in their lungs but normal levels in paired peripheral blood samples (lung restricted T cell expansions).6 Sequence analyses of the TCR α chains of AV2S3 expressing lung T cells suggested that they had been exposed to and stimulated to proliferate by an as yet undefined sarcoidosis associated antigen,7 and recently AV2S3+ cells were found to correlate with clinical manifestations of sarcoidosis.8
In the present study we investigated TCR AV2S3 expression in BAL fluid and peripheral blood T cells of 121 ethnically homogenous Scandinavian patients and analysed HLA-DRB3 alleles in addition to DRB1 alleles. In addition to DRB1*0301 positive patients, we identified a new group of patients with lung restricted T cell expansions expressing AV2S3. These patients were HLA-DRB1*0301 negative and DRB3*0101 positive. Interestingly, DRB1*0301 and DRB3*0101 molecules have distinct similarities in regions important for antigen peptide binding, indicating that, in both these patient groups, an identical antigenic peptide might be presented and recognised preferentially by AV2S3+ T cells. In addition, peripheral blood T cells of DRB1*0301 positive patients had small but significantly higher relative numbers of AV2S3 expressing T cells, which suggests that the AV2S3+ cells are not compartmentalised exclusively in the lungs of these patients and indicates the systemic nature of the disease.
METHODS
Subjects
BAL fluid and paired peripheral blood lymphocytes (PBL) of 121 white Scandinavian patients with sarcoidosis were analysed, 19 of whom had been included in a previous report.6 The diagnosis of sarcoidosis was based on clinical presentation, laboratory and chest radiographic findings, and a positive biopsy specimen and/or a BAL lymphocyte CD4/CD8 ratio of >3.5.9 In patients without a positive biopsy specimen in whom a BAL CD4/CD8 ratio was not obtained or was <3.5, sarcoidosis was diagnosed from the clinical appearance (all had Löfgren's syndrome). Patients were subdivided into two groups: HLA-DRB1*0301 positive (n=69) and HLA-DRB1*0301 negative (n=52). In the DRB1*0301 positive group three patients with biopsy proven sarcoidosis had no pulmonary involvement with normal chest radiographic findings and no respiratory symptoms (table 1). All subjects gave informed consent and the study was approved by the local ethics committee.
Clinical information on HLA-DRB1*0301+, DRB1*0301–/DRB3*0101–, and DRB1*0301–/DRB3*0101+ sarcoidosis patients
BAL procedure and handling of cells
Sterile saline solution (250 ml) at 37°C was instilled into a middle lobe bronchus in five aliquots of 50 ml. The fluid was gently aspirated after each instillation and collected in a siliconised bottle kept on ice. The BAL fluid was strained through Dacron nets and the cells were pelleted at 400g for 5 minutes at 4°C and resuspended in RPMI 1640 medium (Gibco, Paisley, UK). Paired peripheral blood mononuclear cells were separated from heparinised peripheral blood by Ficoll Hypaque (Pharmacia, Uppsala, Sweden) gradient centrifugation, washed twice in RPMI 1640 medium and diluted to appropriate concentrations.
Monoclonal antibodies, immunofluorescence and flow cytometry
Anti-TCR AV2S3 specific monoclonal antibodies were provided by T Cell Sciences Inc (Cambridge, MA, USA), and RPE-Cy5 conjugated anti-CD4 and FITC conjugated-F(ab`)2 fragments of rabbit anti-mouse Ig (secondary antibodies) were from Dako (Dakopatts A/S, Glostrup, Denmark). Normal mouse serum from Balb/c mice was used as a negative control at a dilution of 1:500 in PBS, in all cases staining <0.5% cells.
Cells were incubated with unlabelled TCR AV2S3 specific monoclonal antibody, washed twice, and FITC conjugated F(ab`)2 fragments of rabbit anti-mouse Ig were added for the detection of bound antibodies. Normal mouse serum diluted 1:500 was used to block remaining rabbit anti-mouse Ig before adding the RPE-Cy5 conjugated CD4 specific monoclonal antibody. Cells were analysed in a FACS-Calibur flow cytometer (Becton-Dickinson, Mountain View, CA, USA) using a Hewlett Packard 300 computer (Palo Alto, CA, USA). Lymphocytes were gated out by forward and side scatter and 5000–10 000 cells were analysed in each sample.
Lung restricted (AV2S3+) T cell expansion was defined as more than three times AV2S3+ CD4+ T cells in BAL fluid than in PBL or more than 10% AV2S3+ CD4+ T cells in BAL fluid with normal AV2S3 levels (3.5%10) in paired PBL samples.
HLA typing
HLA-DRB1 typing of all 121 individuals was performed on DNA using polymerase chain reaction (PCR) techniques and amplification with sequence specific primers. HLA-DRB3 alleles were determined in 78 patients where enough DNA was available (54 DRB1*0301 positive and 24 DRB1*0301 negative).11
Statistical analyses
The non-parametric Mann-Whitney U two-tailed test was used for calculating statistical significance.
RESULTS
TCR AV2S3 expression in DRB1*0301 positive and DRB1*0301 negative patients
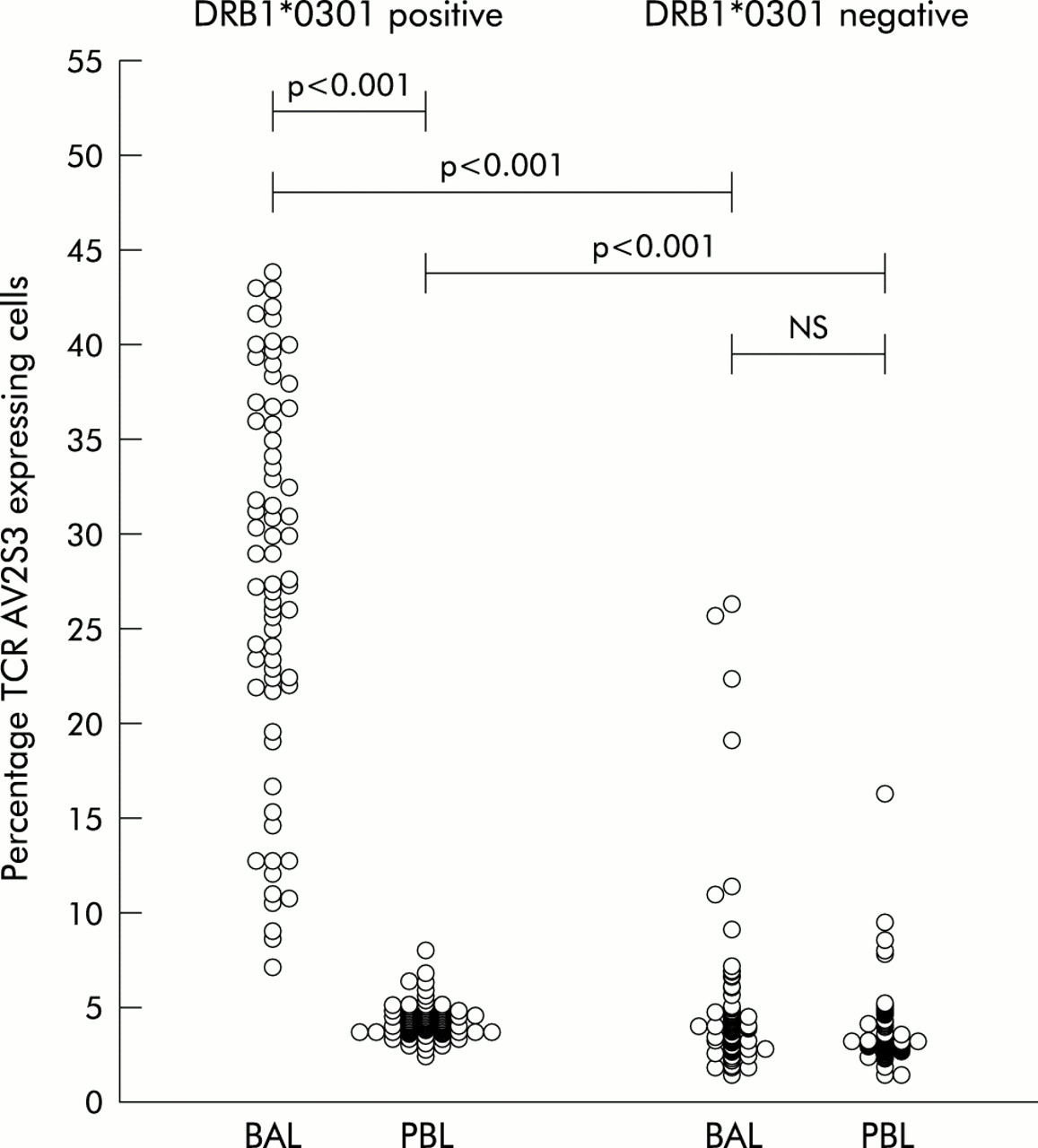
HLA-DRB1*0301 positive patients had greatly increased relative numbers of TCR AV2S3 expressing CD4+ BAL T cells, with AV2S3 expressed by a median of 27.6% (range 7.1–43.9%) of the CD4+ lung T cells compared with 4.3% (2.5–8.0%) in paired PBL samples (fig 1). This difference was highly significant (p<0.001). For HLA-DRB1*0301 negative patients, on the other hand, there was no difference in AV2S3 expression by CD4+ lymphocytes in BAL fluid (4.0%, range 1.5–26.3%) and PBL (3.3%, 1.5–16.4%; fig 1).

Relative numbers of CD4+ T cells expressing the TCR AV2S3 gene segment in bronchoalveolar lavage (BAL) fluid (n=69) and peripheral blood lymphocytes (PBL, n=62) of HLA-DRB1*0301 positive and HLA-DRB1*0301 negative sarcoidosis patients (n=52 for BAL fluid and n=43 for PBL).
As expected, the increased relative numbers of AV2S3+ CD4+ BAL cells in DRB1*0301 positive patients was much higher than those of DRB1*0301 negative patients (p<0.001; fig 1). A distinct lung restricted (AV2S3+) T cell expansion was identified in most DRB1*0301 positive patients (67 of 69), but only in six of 52 DRB1*0301 negative patients. The difference between CD4+ PBL expressing AV2S3 in DRB1*0301 positive patients (4.3%) and DRB1*0301 negative patients (3.3%) was also statistically significant (p<0.001; fig 1).
Individual TCR AV2S3 values in DRB1*0301 positive patients
In several cases more than 40% of the CD4+ lung T cells expressed AV2S3. The patients with higher values usually had an acute onset with Löfgren's syndrome. The two DRB1*0301 positive patients who did not fulfil the criteria for a AV2S3+ lung restricted T cell expansion, as well as several of the patients with lower numbers of AV2S3+ BAL T cells (less than 15%), had little or no clinical disease activity and in many cases a long duration from onset of disease to BAL cell analysis (more than 6 months). Three patients did not have pulmonary sarcoidosis, as judged from normal chest radiographs throughout the follow up period and no respiratory symptoms. However, they had positive biopsy specimens (skin or spleen) and, interestingly, all three also had AV2S3+ T cell expansions in the lung.
The DRB1*0301 allele is linked to the DRB3*0101 allele so that most DRB1*0301 positive individuals also carry the DRB3*0101 allele. However, we also identified DRB1*0301 positive patients with other DRB3 alleles (table 2). Fifty one of 54 DRB1*0301 positive patients classified for DRB3 carried the DRB3*0101 allele, while only three had the DRB3*0202 allele. Almost every DRB1*0301 positive patient had a distinct AV2S3+ lung T cell expansion, the exception being a patient carrying the common DRB3*0101 allele but with few signs of disease activity (table 2). Thus, in the DRB1*0301 positive group of patients there were dramatically increased numbers of AV2S3+ lung T cells regardless of the specificity of the associated DRB3 alleles.
HLA-DRB3 typing of DRB1*0301 positive (n=54) and DRB1*0301 negative (n=24) patients
Individual TCR AV2S3 values in DRB1*0301 negative patients
In the DRB1*0301 negative group of patients all but seven had normal AV2S3 values in BAL fluid. Of these seven patients, one also had an AV2S3+ T cell expansion in the PBL which is not typical of sarcoidosis and was therefore not classified as having a distinct lung restricted AV2S3+ CD4+ T cell expansion. However, six DRB1*0301 negative patients did have distinct lung restricted T cell expansion (figs 1 and 2).

{kind=link}
{kind=link}
Relative numbers of CD4+ T cells expressing the TCR AV2S3 gene segment in bronchoalveolar lavage (BAL) fluid and peripheral blood lymphocytes (PBL) of DRB1*0301 negative patients subgrouped into DRB3*0101 negative (n=46 for BAL fluid and n=39 for PBL) and DRB3*0101 positive (n=6 for BAL fluid and n=4 for PBL) patients. Solid circles indicate patients in whom DRB3 alleles were specified through genotyping (n=24); open circles indicate patients who were classified as DRB3*0101 negative because the DRB1 alleles are not associated with the DRB3*0101 allele in the Scandinavian population.
The HLA-DRB3 alleles were determined in 24 of the DRB1*0301 negative patients, including 14 patients positive for HLA-DR13, an allele known to be linked to the DRB3*0101 allele in a subgroup of white subjects. All six DRB1*0301 negative patients with a distinct AV2S3+ lung T cell expansion had the DRB3*0101 allele, while none of the other patients had this particular DRB3 allele (table 2, fig 2). Notably, in these six DRB1*0301 negative/DRB3*0101 positive patients, the four with the highest AV2S3+ BAL cell values all had Löfgren's syndrome. In the DRB1*0301 negative group of patients the lung restricted AV2S3+ T cell expansions were thus linked to the DRB3*0101 allele exclusively.
Pulmonary AV2S3+ T cell expansions were therefore found to be strongly linked to two separate subgroups of patients—those expressing either the DRB1*0301 or the DRB3*0101 alleles.
DISCUSSION
We have identified a new group of sarcoidosis patients with a particular HLA type (DRB1*0301 negative/DRB3*0101 positive) with lung restricted AV2S3+ CD4+ T cell expansions. We also found significantly increased levels of AV2S3+ CD4+ PBL T cells in DRB1*0301 positive versus negative patients, and confirmed the previously reported correlation between AV2S3+ CD4+ BAL T cell expansions and HLA-DRB1*0301.
In all six DRB1*0301 negative patients with the DRB3*0101 allele a distinct AV2S3+ T cell expansion was seen in BAL fluid. Apart from the patient with a parallel AV2S3+ T cell expansion in both BAL fluid and PBL, none of the remaining DRB1*0301 negative patients had an AV2S3+ BAL T cell expansion and none had the DRB3*0101 allele. This can be concluded, although not every patient was characterised for the DRB3 allele, since the HLA-DRB3*0101 allele is associated only with DRB1*0301 and some DRB1*13 and DRB1*14 alleles in Scandinavians, and all such patients were classified for DRB3. Interestingly, four of the six DRB1*0301 negative/DRB3*0101 positive patients had Löfgren's syndrome, which is rather unusual among DRB1*0301 negative patients but common in DRB1*0301 positive patients (table 1). These four patients also had the highest numbers of AV2S3+ BAL T cells. They therefore behaved clinically and immunologically like DRB1*0301 positive patients.
The HLA-DRB1*0301 and -DRB3*0101 molecules display interesting similarities, especially in regions important for antigen peptide binding. In particular, they uniquely share Tyr-26 and an Arg-74 located in the HLA β chain encoded β pleated sheet and the α helix, respectively. These amino acids are located close to each other and interact with the antigenic peptide amino acid at position 4. Experimentally, the unique Tyr-26 and Arg-74 combination has been shown to be important for the capacity to present similar antigenic peptides to T cell clones, and AchR derived peptides presented by DRB1*0301 and DRB3*0101 molecules required an Asp at this position (position 4).12
DRB3*0101 is expressed at lower levels than DRB1*0301,13 but is still clearly capable of presenting antigenic peptides to specific T cells.14 Interestingly, the less polymorphic DRB3 alleles could readily present bacterial heat shock proteins.14 Arg-74 was experimentally shown to be important for the binding and presentation of Mycobacterium tuberculosis derived HSP65 peptide p3–13.15 Our finding that patients expressing either HLA-DRB1*0301 or HLA-DRB3*0101 have lung restricted TCR AV2S3+ T cell expansions suggests that either of these HLA molecules can present sarcoidosis associated antigenic peptides that are specifically recognised by AV2S3+ T cells. In HLA-DRB1*0301 and HLA-DRB3*0101 negative patients the same antigen could hypothetically generate other peptides that are presented by other HLA molecules, thereby stimulating T cells with other specificities.
The suggestion of a specific sarcoidosis antigen is supported by epidemiological data, indicating an infectious agent that could be transmitted via close personal contact16,17 or upon transplantation.18 A work related risk for nurses and subjects living close to hospitals was reported,19 as well as a seasonal clustering of the disease.17 However, despite decades of intense search for any causative agent, no definitive proof has been presented.
Biased TCR V gene usage is generally considered to appear as a result of a previous immune reaction against a specific antigenic peptide, and the combination of particular peptides and MHC molecules are known to be able to stimulate T cells expressing selected TCRs. In autoimmune diseases where specific antigens may be involved in the pathogenesis, several reports have shown a preferential TCR V expression.20–23 However, in most human autoimmune diseases there has not been such a strong association between T cells expressing a particular V gene segment and a distinct HLA type as we have reported here. In fact, associations between HLA alleles and the expression of specific TCR V genes are rare and, in general, are considered rather weak.24 The uniqueness of our finding is further underlined by the local accumulation of the AV2S3+ T cells in the lungs—the organ most commonly affected in Scandinavian sarcoidosis patients. The magnitude of BAL AV2S3+ T cell expansions, which may be quite dramatic (>40% of BAL CD4+ T cells), correlates with certain clinical manifestations.8 Recently developed techniques, using MHC tetramers including the relevant antigenic peptide to stain antigen specific T cells, have indicated that very large populations of T cells can be antigen specific.25,26 In acute EBV infections such large antigen specific T cell populations used selective TCRs and were, in some cases, of the same magnitude as the ones described here, although they were CD8+ and not CD4+ as in sarcoidosis.27
It was interesting to find lung accumulated AV2S3 expressing T cells also in three DRB1*0301 positive patients without any signs of respiratory disease. A presumed sarcoidosis associated antigen may initially be restricted to the lungs, either through inhalation or by a lung specific expression of an autoantigen or an antigen derived from a microbial infection. The locally generated immune response, resulting in proliferation of AV2S3+ T cells, could speculatively inhibit lung manifestations of the disease in a few individuals. We previously reported a positive correlation between the numbers of lung AV2S3+ T cells and short disease duration, indicating a protective role for these particular T cells.8 Some of the lung accumulated antigen specific AV2S3+ T cells may also “spill over” and escape into the circulation, in line with results of our previous sequence analyses of the TCR α chains of AV2S3 expressing BAL and PBL T cells where we occasionally found identical T cell clones in both BAL fluid and PBL of the same patient (data not shown).7 In this regard, lymphocytes have been shown experimentally to be capable of returning to the peripheral blood from the alveolar space.28 Our finding of levels of peripheral blood AV2S3 expressing T cells which were significantly higher than normal but lower than in BAL fluid in DRB1*0301 positive compared with DRB1*0301 negative patients indicates an immune response that is concentrated but not restricted to the lungs and emphasises the systemic nature of the disease. Alternatively, DRB1*0301 positive individuals could have a genetic constitution that favours the selection of AV2S3+ T cells.
In conclusion, we have described an exceptional correlation between lung CD4+ T cell expansions expressing TCR AV2S3 and the two functionally and structurally closely related HLA-DRB1*0301 and HLA-DRB3*0101 molecules. We suggest that a presumed sarcoidosis associated antigen could be presented by either of these two HLA-DR molecules, leading to the preferential stimulation of AV2S3 expressing T cells in Scandinavian patients with sarcoidosis. This observation may help in elucidating the pathogenesis of the disease.
Acknowledgments
The authors thank Ms Margitha Dahl, Ms Gunnel de Forest, and Mrs Kia Katchar for their contributions. This study was supported by grants from the Swedish Heart Lung Foundation, King Oscar II Jubilee Foundation, the Swedish Medical Research Council (12621, 10393 and 11953), the Swedish Society of Medicine, the Swedish Cancer Society, and Karolinska Institutet.