Article Text

Abstract
Background: Passive training of specific locomotor muscle groups by means of neuromuscular electrical stimulation (NMES) might be better tolerated than whole body exercise in patients with severe chronic obstructive pulmonary disease (COPD). It was hypothesised that this novel strategy would be particularly effective in improving functional impairment and the consequent disability which characterises patients with end stage COPD.
Methods: Fifteen patients with advanced COPD (nine men) were randomly assigned to either a home based 6 week quadriceps femoris NMES training programme (group 1, n=9, FEV1=38.0 (9.6)% of predicted) or a 6 week control period before receiving NMES (group 2, n=6, FEV1=39.5 (13.3)% of predicted). Knee extensor strength and endurance, whole body exercise capacity, and health related quality of life (Chronic Respiratory Disease Questionnaire, CRDQ) were assessed.
Results: All patients were able to complete the NMES training programme successfully, even in the presence of exacerbations (n=4). Training was associated with significant improvements in muscle function, maximal and endurance exercise tolerance, and the dyspnoea domain of the CRDQ (p<0.05). Improvements in muscle performance and exercise capacity after NMES correlated well with a reduction in perception of leg effort corrected for exercise intensity (p<0.01).
Conclusions: For severely disabled COPD patients with incapacitating dyspnoea, short term electrical stimulation of selected lower limb muscles involved in ambulation can improve muscle strength and endurance, whole body exercise tolerance, and breathlessness during activities of daily living.
- neuromuscular electrical stimulation
- chronic obstructive pulmonary disease
- pulmonary rehabilitation
Statistics from Altmetric.com
Exercise intolerance is a hallmark of chronic obstructive pulmonary disease (COPD) and is commonly associated with reduced quality of life and increased utilisation of healthcare resources.1 Traditionally, exercise intolerance has been ascribed to respiratory mechanical and/or pulmonary gas exchange disturbances and their perceptual consequences which are manifest mainly as breathlessness (dyspnoea), especially on exertion.2
It is increasingly clear, however, that a chronic progressively sedentary lifestyle generally ensues, a process long recognised as the “dyspnoea spiral”.3 Evidence has accumulated to suggest that, as part of this vicious cycle, deconditioning of skeletal muscle occurs which contributes significantly to exercise intolerance in this patient population.4–7 Exercise training, typically as a component of pulmonary rehabilitation, has been shown to improve exercise tolerance in COPD.8 However, physical training of very severe patients, such as those who present with intense breathlessness at rest or on minimum exertion, can be particularly difficult. In this population, training has been shown to be associated with less consistent benefits than those characteristically found in patients with mild to moderate dyspnoea.9,10
We therefore propose that passive stimulation of locomotor muscle groups by neuromuscular electrical stimulation (NMES) may provide an alternative approach for improving physical capacity in severely compromised patients with COPD who present with incapacitating dyspnoea. Application of NMES has been consistently associated with increased mass, strength, and endurance of both normally and abnormally innervated muscles in a range of pathological conditions.11–13 Although experience with NMES in patients with skeletal muscle dysfunction secondary to congestive heart failure is accruing,14–17 the efficacy of this technique has yet to explored in COPD.
Using a randomised controlled trial, the objective of the present investigation was therefore to evaluate the potential for NMES to improve peripheral muscle function, and to evaluate the impact of any such changes on exercise tolerance and health related quality of life of patients with advanced COPD.
METHODS
Patients
Fifteen patients (nine men) with a clinical and functional diagnosis of COPD comprised the study group. All subjects presented with moderate to severe ventilatory impairment (forced expiratory volume in 1 second (FEV1) <50% predicted) and incapacitating breathlessness according to the Medical Research Council scale18—that is, scores of 4 (“I stop for breath after walking 100 yards or after a few minutes on the level”) or 5 (“I am too breathless to leave the house”). Inclusion criteria were absence of associated locomotor or neurological conditions, and disease stability as indicated by no change in medication dosage or exacerbation of symptoms in the preceding 4 weeks.
Before participating in the study all the procedures and any associated risks were described in detail to the patients. Written informed consent (as approved by the institutional medical ethics committee) was then obtained from each patient.
Design and procedures
This was a prospective randomised controlled study. The patients were referred from the respiratory clinic of Hairmyres Hospital by two investigators who were blind to the order of patient allocation. Patients were randomised to group 1 who initially received NMES (n=9) or to group 2 who received NMES after a control period (n=6). Group 1 was evaluated twice (before and after NMES) and group 2 was assessed three times (before and after the 6 week control period and after a further 6 week period of NMES). The NMES training period was consistent with the training duration shown to be effective in previous studies of NMES.11,12,15,17
Each evaluation consisted of a 3 day protocol which included: (1) a questionnaire based evaluation of the health related quality of life, body composition assessment, pulmonary function tests, and a maximum incremental cardiopulmonary exercise test (CPET) (day 1); (2) a knee strength and endurance evaluation by isokinetic dynamometry (day 2); and (3) an endurance constant work rate CPET to the limit of tolerance (day 3).
Measurements
Health related quality of life
The Chronic Respiratory Questionnaire19 was administered to obtain an index of the health related quality of life. In this instrument four domains are measured: “dyspnoea” (using self-selected daily activities), “fatigue”, “mastery”, and “emotional function”. Each domain has 4–7 items scored on a scale of 1–7. A change of 0.5 in the arithmetic mean score per domain has been shown to be related to a minimally important difference in general health status.19
Body composition
Fat-free mass (FFM) was measured by the bioelectrical impedance method (Bodystat-500; Bodystat Ltd, Douglas, UK). Impedance measurements were performed on the right side with subjects supine and with their limbs slightly apart from the trunk. FFM was calculated using a validated patient specific regression equation20 from Ht2/Res and total body mass and expressed as a percentage of ideal body weight.
Pulmonary function tests
Spirometric tests were performed using the 2130D SensorMedics spirometer (SensorMedics Corp, CA, USA), flow being measured with a calibrated pneumotachograph. The subjects completed at least three acceptable maximal forced expiratory manoeuvres before and 20 minutes after 200 μg inhaled salbutamol. Maximal voluntary ventilation (MVV, l/min) was estimated from the product FEV1 (l) × 37.5. A computer based automated system (VMax 22 System, SensorMedics Corp) was used to measure static lung volumes by the “breath by breath” nitrogen washout technique and lung diffusion capacity for carbon monoxide (transfer factor) by the modified Krogh technique (single breath).
Cardiopulmonary exercise tests
Exercise tests were performed on an electromagnetically braked cycle ergometer with the subjects maintaining a pedalling frequency of 50 (5) rpm. Each subject initially underwent a symptom limited incremental exercise test (5 W/min). On a different day each subject completed a constant work rate test to the limit of tolerance (Tlim), with the work rate being maintained constant at 80–90% of the peak work rate obtained in the incremental test.21
During the exercise tests respired O2 and CO2 concentrations and respired flow were monitored continuously by calibrated rapidly responding gas analysers and an anemometer, respectively (VMax 229 System, SensorMedics Corp). Pulmonary oxygen uptake (V̇o2, l/min STPD) and minute ventilation (V̇e, l/min BTPS) were derived breath by breath and expressed as 15 s stationary averages. Heart rate (HR, bpm) was derived beat by beat using the R–R interval from a 12-lead electrocardiogram, and oxyhaemoglobin saturation (Sao2) by pulse oximetry. Subjects were also asked to rate “shortness of breath” or “leg effort” each minute in an alternating sequence using the Borg category ratio scale (0–10). The peak V̇o2 values on the incremental test were compared with those predicted by Neder et al, taking into consideration sedentariness, sex, age, weight, and height.22
Peripheral muscle strength and endurance
Concentric contractions of the quadriceps femoris (knee extension) of the dominant leg were evaluated using an isokinetic dynamometer (KinCom, Cybex, Chattanooga, NY, USA).23 All patients performed: (1) a maximum isokinetic strength test with three movements tested at an angular velocity of 70°/s separated by 1–3 minutes rest (peak torque in N.m); (2) a maximal isometric test in which the subjects were asked to sustain the lever arm at 40° for 5 seconds while the force applied was instantaneously recorded (mean force in N); and (3) an endurance test for 1 minute in which the subjects were asked to perform the maximum possible number of contractions at an angular velocity of 70°/s during this time frame (total work in J, mean power in W, and a fatigue index expressed as the % ratio between the work performed in the three last and three initial contractions).
Training protocol
The NMES training protocol used was based on that of Kots,24 later modified by Selkowitz.25 A portable, user friendly, dual channel NME stimulator was used (Respond Select, Empi Inc, South Dakota, USA). The following training protocol was chosen in order to minimise the effects of fatigue on muscle contractility:
-
symmetrical biphasic square pulsed current at 50 Hz;
-
duty cycle: 2 s on and 18 s off (10%) in the first week, 5 s on and 25 s off (17%) in the second week, and 10 s on and 30 s off (25%) thereafter;
-
pulses 300–400 μs wider using the highest tolerable amplitude (10–20 mA at the start of the training session increasing up to 100 mA).
This training protocol was applied in each leg (15 minutes in the first week and 30 minutes thereafter), in sequence, five times per week for 6 weeks (a total of 30 sessions). During the NMES application the patient's back was fully supported but the limb receiving treatment was left hanging unsupported.
In order to familiarise the patients with the equipment and to detect possible side effects, the NMES training protocol was initially applied under the guidance of a qualified and experienced physiotherapist in an outpatient hospital setting (first week). A “user diary” was completed daily in the home based training phase to include the patient's subjective impressions during and between the training sessions. In addition, the same physiotherapist responsible for the training assessed compliance at a weekly visit to the patient's home, during which she adjusted the stimulator settings and checked a hidden system recording clock which recorded cumulative time of usage.
Statistical analysis
Mean (SD) values were obtained for subjects in both groups. Between group differences at baseline and after 6 weeks were assessed by an unpaired Student's t test; mean differences and their 95% confidence intervals are reported for the main outcomes. In addition, the data following NMES in patients in group 2 were compared with baseline values using a paired t test. Product-moment correlation (Pearson) was used to define the associations between variables. The probability of a type I error was established at 0.05 for all tests.
RESULTS
Baseline characteristics
No significant differences were found between the groups in anthropometric and lung function variables at baseline (table 1). The tolerance to incremental cycle ergometric tests was severely reduced in both groups relative to predicted values (table 2).22
Anthropometric and lung function characteristics at baseline
Whole body exercise tolerance and peripheral muscle strength in patients who received NMES (group 1, n=9) and controls (group 2, n=6)
Although breathlessness was the main limiting symptom to incremental exercise (median 7 (range 4–10)), leg effort was also an important contributory factor for all patients (5 (3–9)). Both groups had marked reductions in muscle strength and endurance—for example, peak torque was only 55.8 (20.5)% predicted in group 1 and 61.3 (15.7)% predicted in group 2.26
Physiological and subjective effects of NMES
All patients were able to complete the training sessions successfully. Compliance was excellent: all patients completed their diaries fully and the hidden clock system confirmed that the NMES system was used for the expected period. While four patients (two in each group) presented with mild exacerbations of COPD during the training period, they were able to continue the NMES training safely during these events. There were no reports in the patients' diaries of any side effects of NMES, such as pain or discomfort.
Peripheral muscle strength and endurance
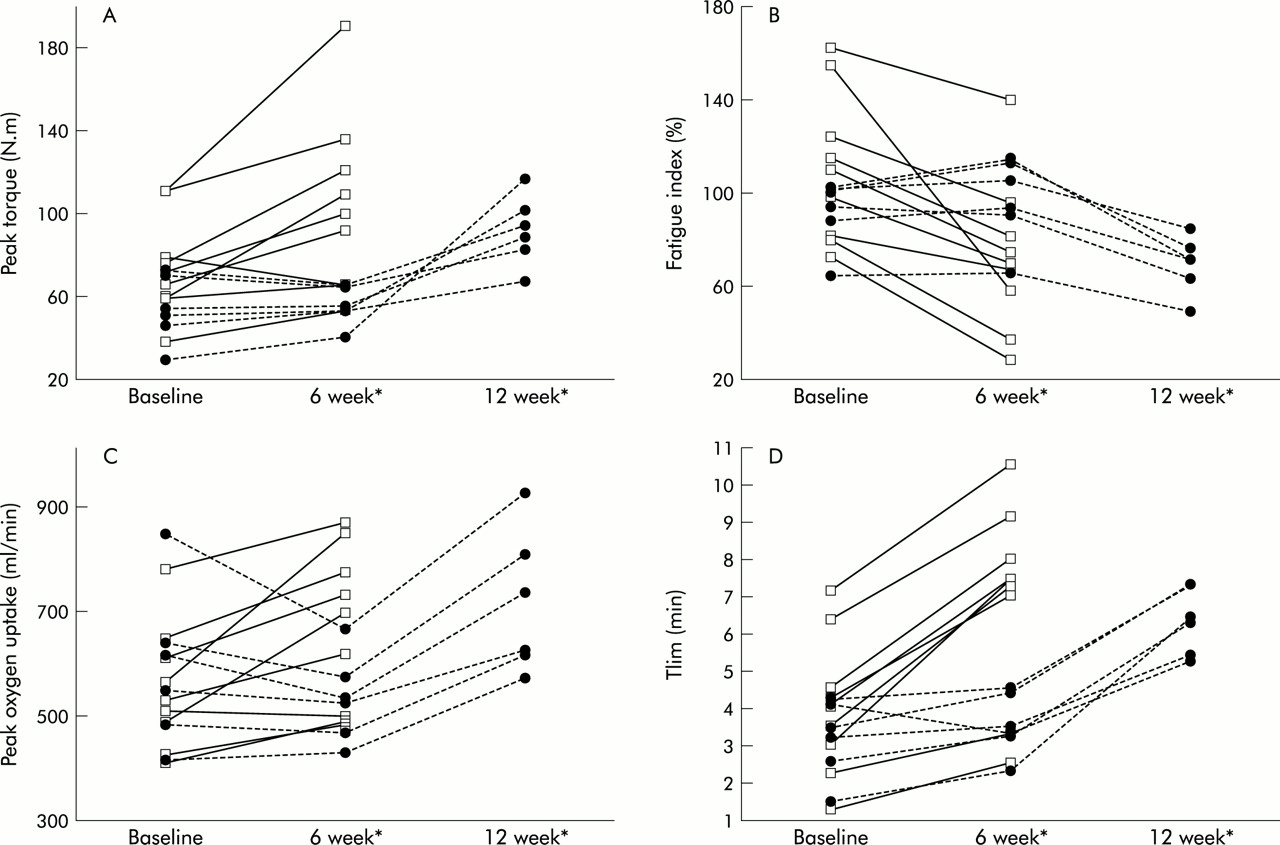
Significant mean differences in maximal isokinetic strength (peak torque) and muscle fatigue were found between the two groups (table 2 and fig 1 A and B). Although we did find trends for improvement after NMES in isometric mean force and other indices of muscle endurance such as total work and mean power, they did not reach statistical significance (p>0.05). Peak torque and muscle fatigue after NMES in patients in group 2 were also significantly higher than those found at baseline (fig 1A and B).

{kind=link}
Individual values for (A) maximal knee isokinetic strength (peak torque), (B) endurance (fatigue index), (C) maximum (peak oxygen uptake), and (D) endurance (time, Tlim) exercise capacities at baseline and 6 and 12 weeks. Note that while patients in group 1 (n=9, solid lines) received NMES after enrolment, those in group 2 (n=6, dashed lines) were submitted to a control period before receiving NMES. *p<0.05 for all variables (group 1 v group 2 after 6 weeks and in group 2 at 12 weeks v baseline).
Whole body incremental and endurance exercise
Application of NMES was associated with an enhanced tolerance to whole body incremental exercise, as inferred from symptom limited peak V̇o2 and endurance exercise (table 2 and fig 1C and D). The most striking effects, however, were found in the endurance capacity: the percentage increase ((post – pre)/pre × 100) in Tlim following NMES training was substantially larger than that for peak V̇o2 (84.5 (21.3)% v 16.3 (8.1)%; p<0.01). Similarly, values for peak V̇o2 and Tlim were significantly higher after NMES than at baseline in patients in group 2 (fig 1C and D)
Health related quality of life
NMES training was associated with beneficial changes in the “dyspnoea” domain of the quality of life questionnaire19 with a mean difference between groups 1 and 2 after 6 weeks of 1.2 (95% CI 0.4 to 2.0). No between group differences were observed in “fatigue”, “emotional function”, and “mastery” domains. In addition, in group 2 the mean scores for dyspnoea after NMES were significantly improved compared with baseline (mean difference 1.4 (95% CI 0.5 to 2.3); p<0.05).
Correlates of improvement after NMES
No significant relationship was found between the magnitude of training related improvement and the resting or exercise baseline data. However, improvements in muscle function (peak torque) and exercise tolerance (Tlim) correlated significantly with reduced leg effort adjusted for post-training changes in exercise duration (constant work rate test) (R = –0.77 and –0.74, respectively; p<0.01).
DISCUSSION
This study constitutes, we believe, the first description of the effects of NMES on peripheral muscle function, whole body exercise tolerance, and health related quality of life in patients with advanced COPD. Using a 6 week home based NMES training programme, we were able to enhance patients' functional capacity which was reflected in an improvement in self-reported daily dyspnoea. These preliminary findings suggest that NMES can be a safe and effective strategy for rehabilitating patients with severe COPD who present with incapacitating breathlessness.
The major advantage of NMES over conventional exercise training in patients with COPD is the virtual absence of ventilatory stress during passive exercise, reflecting the smaller muscle mass involved. Our patients were therefore comfortably able to cope with a training regimen which, if provided by voluntary dynamic contractions, would be demanding and probably not tolerable. In fact, from the patients' diaries there was a consistent view that the associated sensations were not painful or uncomfortable, which emphasises the importance of including some days of familiarisation and a progressive training scheme. In this context, we also found that four patients were able to maintain their NMES training even in the presence of an acute exacerbation. This finding raises the hypothesis that NMES could be valuable for ameliorating the marked decrease in muscle strength (and mass) which is frequently observed following acute exacerbations of COPD.27
Our data are consistent with growing evidence that NMES can be safely and effectively used in patients with skeletal muscle function deficit and exercise intolerance secondary to systemic diseases.14–17 Quittan et al, for example, have described substantial gains in muscle strength and exercise tolerance after NMES in patients with congestive heart failure which has been confirmed by others.14–17 These positive effects of NMES are likely to be similar to those morphological changes described by Maltais and colleagues9 in patients with COPD who were submitted to conventional endurance training. Using a comprehensive range of outcome measures, our study showed a reduction in leg effort for a given level of exercise after NMES training (table 2) which would be consistent with this view. Further morphological studies after NMES training, however, will be required to confirm this hypothesis.
It is also interesting to note that the beneficial changes in muscle function found in this study could be translated into more general benefit. A recent position statement on pulmonary rehabilitation28 recommends assessment of the efficacy of treatment using the World Health Organisation's description29 of illness impact across three domains—impairment (skeletal muscle function), activity limitation (exercise tolerance), and participation restriction (chronic dyspnoea)—and our NMES training programme achieved improvements in all of them.
The major limitation of this study relates to its small sample size. It is likely that the study lacked statistical power to unravel the full benefits of the intervention. In fact, several of the outcomes failed to reach statistical significance despite clear trends towards improvement: this was particularly true for some indices of muscle endurance and, interestingly, the amount of breathlessness corrected for exercise intensity (table 2). In this context, the study should be viewed as an initial investigation of the feasibility and short term efficacy of NMES. Further randomised controlled trials using larger samples with a longer follow up period are clearly warranted.
We were also not able to re-evaluate patients in group 1 after NMES—that is, this was not a true crossover study. We considered it unethical to submit these frail patients to an additional period of physical detraining followed by a demanding period of retesting, but offered all patients access to our formal pulmonary rehabilitation programme on completion of active NMES treatment on the basis that any improvement, if our hypothesis was correct, should be consolidated. In addition, it would be interesting to compare NMES alone or in addition to mild resistive (weight) training30 with conventional rehabilitation programmes, particularly in this specific group of severe patients. Furthermore, a formal cost effectiveness analysis is necessary before the widespread use of NMES can be recommended. Our initial impression of the cost outlay per patient device is encouraging: reliable, robust stimulators are currently commercially available for £200–300 and, once issues of bulk purchase are taken into account, this figure could perhaps be reduced further.
In conclusion, a 6 week home based neuromuscular electrical stimulation programme has been shown to improve some markers of skeletal muscle strength and endurance in patients with severe COPD. These beneficial effects on peripheral muscle function were translated into an improved ability to perform whole body exercise and were associated with reduced breathlessness on the activities of daily living. These preliminary findings need to be confirmed by larger randomised controlled trials.
Acknowledgments
The authors are grateful to Mrs J Sullivan, K Fife, D MacFarlane, and I Johnson (Department of Respiratory Medicine, Hairmyres Hospital) for their skilful technical assistance.
REFERENCES
Footnotes
-
J A Neder was supported by a long term Research Fellowship Grant from the European Respiratory Society.