Article Text

Abstract
Background: Mandibular advancement devices (MADs) can successfully control both snoring and obstructive sleep apnoea (OSA). Many patients on nasal continuous positive airway pressure (NCPAP) for OSA would like a more portable alternative, even if only temporarily. This study assesses what proportion of patients with OSA already on NCPAP can successfully use a MAD for short periods (up to 1 month) as a temporary alternative to NCPAP.
Methods: Fifty patients with OSA, already on NCPAP for at least 3 months, were recruited by invitation. They were provided with a simple fixed MAD estimated to provide 75% of maximum mandibular protrusion. Sleep studies using a portable home recorder were performed on and after three nights without NCPAP to provide control data. Following acclimatisation to the MAD, sleep studies were also planned after 3, 7, and 28 days while using the MAD. If their overnight >4% Sao2 dips per hour deteriorated to >20 or the Epworth sleepiness score (ESS) rose to >9 (or increased by >4 over baseline) on nights 3 or 7, they were then deemed to have failed the trial and were withdrawn.
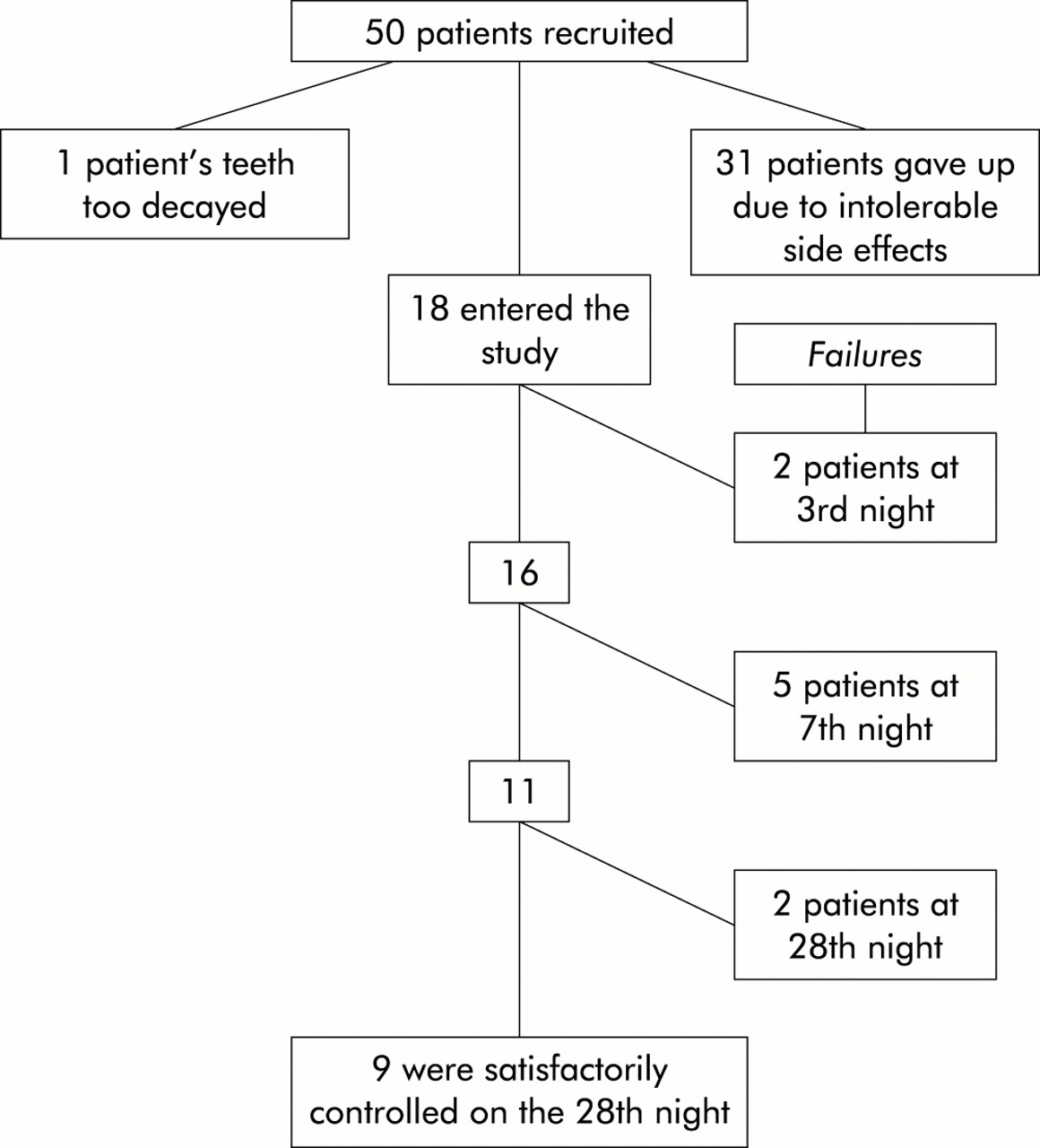
Results: Of the 50 patients entered, one had inadequate teeth for a MAD and 31 gave up trying to use the device during the acclimatisation period because of side effects. Of the 18 prepared to use the device, two patients failed at night 3, five at night 7, and two at night 28. Thus, nine patients remained controlled by our criteria at night 28. On average, sleep study indices while using the MAD were poor compared with the night on NCPAP.
Conclusions: Simple MADs are poorly tolerated by patients with OSA already on NCPAP. OSA was adequately controlled by our criteria in 32% of those recruited for the equivalent of a weekend, in 22% for 1 week, and in 18% for up to 1 month. Better tolerated devices would be likely to improve on these figures.
- obstructive sleep apnoea
- mandibular advancement devices
- nasal continuous positive airway pressure
Statistics from Altmetric.com
Mandibular advancement devices (MADs) have been used successfully to control both snoring1 and obstructive sleep apnoea (OSA).2 It is assumed that they work by increasing the volume of the pharynx and rendering it less collapsible during sleep.3 It is clear they do not work for all patients, and are probably more successful for less obese patients with milder disease.4 There are many patients with OSA on nasal continuous positive airway pressure (NCPAP) who find their treatment inconvenient while away from home who would like a more portable alternative, even if only temporarily.
The purpose of this study was to assess what proportion of a group of patients with OSA already on NCPAP could successfully use a MAD for short periods (up to 1 month) as a temporary alternative to NCPAP.
METHODS
Patients
To be eligible for the study patients needed to have been on NCPAP for at least 3 months, to have an average NCPAP compliance of >4 hours per night, a pretreatment Epworth sleepiness score (ESS) of ≥10, a diagnostic pretreatment rate of >4% dips in oxygen saturation (Sao2) overnight of >15/hour, and to have sound teeth. Patients were recruited by invitation from the NCPAP follow up clinic and via the patients' association quarterly newsletter. Characteristics of the patients included in the study are shown in table 1.
Baseline data on the 50 patients entering the study
Techniques
Sleep studies
Sleep studies were performed in the subjects' own homes using RM50 portable monitors (DeVilbiss, London, UK). These devices record for 8 hours and can be programmed to turn on and off at particular times (usually 23.00 and 07.00 hours, respectively). The RM50 records oxygen saturation from a finger probe, snoring via a throat microphone, body position via a sensor in a chest box (held on by one chest band), chest movements, heart rate (from three ECG electrodes), and pulse transit time (PTT). The latter is the time delay between the ECG R wave and the arrival of the pulse wave at the finger detected from the transmittance signal of the oximeter probe. This value is typically about 250 ms and varies inversely with blood pressure. As the blood pressure falls, tension in the arterial wall falls and PTT increases, and vice versa.
Beat to beat measures of PTT therefore provide an estimate of the beat to beat changes in blood pressure5,6 that occur both during every inspiratory effort (pulsus paradoxus)7 and following a transient arousal from sleep.8 By chance, a change of 1 ms is about equivalent to a change of 1 mm Hg in blood pressure. It has been shown that respiratory swings in PTT quantitatively reflect swings in oesophageal pressure,9,10 and that falls in PTT over a slower time course of 20 s or so reflect the rise in bllod pressure following arousing stimuli, even when there are no discernible changes on the EEG (so called “subcortical arousals”).11
Analysis of the RM50 signals thus provided the following derivatives: number of >4% dips in Sao2 per hour of the study,12 number of rises in blood pressure per hour of the study,11,13,14,15 and the mean fall in blood pressure due to each inspiration (pulsus paradoxus) across the whole study.9,10,16,17 The units for the latter are in milliseconds and the overnight mean could represent up to 7000 or more breaths.
Previous work from this unit to assess the reproducibility of these two PTT derivatives compared two separate overnight recordings in 40 adult patients with a wide range of severity of sleep disordered breathing. Both “blood pressure arousals” and mean all night inspiratory effort showed good reproducibility with correlation coefficients between nights 1 and 2 of 0.81 and 0.87, respectively.15
Epworth sleepiness score
The Epworth sleepiness score (ESS) is the most widely used subjective index to quantify sleepiness.18 It consists of eight questions about the tendency to fall asleep in situations of differing stimulation such as watching television or talking to someone. Each question is scored 0, 1, 2, or 3 indicating an increasing tendency to fall asleep in each situation; the total score can thus vary from 0 (no sleepiness) to 24 (extremely sleepy) with 9 being the upper limit of normal.19 Previous uncontrolled studies have shown that this index improves significantly following NCPAP for OSA.20 The ESS is designed to assess sleepiness retrospectively over a period of time “in recent times”. When using the questionnaire to assess sleepiness over a shorter period, the patients were asked to confine their rating to this shorter period.
Mandibular advancement device
The mandibular advancement device used in this study essentially consists of two customised sports-type mouth guards (one for the top teeth and one for the bottom teeth) fused together in such a way that, when the appliance is bitten into, the mandible is held passively in a protruded position.1 Construction of the appliance requires upper and lower dental impressions from which plaster models are cast. A wax interocclusal record is taken with the patient posturing the lower jaw forward to about 75% of the maximum possible. Thermoplastic polyvinyl acetate/polyethylene blanks are moulded onto the models and trimmed. The models are then placed on a dental articulator in the previously recorded protrusive relationship and the upper and lower parts of the device are heat sealed together in this position. Finally, this bond is reinforced by heat moulding a thin layer of the thermoplastic material over the inner and outer surfaces. Both the clinical and laboratory stages of construction are straightforward, using inexpensive materials and widely available techniques.
Protocol
Following recruitment, patients were seen by one of two dentists (at no cost to themselves) for the dental impressions required for the MAD. Following construction, they were fitted at a second visit or occasionally they were sent directly to the patient and a second appointment was organised only if necessary and by patient request. Patients were then given as long as necessary to acclimatise to wearing their MAD overnight at home. During this acclimatisation period one home sleep study was performed on NCPAP. If they were happy to continue they were randomised to one of two pathways: MAD trial followed by an assessment of OSA severity off all treatment for three nights or vice versa. During the trial of MAD usage an assessment was made after each sleep study (at 3, 7, and 28 days) as to whether or not the device was successfully controlling the patient's OSA. This is necessarily arbitrary and the following criteria were used to define continuing control: >4% Sao2 dip rate ≤20 per hour; ESS <10 (or not increased by >4 over baseline). If these criteria were not met, the patient was withdrawn and the MAD deemed to have failed at that particular time interval.
RESULTS
Figure 1 is a flow diagram showing the outcomes stage by stage. Despite our assessment of sound teeth, the dentist disagreed in one patient. Thirty one subjects (62%) gave up because of intolerable side effects which included excessive salivation, sore gums, and painful masseter muscles or temporomandibular joints. Patients were often unwilling to persevere because they felt insecure without their NCPAP machines, having lack of faith in the efficacy of the MAD. In 32% of patients their OSA and symptoms were controlled for the equivalent of a weekend, in 22% for up to 1 week, and in 18% for up to 1 month. If these data are quoted for the 18 patients able to tolerate the MAD, then 89% were controlled for a weekend, 61% for 1 week, and 50% for up to 1 month.
{kind=link}
Flow diagram of patients entered into the study.
Control data when on and off NCPAP are shown in table 2 (columns 2 and 3). On NCPAP the results were normal and the PTT derivatives (arousals and inspiratory effort) were in the normal range established in earlier studies.21,22 After no treatment for 3 nights there was a clear deterioration in all measures, even after such a short time; these latter data were only available in 34 of the original 50 as some patients declined to be studied further when they realised they were not going to be able to tolerate the MAD. Data at each of the stages while using the MAD are shown in in table 2 (columns 4, 5 and 6), including the results for the patients subsequently withdrawn when they failed to fulfil the criteria for continuing control of their OSA (two on night 3, five on night 7). Despite control of OSA symptoms and only a slightly raised >4% Sao2 dip rate, the arousal index and measure of inspiratory effort were considerably worse than during treatment with NCPAP, approaching the severity when on no treatment.
Mean (SD) ESS and sleep data when on and off NCPAP and at each stage during MAD usage
DISCUSSION
This study has shown that simple MADs can replace NCPAP and “control” OSA for short periods of time in some patients. The acceptance rate was poor and in over 60% the cost of the device was essentially wasted. Most of the patients acclimatising to the device found it useful for a weekend, and many for longer. In the UK the cost of these devices is about £200, so the effective cost per patient able to use a device is nearer £600. The cost is therefore more than the original NCPAP machine.
The definition of “control” is, of necessity, arbitrary. Had we set higher or lower criteria to define control, then our percentage success rates would have been altered accordingly. The definition we used was a pragmatic one, agreed by several staff working with patients with OSA, and seemed to accord with the patients' view of control. It is interesting that, despite apparently keeping the ESS and Sao2 dip rate down, these devices were far less successful at controlling sleep fragmentation (as measured by transient blood pressure rises via PTT) and inspiratory effort (as measured by respiratory blood pressure swings via PTT). This would suggest that MADs are only partially controlling the upper airway obstruction and perhaps are converting apnoeas to “upper airway resistance events”.
The use of MADs has been explored as a treatment for snoring in the absence of sleep apnoea, and there are controlled data to show that they clearly work.1 In OSA their success is somewhat less and variable. For example, the Vancouver group23 studied 24 patients with mild to moderate OSA, comparing an adjustable MAD with NCPAP (4 months each) in a randomised crossover design. The mean apnoea/hypopnoea index (AHI) was about 25 and fell to 4 on NCPAP but only to 14 with the MAD. Furthermore, some patients derived no benefit or even deteriorated using a MAD, whereas all improved on NCPAP. Despite the superior physiological improvement from NCPAP, there was greater improvement in subjective sleepiness using the MADs and more patients preferred them. Half of the patients were, of course, started on the MAD first, rather than having already been established successfully on NCPAP for a period of time, as in our study. There were no variables such as cephalometric measurements that predicted a better response to the MAD.
Our low acceptance rate was disappointing and may have been due to a variety of reasons. Had we used adjustable devices, with a gradual increase in the degree of protrusion, we might have avoided some of the unpleasant side effects. However, there is no good evidence that this is so. Our device covers the teeth and gums to spread the load, but this encourages gum discomfort and there are MADs that only clip onto the teeth. Again, there is no work available to suggest the superiority of one type of device over another. In a recent questionnaire survey of the long term usage of carefully fitted adjustable MADs (Silensor and Herbst appliances) on an intention to treat basis, only 47 of 166 (28%) were using it every night, and only 69 (42%) were using it “at least once a week”.24 Our own view from talking to patients was that, although they were keen to try an alternative to NCPAP, when they actually tried to come off it they felt insecure and were aware of sleeping badly. Had they been introduced to the MAD before NCPAP, the outcome might have been different. Whatever the reason, the eventual success rate was not as good as we had hoped. Given the simplicity of the device used, it is likely that our results represent a “worst case” scenario with more modern devices perhaps likely to achieve greater success. These data have at least allowed us to inform patients currently on NCPAP of the approximate success rate should they choose to try a MAD as an alternative.
Acknowledgments
The authors thank Jill Adam and Paul Fuller, the two dentists who made all the MADs for our patients. The Sleep Apnoea Trust supported the study through the purchase of the MADs.