Article Text

Statistics from Altmetric.com
We read with interest the recent paper by Blasi et al which showed that Chlamydia pneumoniae infection is associated with higher rates of exacerbation and airway microbial colonisation in patients with COPD.1 We have prospectively studied patients in the East London COPD study with daily monitoring using diary cards to detect COPD exacerbation defined using the same criteria.2,3 Serum microimmunofluorescence (MIF) immunoglobulin G (IgG) titres for C pneumoniae were measured in 110 patients (FEV1% 41.7 (18.4)) with stable COPD during 1 year with simultaneous estimation of plasma fibrinogen and serum interleukin 6 (IL-6); 26% of the patients had IgG titres of ≥1 in 16 (fig 1). High C pneumoniae IgG titres were not related to FEV1 % predicted, exacerbation frequency, plasma fibrinogen, or serum IL-6 levels. In their paper Blasi et al did not report whether there was a relation between MIF titres and exacerbation frequency.
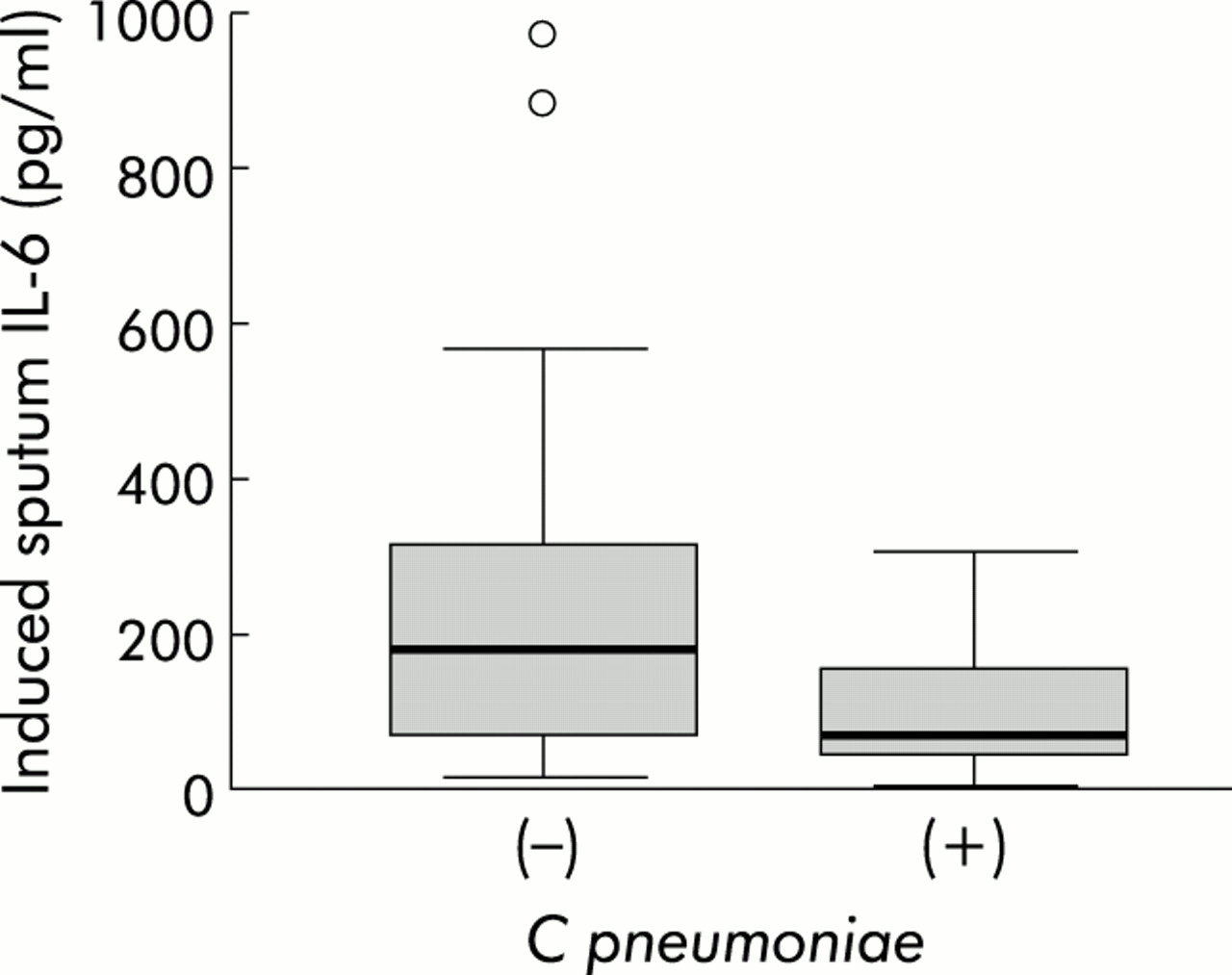
Blasi and colleagues found that 43% of patients when stable were positive for C pneumoniae by DNA polymerase chain reaction (PCR) using peripheral blood mononuclear cells (PBMCs). At exacerbation they have only shown data for the 34 (of 61) who consented to the antibiotic trial and all 34 were positive for C pneumoniae. In our study a further 33 patients (FEV1% 39.8 (16.3)) were simultaneously sampled using nasopharyngeal aspirates and induced sputum when stable and during 43 COPD exacerbations. We found no C pneumoniae using a nested reverse transcriptase PCR adapted from Cunningham et al4 at stable baseline but nine patients (seven from induced sputum and another two in nasal aspirates) (28%) were positive for C pneumoniae at exacerbation. The presence of C pneumoniae was not associated with smoking history, FEV1%, peak flow change at or peak flow recovery from COPD exacerbation, rate of peak flow recovery, IL-6 (fig 2) or IL-8 levels, or total and differential cell counts in induced sputum. The lack of relationship between C pneumoniae detection and inflammatory markers at exacerbation suggests to us that C pneumoniae exacerbations are no different from exacerbations not associated with C pneumoniae.
We found no relationship between C pneumoniae detection in the airway at exacerbation and exacerbation frequency (p=0.504), but Blasi et al found that C pneumoniae positive patients (in stable COPD) had a greater tendency towards frequent exacerbation. However, the difference in exacerbation frequency between the two groups was small (0.6 exacerbations per year), and the authors need to be cautious about concluding that this difference could affect disease progression.
The main difference between the data of Blasi et al and ours is that in their study 16 of 42 patients (38%) enrolled in study 1 had sputum positive for C pneumoniae by DNA PCR and a similar number (61/141, 43%) in study 2 in PBMCs, both during stable COPD. We sampled only once in stable COPD and found none, despite finding 28% at exacerbation. Blasi and colleagues sampled subjects repeatedly (at least four times), but it is not clear how many times they had to be positive to be defined as “respiratory samples positive for C pneumoniae by DNA PCR”. The 16 positive patients provided 69 sputum samples; were all sputum samples positive on all occasions examined in these patients? Similarly, were all 125 sputum samples from the 26 patients who were C pneumoniae negative always negative? It would be helpful if the authors could give the data on the chronic nature of infection in their sputum samples.

Distribution of serum C pneumoniae microimmunofluorescence (MIF) IgG antibody inverse titres in 110 patients with stable COPD.
{kind=link}
{kind=link}
Induced sputum levels of IL-6 during Chlamydia (+) and non-Chlamydia (–) COPD exacerbations in 33 patients with 43 exacerbations. Outliers are shown; p=0.187 (Mann-Whitney U test).
Authors' reply
We are grateful to Seemungal et al for their comments regarding our recently published paper on Chlamydia pneumoniae and chronic bronchitis.1
Seemungal et al prospectively studied 110 patients with COPD for 1 year, evaluating serum microimmunofluorescence IgG titres, plasma fibrinogen, and IL-6 levels. They found no correlation between high IgG titres and FEV1 % predicted, exacerbation frequency, plasma fibrinogen, and serum IL-6 levels. We also found no correlation between serological results and FEV1 % predicted or exacerbation frequency. In fact, as in previous reports,2 we found a low degree of correlation between C pneumoniae serology and peripheral blood mononuclear cell (PBMC) PCR. A greater degree of correlation was observed when IgG and IgA titres were combined but, unfortunately, no comparison is possible as Seemungal et al only performed IgG titre determinations. In any case, our findings are not truly comparable with those of Seemungal et al as serology is known to be less specific than PCR for the identification of chronic infection with C pneumoniae.3
In the second part of their letter Seemungal et al report the results of an analysis on a further group of 33 patients who were simultaneously sampled for nasal aspirates and induced sputum when stable and during exacerbation. They found no PCR positivity in stable patients, whereas in nine of 43 exacerbations C pneumoniae was detected by PCR in respiratory specimens. The authors infer that DNA positivity in the sputum is a marker of C pneumoniae acute infection; this would mean that around 30% of all acute exacerbations are sustained by C pneumoniae. However, the gold standard for acute infection is still considered serology on paired samples. Applying both PCR and serology on paired serum samples we found an acute infection in two of 34 exacerbations confirming our previous data of an overall incidence of 5–6%.4 Their definition of acute C pneumoniae infection may explain, at least in part, why they could not detect any difference between exacerbations associated or not associated with C pneumoniae in terms of inflammatory response.
The reported discrepancy in PCR positivity on respiratory samples between our study and that of Seemungal et al may be related to different PCR techniques. In fact, we found 16/42 (38%) PCR positive patients with stable COPD, whereas they found 0/33 and 9/33 (28%) in stable COPD and during an exacerbation, respectively. Considering that the rate of positivity in our stable patients is comparable to that of patients with exacerbation in Seemungal’s series, we think that the different PCR results may simply be related to PCR sensitivity, sputum quality/quantity, amount of DNA retrieved from the samples, and number of tested samples.5 Seemungal et al tested a single induced sputum specimen for each stable patient whereas we analysed at least four spontaneous sputum samples for each stable patient. We defined any patient with at least two positive specimens as PCR positive. Sixteen patients were classified as PCR positive on the basis of 43/69 (62%) PCR positive sputum samples. Twenty six patients were considered PCR negative; 24 had repeatedly negative PCR results on all 113 sputum samples and two patients had a single PCR positive sputum specimen (2/12 specimens).
Our results on exacerbation frequency are based on the observation of 141 subjects for 2 years compared with 33 subjects in the study by Seemungal et al. The different number of subjects included in the two studies may explain some discrepancies. We do agree that caution is needed in interpreting the results of our study and stated that “our study indicates the possible role of C pneumoniae chronic infection in disease progression in COPD patients. Further confirmation based on large scale trials is needed”.1 However, even a slight increase in exacerbation frequency may have a role in disease progression.6,7