Article Text

Abstract
Technical developments in spiral CT scanning mean that considerably smaller lung cancers can now be identified than with previous methods of detection. Only time will tell whether this enhanced capability will result in a reduction in the number of deaths from lung cancer. The implications and problems of screening for lung cancer are discussed. Screening implies a careful refinement of a range of clinical activities that must be routinely delivered in a carefully coordinated fashion to allow for the possibility of improved outcome. Critical analyses of the nuances of this process are essential if the field is to move forward.
- lung cancer
- screening
- early diagnosis
- spiral CT scanning
Statistics from Altmetric.com
Introduction
Lung cancer is the most lethal cancer in the world.1 The prospects for changing this reality are clouded by a number of factors including, most notably, the failure of primary prevention significantly to reduce tobacco usage among young people.2,3 In the United States alone for the year 2002 there will be an estimated 169 400 cases of lung cancer and 154 900 deaths.1 The number of deaths from lung cancer deaths exceeds the total number of deaths from breast, colon, prostate, and cervical cancer by over 30 000 cases, yet there are over half a million new cases annually of these four other cancers. Why is lung cancer so much more frequently lethal than these other common cancers? One difference between the management of lung cancer and that of breast, colon, prostate and cervix cancers is that lung cancer is more frequently diagnosed at an advanced metastatic stage. Progress in improving treatment of advanced cancer has been disappointing, so late diagnosis of lung cancer is a fundamental obstacle to progress in lung cancer outcomes.4,5 A summary of the reasons why lung cancer would be an appropriate disease for a population based screening approach is shown in box 1.
Box 1 Why lung cancer screening is attractive
-
Leading cause of cancer death worldwide
-
Leading cause of premature cancer death
-
Symptomatic disease is generally lethal
-
Localised cancer can be managed curatively with today's clinical tools
-
New technology may detect early disease more efficiently
-
Defined high risk cohort based on tobacco consumption
Spiral computed tomographic (CT) scanning potentially provides a robust tool for early detection of lung cancer. Although early stage resectable lung cancer has measurably better survival than advanced stage disease, the current failure to detect early lung cancer routinely is a pivotal feature distinguishing lung cancer management from that of breast, colon, prostate, and cervical cancer. This difference highlights the strategic importance of rapidly evaluating early lung cancer detection systems as a potential vehicle for cancer mortality reduction. Pilot trials of spiral CT based early lung cancer screening in New York and Japan with a frequency of stage I detectable lung cancer in over 80% of newly diagnosed cases are promising.6–10 In many settings in the US these early findings are believed to be sufficiently persuasive to begin promoting spiral CT scanning for early lung cancer detection to individuals at high risk due to a history of tobacco use. A list of reasons why lung cancer screening is not currently endorsed is shown in box 2.
Box 2 Why lung cancer screening is not done
-
No validated screening tool
-
Potential for enormous cost
-
Challenge of developing management strategies to deal with the consequences of imperfect screening tool to minimise adverse outcomes
-
Psychological burden of misclassified screenees
-
Lack of existing screening infrastructure to build upon
WHAT HAS CHANGED?
For many years CT scanning was felt not to be useful in lung cancer because, while highly sensitive, too many suspicious CT findings turned out to be false positives—that is, not to be lung cancer. However, technical innovations leading to the development of very fast CT scans, generally referred to as spiral (or helical) CT, has resulted in renewed interest in CT scanning. Some of this improvement is due to engineering refinements in the movement of the subject through the detector coil so that the images are acquired more quickly. However, much of the enhanced capability is simply related to improved microprocessing power. Better processing power allows not only faster imaging acquisition, but also greater capability in image processing. Detectors for CT can now be arrayed in parallel. Multiple slice scanners increase image acquisition capability as a function of the number of detectors employed. Faster image acquisition means an image can be acquired within seconds so, for most people, a complete study of the thorax can be comfortably obtained during a single breath hold. The motion artifacts formerly introduced by the act of breathing when imaging times were much longer compromised image quality due to the inaccuracy of slice reconstruction. Faster image acquisition time also means that additional image slices through the thorax can be acquired.
The inherent limitations of standard radiographic approaches where three dimensional objects are routinely visualised in two dimensions is being increasingly recognised as unsatisfactory for early diagnosis. The four-detector scanners currently used can easily exceed the old standard of a single slice per centimetre of thorax height and can readily acquire as many as 8–10 images per centimetre. Herein lies the potential to detect very small tumours while avoiding a high rate of interventions for lesions that are not malignancies. Multiple images per centimetre mean that the shape of a small nodule can be established with much greater detail since its volume is reconstructed with information from many more relevant slices. The vastly increased data also enable a more accurate three dimensional reconstruction of tumour or nodule geometry. In general, comparing three dimensional structures from serial scans involves less guesswork about the “registration” (orientation of a structure relative to where the image was acquired) of a lesion than with the standard two dimensional images. This evolution in image processing capability of generating three dimensional renderings of three dimensional lesions is at the core of the enhanced utility of the current generation of high resolution CT scanners. Tremendous progress can be expected as the field becomes more comfortable in working with digital three dimensional datasets and as the capabilities of computer assisted diagnosis continue to evolve and are integrated into routine cancer screening clinical management.
BRINGING THE DIGITAL REVOLUTION TO LUNG CANCER SCREENING
Important validation work is currently ongoing to define precisely the robustness of three dimensional volume rendering. The expected operational capabilities of this new tumour monitoring tool is likely to exceed existing approaches by a wide margin. The pioneering work of the imaging group at Cornell University School of Medicine has suggested an example in this regard. The Cornell investigators have exploited the ability of high resolution CT scanning to do volume comparisons by performing serial scanning over a period of several months. Their proposed criterion for identifying a clinically significant nodule becomes a quantitative assessment of nodule growth instead of a single snap shot of lung anatomy.6,7,11 The rationale for discrimination through volumetric change is that any adult may have a number of old nodules from previous trauma and infections but, at the time of lung cancer screening, most of these old scars would be stable in size. However, for a lung nodule to evolve into a clinically significant cancer, the nodule must be growing. The use of growth rate as a dynamic criterion for further evaluation is based on the observation that malignancies commonly are defined by progressive growth, although in most malignancies the opportunity to observe and measure growth directly is limited by both technology and the need to intervene. With indirect measurements such as prostate specific antigen (PSA), the use of a dynamic evaluation rather than a “one time” evaluation is felt to be a reliable basis for clinical management decisions.12 In the particular case, however, detection of very small nodules offers the advantage of detection very early in the preclinical phase but, likewise, poses the challenge of avoiding excessive diagnostic and therapeutic interventions for misclassified lesions identified on screening studies.
The use of spiral CT scanning for dynamic comparison of three dimensional volumes to determine growth rate will be subjected to ongoing refinement as the number of cases studied with this approach grows. As with all other measures of malignant potential, it probably will not achieve perfect discriminatory performance and thus the technology and near term follow up regimen must be subjected to rigorous clinical evaluation. However, as a cancer screening tool it still represents a major conceptual advance because CT based volumetric images generate an objective quantitative end point derived from a sensitive and robust measurement tool, one that is likely to gain measurement precision over time.
The field of computer assisted diagnosis is evolving rapidly. The first software tools to allow for three dimensional volume comparisons are being finalised by the CT manufacturers. Ongoing efforts in software development should permit fully automated computer assisted diagnosis for the initial evaluation of lung cancer screening studies. If carefully developed and validated, computer assisted diagnosis may be the key to providing reliable screening at an economical cost. From the literature on breast cancer, wide variation in radiological interpretation becomes a progressively greater problem as the evaluation moves to assessment of smaller lesions.13 Subjectivity in evaluating screening scans could limit the potential of this approach. The refinement of computer assisted detection tools, which may improve both sensitivity and specificity, is therefore a critical developmental need for interpretation of screening tests.14
ACHIEVING REDUCTION IN MORTALITY
In discussing precedents for lung cancer screening, it is important to point out that enthusiasm for the technological potential of spiral CT scanning must be tempered with the need to demonstrate efficacy according to conventional criteria for the acceptance of population based screening as outlined by the World Health Organization in 1968.15 The continuing controversial issues with prostate cancer screening are perhaps the most contemporary example of a need to provide a solid base of evidence to demonstrate both efficacy and acceptance, but in fact the development of lung cancer screening faces challenges that are common to any screening test. Although in widespread use, prostate cancer screening is not yet validated as providing a clear benefit in terms of reducing the mortality from prostate cancer. There is a concern that, while the use of a prostate screening test advances the time of diagnosis of prostate cancer in many men, it has not yet been established whether this will result in significantly reduced prostate cancer mortality.
The parallels between prostate and lung cancers are that both generally occur late in life when other non-malignant diseases constitute a significant competing risk for mortality. The clinical care in both situations for potentially curative cancers can be expensive as well as fraught with medical complications, so the consequences of frequent misclassification are very problematic. In light of this, there is a need to define “clinically significant” cancer (a cancer that poses a life shortening risk) compared with a malignancy that does not pose a life shortening risk either because of competing co-morbidity or because the cancer represents overdiagnosis in the strictest sense of the term—that is, it would not progress and become lethal.16 These issues assume significance both for the work up and treatment of cancer cases identified by screening. For patients with lung cancer, in particular, clinical management for diagnostic work up as well as for curative resection will involve a certain fraction of iatrogenic complications including fatalities.
SYSTEM ENGINEERING LUNG CANCER SCREENING
An important and under appreciated criticism of the published lung cancer screening trials is that the downstream work up and care of cancer cases identified by screening was not standardised. This leaves room for variability with the quality of care, and potentially introduces bias into the measure of screening efficacy. While successful randomisation in a screening trial potentially eliminates the chance of unequal distribution of important non-screening prognostic variables, no corresponding handling of the downstream clinical management between study arms has been formally reported. This issue has particular importance for lung cancer screening involving spiral CT scanning. Cancers detected by CT screening, especially in an incidence screening setting, will frequently involve primary lung cancers that are less than 1 cm in volume. The diagnostic work up and optimal care for this type of very small volume disease represents a major new challenge since it is a form of lung cancer that has never before been a focus for clinical management research. Indeed, lesions of less than 1 cm may be highly curable. This is also the situation where the concern about “overdiagnosis”—that is, a cancer that would not cause a shortening of life expectancy—may have some validity.16 Careful study of this issue in order to clearly establish the natural history of these smaller cancers, as well as the best practices for clinical management, is a very high priority at this time.
In developing lung cancer screening systems, a major challenge is actually elucidating all aspects of the work up and intervention of suspected cases to define the safest and most economical management approach. In the past and still today, the orientation of investigations focused on screening was dominated by exposure to screening. Attention to the quality standards in administering the screening test, as well as attention to other aspects of the management of patients with early lung cancer, was not a priority. At both the theoretical and operational level, this is problematic as even a profound benefit of improved cancer detection could be compromised either by suboptimal case work up, suboptimal definitive treatment, or combinations of poor quality diagnostic work up and treatment.
POSSIBILITIES FOR GLOBAL COOPERATION IN SCREENING RESEARCH
A consensus statement from the International Conference on Prevention and Early Diagnosis of Lung Cancer, held in Varese, Italy in December 1998, highlighted the promising results from investigations with spiral CT scanning and other evolving early detection tests, and strongly encouraged “national governments and public health organizations involved in cancer prevention and control to more aggressively address tobacco control and to urgently consider the issues surrounding the early detection of lung cancer”.17
In addition, the consensus statement also indicated that there should be an accelerated research programme to determine the efficacy and effectiveness of these new technologies for early lung cancer detection. Apart from the most salient reason to quickly determine whether lung cancer mortality truly can be reduced by early intervention—that is, the number of deaths from lung cancer that might be avoided—the proliferation of access to testing and promotion of testing to high risk groups in the US may rapidly diminish the potential to conduct a successful randomised trial.
Plans are evolving for a number of different groups in the US and Europe to launch large spiral CT based lung cancer screening trials. At this time, funding for a large randomised controlled trial of lung cancer screening to be conducted in the US is under review. In Europe about a dozen randomised trials are in the planning stages and several pilot programmes are pending. A number of groups have already initiated smaller observational cohort studies. Given the complexity of the lung cancer screening challenge, it is unlikely that a singe trial would answer the fundamental questions to the complete satisfaction of policy makers. Therefore, a US/European collaboration has been underway to harmonise trial designs and protocols to the extent possible so that the fullest range of investigational options are available. This international initiative is important because large trials are expensive, complex, and lengthy, and for these reasons there have been comparatively few of these kinds of studies to evaluate cancer screening tests. Further, the potential for comparative analysis of completed studies has been limited due to lack of coordination in planning and study design. In response to these concerns, an international consortium has been meeting to discuss issues related to the development of validating clinical trials of spiral CT scanning for early lung cancer detection.18 Through the sponsorship of a variety of organisations including the American Cancer Society and the National Cancer Institute in the US and a number of European institutions, a multidisciplinary group of investigators has been meeting. The goals of this collaboration are: (1) scientific exchange; (2) the establishment of common protocols for data elements and measurement, scanning protocols and quality assurance, and pathology and biomarkers; and (3) greater comparability between study end points and, perhaps, ultimately a pooled analysis of data.
This work is attended by a sense of urgency. Many investigators sense that a finite “window of opportunity” exists before broad dissemination of “wild type” screening by individuals at risk for lung cancer and their doctors. There is a significant danger in ad hoc or “rogue” screening as reflected in the editorial written some years ago by Bailar in discussing the challenges in mounting lung cancer screening trials.19 For a screening trial, unless every aspect of the screening process as well as the downstream case management is optimised, the distinct possibility exists that a potential benefit of screening could be lost. The “worst case scenario” is that not only would potential benefit not be realised, but also that trial participants not destined to succumb from lung cancer would incur unnecessary harm as a result of suboptimal clinical management. In one of the most mature screening efforts where the entire management process for breast cancer care was deliberately standardised, a remarkably favourable impact on mortality was reported.20
For lung cancer screening there are a number of important but unresolved clinical management questions on how best to proceed with the screening.
-
What is the appropriate risk stratum to screen, and how will that stratum be defined?
-
What are the criteria for a “positive” scan?
-
What are the imaging parameters to obtain an optimal scan while minimising radiation exposure?
-
What is the safest and most cost effective algorithm to work up suspicious nodules?
-
What is the best procedure to remove a small lung cancer?
-
How often should screened subjects with normal scans be followed with subsequent scans?
-
How do we communicate most effectively the risks and benefits of a screening trial to the participants volunteering for it?
With the anticipated rapid evolution of spiral CT technology as well as image analysis capabilities, the impetus for international collaboration in lung cancer screening is the realisation that, since this complex field is moving so fast, sharing of research information is essential to timely worldwide progress on this public health challenge.
CONTROVERSIES IN CANCER SCREENING
A Cochrane review recently challenged the value of mammography in reducing breast cancer deaths, primarily based on a critique of the seven completed randomised trials.21 Although the criticisms of the underlying methodology were shown to be flawed,22–26 the fact that a screening test that is so well established in terms of practice parameters and public acceptance was subjected to prolonged debate has important implications for the studies that will need to be done to determine the efficacy of lung cancer screening. A central question that emerges is how should we measure screening benefit? For lung cancer screening this basic question poses a unique challenge because there is so little relevant experience.
From a scientific perspective, it is critical to understand the sensitivity of the screening tool with regard to its capability to advance the time of disease detection in a defined population. This earlier awareness of a disease is referred to as “advancing the sojourn time”. For lung cancer, the established measure of sojourn time, or the detectable preclinical phase, landmarks would be the time from the first moment a lesion is detectable by chest radiography to the initial presentation of development of symptomatic disease. From the limited information available in the literature on chest radiographic screening, investigators have speculated that chest radiography advances the diagnosis from clinical detection by the order of 1 year. From all of the negative screening trials based on chest radiography, this short sojourn time is not long enough to allow intervention sufficiently early in the natural history of lung cancer to significantly reduce deaths, since most chest radiographs identify cases of lung cancer which already have at least regionally metastatic disease.
Does spiral CT scanning result in a meaningful increase in sojourn time? In considering this question, a fundamental assumption is that lung cancer evolves over the course of years in a fashion consistent with the progressive theory.27 This theory is consistent with the dominant notion of field carcinogenesis rather then the systemic theory that postulates that cancer begins as a metastatic process.28–30 If cancer is metastatic in origin, then the benefit of improving the sojourn time is moot.
To help illustrate the issue of sojourn time we have constructed a hypothetical baseline screening situation. Figure 1 is a scheme which illustrates the dynamics of this issue. It explores the implications of a more sensitive screening tool which was capable of moving the sojourn time from 1 year to 3 years. The horizontal bars indicate the natural history of hypothetical subjects on a randomised screening trial. In this construct, assume that all true information about the outcomes of the subjects is known. In this setting, the enhanced yield of significant clinical information with the longer sojourn time is evident since more localised cancers would be diagnosed. A longer window for providing “curative” interventions would occur compared with what would happen to the control arm as these subjects would not have been screened. As this field matures, accumulating more information about the actual sojourn time for lung cancer detected by spiral CT scanning will be particularly useful in arriving at a rational determination of screening frequency. In addition, achieving a more precise estimate of the usefulness of the screening tool to advance the sojourn time will reciprocally permit more precise evaluation of the efficiency with downstream clinical management of screen detected cases to realise the potential benefit of improved case detection capabilities.

The importance of sojourn time with success of curative interventions on screen identified cancer cases. This scheme portrays hypothetical “true” clinical outcome with a sample of subjects in a randomised screening trial. Each bar represents a trial participant's course with the indicated progression of disease (see legend). The representation is to show how the sojourn time of 1 year (top arrow) compared with a sojourn time of 3 years (bottom arrow) alters the “window of opportunity” to intervene with the potential for curative intent.
At this time one can only speculate about the potential of spiral CT scanning to advance the diagnosis of lung cancer based on the published pilot lung cancer screening trial data such as that available from the Cornell group. In their two initial reports, the frequency of localised primary lung cancer rose from the 30% frequency seen with some chest radiography screening trials to over 80% stage I lung cancer. Correspondingly, the average size of the detected primary lung cancer lesion also fell from 16 mm in the prevalence study to 8 mm in the incidence study. Based on tumour doubling time relative to lesion size at time of detection, these findings are consistent with a lengthening of the sojourn time as suggested by the breast cancer experience.24 Validation of this potential improvement as it relates to lung cancer mortality needs to be documented.15 From an optimistic perspective, the size of the lesions reported by the Cornell group in their pilot studies is close to the observed experience with typically smaller lesions identified with successful mammographic screening.27,28
The analysis of these issues suggests important implications for the design of screening trials. The concept of sojourn time implies that a successful diagnostic screening tool must detect a cancer case while it is still localised and, hence, curable. The benefit of establishing more precise knowledge about a new screening tool relative to sojourn time would be important for designing the frequency of serial screening for a cohort. From vast clinical experience, cure of lung cancer is only regularly seen in the setting of localised (premetastatic) cancer. A successful screening diagnostic tool must therefore be able to routinely identify localised cancer. Again, from clinical experience, validating the identification of localised cancer can be reliably accomplished only by long term clinical follow up of a cohort to ensure that occult metastatic disease was not present. Determining how frequently a cohort should be screened to establish the natural history of occult metastatic disease is critical. Efforts to accumulate useful information in defining the actual length of sojourn time for lung cancer detected by spiral CT scanning are a high priority of the international collaborators.
Armed with this information, the length of follow up for a cohort could be refined to focus on the relevant period in which the benefit of mortality reduction for lung cancer would be most evident. The Cornell imaging group recently reported an example of this perspective in analysing the benefit of breast cancer screening.24 Their hypothesis was that the sensitivity of the screening tool and the frequency of using that tool in a defined cohort would dictate when one could rationally expect to see a benefit of screening. In looking for mortality benefit, the trial design must incorporate follow up provisions that would determine if a trial was successful by accurately measuring outcomes within that relevant window. The Cornell group proposed that the most informative parameter to monitor to assess the benefit of screening is the case fatality rate of breast cancer.24 While this is an intuitively rational approach, this level of refinement has been frequently overlooked in the design and analysis of screening trials. More thoughtful consideration of these nuances of the design of cancer screening trials may reduce some of the tension in this field and allow for the completion of better designed trials to catalyse the development of best clinical practice in this area.29
WHERE DOES IMAGING SMALLER PRIMARY LUNG CANCERS LEAD?
Another important ramification of the pilot studies at Cornell University arises out of consideration of the average size of the lesions detected in their early screening reports. As previously discussed in the prevalence screen, the average size of a detected lesion was 1.6 cm and the corresponding detected primary size in their follow up incidence screen was 0.7 cm.6,7,11 The frequency of metastatic dissemination with primary lesions of this size is unknown, but there is a reasonable chance that, with these very small volume tumours, there is a lower probability of metastatic dissemination.29 However, if better control of the primary lung cancers is achieved, it is evident from our understanding of field carcinogenesis that the longer an individual survives after a primary resection, the greater is the chance of manifesting a subsequent primary lung cancer.30 This risk for subsequent lung cancer has been estimated to be cumulative and of the order of 1–3% per year.31 With a 10–30% chance of second tumours over a 10 year period of time, the need to preserve pulmonary tissue to permit additional lung cancer resections is essential.
Managing CT detected lung tumours of less than 1 cm is a new clinical situation for which there are no evidence-based recommendations for best clinical practice. In contrast, based on many years of experience, there are some consensus practices for the work up of non-calcified solitary pulmonary nodules when they are over 1 cm in diameter. Since many of the lesions detected by screening will be less than 1 cm, the Cancer Treatment Evaluation Program of the NCI recognised the urgent need to foster adaptive clinical research to define new management approaches to screening small volume cancers. Their response to this challenge was to conduct a “state of the science” meeting to explore new research initiatives for developing effective approaches to manage the types of early cancers revealed by lung cancer screening (the Executive Summary from this meeting is available on the website http://www.webtie.org/sots/Meetings/Lung/June%2019%202001/Default.htm).
For small volume CT detected lung cancers, research options range from less extensive surgical procedures to video assisted thoracoscopy to radiofrequency ablation. Several Japanese groups have explored innovative management options for clinical subsets that they have identified as having a distinctive natural history from their considerable lung cancer screening experience over several decades.8–10,32,33 For example, in managing hilar lung cancers they have reported several bronchoscopically administered ablation techniques that have achieved satisfactory local control of the small primaries with excellent long term survival.
In the US the first surgical question in managing small volume lung cancer identified by screening is the appropriateness of lobectomy and mediastinal dissection compared with less invasive approaches. Before the introduction of spiral CT scanning the Lung Cancer Study Group (LCSG) had shown that lobectomy was superior to less than complete anatomical resection, but this was with larger (generally radiologically detected) primary lung cancers.34 There is an emerging sense that the types of lung cancer cases identified by screening are clinically different from the routinely diagnosed cases evaluated in the previous LCSG study. As a result, there is a need to determine the frequency of nodal and distant metastatic disease with lung cancers of <1 cm. This information would be most useful in the subsequent design of new management approaches in this situation.
Dutch workers have also reported considerable efforts to refine the management of early lung cancer confined to the airways.35,36 A key observation from this experience was that local recurrences could be successfully retreated with surgical salvage if the lesions were discovered early. In this pilot study with mean long term follow up of about 5 years, the cure rate for medically inoperative patients managed with local modalities was more than 75%. This experience is consistent with the Japanese results and both of these pioneering efforts suggest that research efforts in highly selected patients to develop less morbid approaches to primary lung cancer control are responsible in a thoracic cancer research setting where close follow up measures can be ensured.
Spiral CT scanning excels in the detection of small peripheral cancers. The research options for lung cancer resection that have been proposed for peripheral lung primaries include segmentectomies, wedge resections, and video assisted thoracoscopic surgery. The evolution of CT technology from a single detector to increasing numbers of detectors is going to result in progressively more sensitive detection of small nodules. As we develop the tools to map these ever smaller lesions routinely, it will become more difficult to establish with certainty that these tiny nodules will be life threatening. Should clinicians fully resect these lesions and exhaustively study them with the latest molecular diagnostic tools? Will spiral CT scanning ever achieve a sensitivity sufficient to detect routinely growing lesions before metastatic involvement is likely so that clinicians could move to a non-invasive tissue ablative technique such as conformal radiotherapy or radiofrequency ablation without a diagnosis? Will aerosolised delivery of high local/regional doses of anticancer drugs allow for effective control of small volume nodal involvement? Will patients treated with these less intrusive experimental approaches to primary lung cancer control comply with ongoing spiral CT monitoring such that the potential for surgical salvage of local recurrences with curative potential is not lost? The implication of tobacco induced field cancer raises additional issues since—after initial successful management of a primary lung cancer and if the person lives long enough—there is a high likelihood of finding subsequent primary lung cancers.
In cases of lung cancer detected by screening, management of the initial lung cancer must incur minimal trauma or side effects so that the individual maintains sufficient pulmonary reserve to allow successful control of subsequent new primary lung cancers. Yet there is a question on how to conduct responsible research on safe and less morbid ways to control screening detected lung cancers without compromising an individual's most established chance of a cure.
In the current situation, patients with non-operable cancer present the most direct opportunity to investigate the benefits of research options for innovative new approaches to the primary control of small volume lung cancer. There exists a small but real number of newly diagnosed patients with lung cancer who either have medical contraindications for lung resection or are disinclined to undergo a surgical procedure. In the NCI “state of the science” meeting ranges of proposed options were suggested including radiotherapy based options (such as brachytherapy and conformal or stereotactic radiotherapy techniques). Since non-operative early stage lung cancers are not numerous, there is a significant need to cooperate across broad groups of clinical trial structures to ensure that the new options for managing small primary lung cancers are rapidly evaluated.
MOVING TO MOLECULAR ONCOLOGY
The field of cardiology has witnessed a remarkable shift from surgical intervention to medical intervention with a corresponding improvement in outcomes. Is this a model for lung cancer management? As the size of lung primary cancers detected by routine screening continues to shrink, research modalities emerge that are progressively less invasive—from photodynamic laser therapy to radiofrequency ablation to the use of aerosolised drugs. If these approaches are found to be useful in controlling either very small lung cancers or even preinvasive lung cancers and their administration turns out to be safe and economical, then a simpler management of early lung cancer may evolve. Correspondingly, with such improvements in management options, the spectre of overdiagnosis diminishes.
Rigorously designed and implemented clinical trials would be necessary to establish if new tools are effective in early and only “suspicious” lesions. This type of research may entail “watch and wait” provisions in which further standard interventions are used only if the suspected primary is not successfully controlled by the research intervention already piloted by Japanese and Dutch workers.32,33,35,36 An area where this type of research approach may be appropriate would be in the management of patients with “ground glass opacities”.37 New research is suggesting that these CT detected interstitial changes may in fact be a preinvasive precursor of adenocarcinoma of the lung and therefore a favourable clinical entity for translational research.
The purpose of proposing this type of innovative research is to address the concern about dealing with the concept of “overdiagnosis” with lung cancer screening. With safe interventions, accepting a level of “overdiagnosis” would even become desirable to ensure sensitivity in finding all potentially lethal lung cancers. Spiral CT technology is and will continue to evolve rapidly in its imaging sensitivity. Even with the newest generation spiral CT scanners with eight detector heads, the routine detection of growing lesions of 3–4 mm will be possible and the problem of how to manage these small lesions will assume growing importance. Concerns about “overdiagnosis” must be balanced by the reality of the modest utility of current lung cancer detection and treatment approaches. Solving the integrated problem of, not only finding early localised cancer, but also validating a safe and effective modality to eradicate such localised lesions is at the core of developing successful screening for lung cancer.
In patients with primary cancer or preinvasive disease of minimal size that could be detected by CT based lung cancer screening, the extent of disease is confined to the respiratory epithelium. This location and size represents a potentially favourable situation for innovative drug delivery strategies. Current clinical management tools have not been optimised to manage this localised phase of early lung cancer. As a research direction, we propose that arresting the progression of clonal lung cancer growing in the bronchial epithelium may be facilitated by using direct delivery of chemopreventive drugs.29 The target of this drug delivery strategy would be the “field” of cancer injury, which includes the extent of the airway tissue in the direct path of the tobacco combustion products chronically deposited on the respiratory epithelium.38 A goal of chemoprevention is to identify mechanistically directed agents which arrest the clonal progression of cancer and avoid the clonal progression to the final lethal phase of aerodigestive cancers.39
The most attractive candidate molecules with which to begin this evaluation are the retinoids. Based on seminal work conducted at M D Anderson over the last decade,40–42 administration of chronic retinoids results in the suppression of new upper aerodigestive cancers. Through the translational efforts with vitamin A analogues, it is not clear that this strategy can be implemented without undue clinical toxicity when the chemopreventive is given orally. The frequent occurrence of such side effects is a particular problem for chemoprevention agents as the average patient suitable for this treatment has no clinical symptoms and is not likely to be willing to tolerate noxious drug related complications. In the first report of a positive chemoprotective effect with 13-cis-retinoic acid, the dose of retinoid was originally 100 mg/M2 but this was reduced to 50 mg/M2 because of toxicity.40 For the follow up trial, which was not successful, the dose of 13-cis-retinoic acid was further reduced to a total daily dose of 30 mg in an effort to identify an effective chemopreventive approach with a more acceptable side effect profile.42 Was the unintended consequence of the major retinoid dose reduction to ameliorate side effects an associated failure to achieve a critical retinoid dose in the bronchial epithelium?
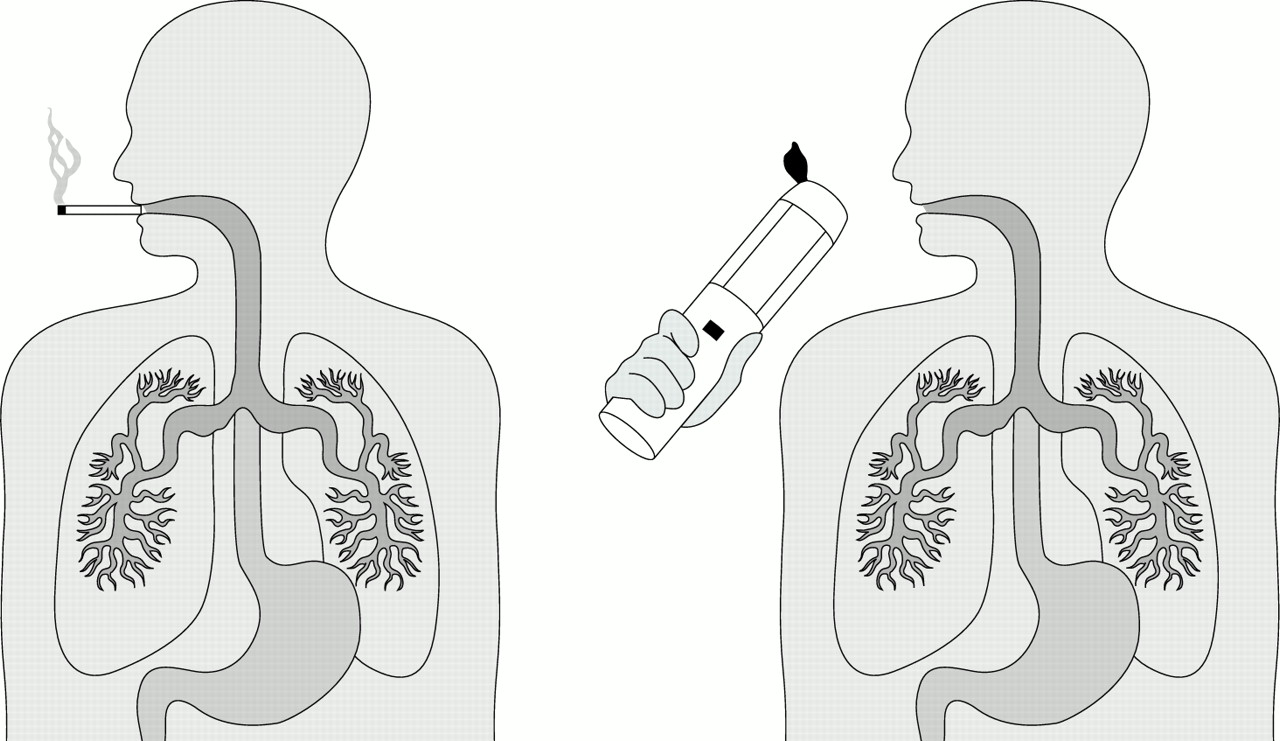
Through the use of aerosolised delivery technologies and other local delivery approaches, higher drug levels can be administered with minimal systemic toxicity by preferentially targeting the cancer field.38 The logic of aerosol drug delivery is evident as deposition of the carcinogen is also accomplished via aerosol delivery (fig 2). The volume of the primary target area is vastly smaller with aerosol delivery than with an orally administered drug for respiratory epithelial chemoprevention. The relevant compartments for saturation with oral drug delivery, depending on the chemistry of the agent, are either the intravascular compartment or the total body compartment. These compartments vastly exceed the volume of the interstitial fluid of the respiratory epithelium (about 15 ml), and this fluid bathes all the cells at risk of emerging as a lung cancer for the first decade or more of the natural history of lung carcinogenesis. Aerosolised antibiotic delivery has been used with great success in the management of pulmonary infections in cystic fibrosis where the chronic parenteral administration of antibiotics led to severe side effects. Preliminary experiments in an animal model of tobacco associated carcinogen induced lung adenomas treated with aerosolised retinoids suggest the feasibility of this approach.43,44 Direct delivery of pulmonary drugs, if validated in human trials, may enable an integrated prevention orientated management strategy that may ultimately contribute to a substantive reduction in mortality. A range of other critical research tools may also contribute to the successful management of very early stages of cancer.45
{kind=link}
{kind=link}
Rationale for pulmonary delivery to manage the premetastatic phase of a cancer that is generally caused by the aerosolised delivery of carcinogens. Pulmonary delivery can saturate cellular targets on the respiratory epithelium at an extraordinary dose and routinely result in systemic doses that would be non-clinically significant. This is a logical but essentially untested approach to improving the therapeutic index with lung cancer chemoprevention.
OTHER ISSUES WITH LUNG CANCER SCREENING
Bailar's description of lung cancer screening as a chain is still relevant.19 The integrity of a chain is defined by the weakest link. In screening, whichever aspect is not optimised is likely to undermine the success of all the other defined steps. In this review we have discussed how best to manage an individual with a treated small volume primary cancer. However, even if we resolve that, other problems could emerge. How often should the patient be monitored with a spiral CT scan to intercept the development of a metachronous primary lung cancer? What are the roles of adjunctive diagnostic methods such as bronchoscopy or needle aspirations in assisting the diagnostic work up? What is the algorithm with the most efficient diagnostic work up and the lowest cost and morbidity? These and many other related questions could benefit from additional objective information.
Establishing a rational basis for the ongoing management of subjects with a variable risk of lung cancer will be essential to determine the cost of this new type of clinical management. Cost will be a crucial consideration in terms of the broad dissemination of these new approaches, and incorporating the evaluation of this and other important outcome measures such as quality of life into the early stages of this cancer clinical management research is essential.46,47 To accomplish this it will be necessary to foster broad collaboration between interested research groups. For instance, for very small CT detected lesions of uncertain natural history, rigorous research is required to define the safest, least expensive, and least intrusive intervention to control these early lesions. In addition, since these cases will only be routinely found by screening, even with high risk populations only a few cases per cohort would be expected. In the face of the global tobacco epidemic, there is an unprecedented need for collaborative interactions between screening institutions to address research questions about downstream clinical management issues in a timely fashion.48 It is unlikely that a single large centre working alone could successfully address even one of these new management research issues by itself.
CLOSING THOUGHTS
In parallel with the multidisciplinary effort to refine the process of conducting and validating a clinical trial, a number of entrepreneurs are offering spiral CT scanning as a routine clinical service. How are the entrepreneurs going to handle the issues outlined above? For the next decade, as we await a definitive trial of spiral CT screening, what do the clinicians tell the many patients who will die of lung cancer? While many investigators are optimistic about spiral CT scanning as a tool for early detection of lung cancer, the clinical management of the small lung lesions detected by spiral CT scanning is a new and uncharted clinical challenge. These are critical questions for which there exists no clear consensus as to the best way forward.
In the absence of data to support screening but with increasing availability and promotion of such technology, an individual with a high risk of lung cancer who is informed of the imprecise state of our knowledge about spiral CT based detection of early lung cancer may still want to have a lung cancer test.49 In that circumstance, ideally in consultation with their physician, the individual should find an imaging centre with a commitment to the integrated management of lung cancer detection. Such a centre should have stable relationships with an array of other lung cancer specialists who know and understand the challenges of lung cancer screening, including radiologists, pulmonologists, and surgeons. Additional expertise from radiation therapists, medical oncologists, and surgical oncologists may be required to deliver appropriate therapeutic interventions. As most lung cancer risk factors are life long, a continuing relationship at the screening site is prudent to permit ongoing monitoring at some interval. Research groups are discussing the implementation of certification procedures to ensure that only institutions with an appropriate commitment to the rigour of this early lung cancer screening process are licensed to provide such a service. As yet, no standards exist for this designation so due diligence on the part of the public is critical.
It is clear that spiral CT scanning in the hands of skilled professionals can find considerably smaller cancers more frequently than with previous lung cancer detection tools. Only time will tell whether this enhanced capability will result in reducing the mortality of lung cancer. Over the next decade people at risk of lung cancer should discuss these issues with their physicians and make their own decisions in this promising but uncharted area. Ongoing considerations of these difficult issues by relevant parties are essential.
REFERENCES
Footnotes
-
The National Cancer Institute's randomised detection trial of 50 000 person spiral CT scans versus chest radiographs has just opened for accrual. Information about the recently started National Lung Screening Trial can be obtained at the site http://newscenter.cancer.gov/BenchMarks/archives/2002_09/index.html or http://cancer.gov/NLST.