Article Text

Abstract
Background: A study was undertaken to determine the oropharyngeal carrier state of potentially pathogenic microorganisms (PPM) and the magnitude of colonisation and infection rates of the lower airways with these PPM in children requiring long term ventilation first transtracheally and afterwards via a tracheotomy.
Methods: A 5 year, prospective, observational cohort study was undertaken in 45 children (33 boys) of median age 6.4 months (range 0–180) over a 5 year period at the Royal Liverpool Children's NHS Trust of Alder Hey, a university affiliated tertiary referral centre. The children were first admitted to the 20-bed paediatric intensive care unit (PICU) and, following placement of a tracheotomy, they were transferred to a four bedded respiratory ward. The two main indications were neurological disorders and airway obstruction. All children were ventilated transtracheally for a median period of 12 days (range 0–103) and, after placement of the tracheotomy, for a similar period of 12 days (range 1–281). Surveillance cultures of the oropharynx were taken on admission to the PICU and on the day of placement of the tracheotomy. Throat swabs were taken twice weekly during ventilation, both transtracheal and via the tracheotomy. Tracheal aspirates were taken once weekly and when clinically indicated (in cases where the lower airway secretions were turbid).
Results: Twenty five patients (55%) had abnormal flora, mainly aerobic Gram negative bacilli (AGNB), particularly Pseudomonas aeruginosa, while the community PPM Staphylococcus aureus was present in the oropharynx of 37% (17/45) of the study population. The lower airways were sterile in six children; the other 39 patients (87%) had a total of 82 episodes of colonisation. “Community” PPM significantly increased once the patients received a tracheotomy, independent of the number of patients enrolled, episodes of colonisation/infection, and the number of colonised/infected patients. “Hospital” PPM significantly decreased after tracheotomy only when episodes were compared.
Conclusions: While P aeruginosa present in the admission flora caused primary endogenous colonisation/infection during mechanical ventilation on the PICU, S aureus not carried in the throat was responsible for the exogenous colonisation/infection once the patients had a tracheotomy. This is in sharp contrast to adult studies where exogenous infections are invariably caused by AGNB. This discrepancy may be explained by chronic underlying conditions such as diabetes, alcoholism, and chronic obstructive pulmonary disease which promote AGNB, whereas the children were recovering following tracheotomy.
- children
- colonisation
- infection
- tracheotomy
Statistics from Altmetric.com
A MEDLINE search using the MESH words “flora”, “tracheotomy”, and “paediatric” revealed only one paper published 20 years ago1 which evaluated the flora of lower airways in 27 children who received a tracheotomy.
A prospective study was undertaken of the microbiology of 45 tracheotomised children over a period of 5 years. Serial samples from both the oropharyngeal cavity and lower airways were obtained in children who required ventilation initially transtracheally on the paediatric intensive care unit (PICU), and subsequently via a tracheotomy on a specialised respiratory ward. The two main end points of this observational cohort study were:
the microbiological end point of oropharyngeal carriage of potentially pathogenic microorganisms (PPM);
the clinical end point of colonisation/infection of the lower airways in children requiring chronic ventilatory support.
METHODS
Patient population
The investigation was a prospective observational 5 year cohort study in children admitted to the Royal Liverpool Children's NHS Trust of Alder Hey, a university affiliated centre of 320 beds. They were admitted first to the 20 bed PICU and, following placement of a tracheotomy, were transferred to the four bedded respiratory ward for children requiring chronic ventilatory support.
Between September 1993 and August 1998 a total of 45 children were consecutively enrolled in the trial. All patients admitted to the PICU and ventilated transtracheally for a minimum of 4 days were enrolled and the study was then continued on children who required a tracheostomy.
Study protocol
Surveillance samples
Surveillance samples from the oropharynx were obtained immediately on admission to the PICU and on the day of placement of the tracheotomy. Afterwards, throat swabs were taken twice weekly during ventilation, both transtracheally and via the tracheotomy. The samples were used to determine the microbiological end point of the carrier state of PPM.2
Diagnostic samples
Tracheal aspirates were taken from the lower airways once weekly and when clinically indicated—that is, when the lower airway secretions were turbid. Colonisation was distinguished from infection using thresholds for both potential pathogens and leucocytes (see definitions).3
Placement of tracheotomy
In all patients the placement of a tracheotomy was performed electively and never as an emergency. The placement of a tracheotomy was considered under the following circumstances4:
when there was airway obstruction which was unlikely to resolve in the short term;
when a patient had been on a ventilator for a prolonged period and there was a high risk of acquiring subglottic stenosis from endotracheal tube trauma;
when the patient was unsuccessful in being weaned from the ventilator because of lower airway or neuromechanical disease.
Two weeks of transtracheal mechanical ventilation was considered to be safe, in line with the experience of others.5
Antibiotic policy
Systemic antibiotics were given only in case of infection. Infection was diagnosed from clinical signs including fever of 38.5°C, leucocytosis >12 000 × 109/l, raised C reactive protein (CRP) >15 μg/ml combined with purulent tracheal aspirates yielding ≥106 colony forming units (CFU)/ml. All five requirements had to be fulfilled for the diagnosis of infection. Tracheobronchitis was distinguished from pneumonia by the absence of chest radiographic changes. Infection due to Gram positive bacteria was, in general, treated with a first generation cephalosporin, while a third generation cephalosporin was given to children who developed a lower airway infection caused by aerobic Gram negative bacilli (AGNB). Infection in general was treated with a 5 day course of antibiotics, followed by clinical re-evaluation of the patient.
Microbiological processing
Surveillance samples of the oropharynx
Throat swabs were processed qualitatively and semi-quantitatively to detect the level of carriage. Three solid media—chocolate (Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis), staphylococcal (Staphylococcus aureus, both sensitive and resistant to methicillin) and MacConkey (Escherichia coli and AGNB) agar—were inoculated using the four quadrant method combined with an enrichment (brain-heart infusion) broth.6 Each swab was streaked onto the three solid media, then the tip was broken off into 5 ml of broth. All cultures were incubated at 37°C under aerobic and CO2 enriched atmosphere. The MacConkey agar plate was examined after one night and the plates for S pneumoniae, H influenzae, M catarrhalis and staphylococci after two nights. In addition, if the enrichment broth was turbid after one night of incubation, it was then inoculated onto the three media. A semi-quantitative estimation was made by grading growth density on a scale of 1+ to 5+ as follows: 1+ = growth in broth only (approximately 10 microorganisms/ml), 2+ = growth in the first quadrant of the solid plate (≥103 PPM/ml), 3+ = growth in the second quadrant (≥105 bacteria/ml), 4+ = growth in the third quadrant (≥107 microbes/ml), 5+ = growth on the whole plate (≥109 microbes/ml). Macroscopically distinct colonies were isolated in pure culture.
Diagnostic samples of the lower airways
Endotracheal aspirates were mechanically homogenised using glass beads and were vortexed for 1 minute. The samples were then inoculated using the four quadrant method (without enrichment broth) onto Columbia blood agar in addition to the three above described plates. All plates were incubated at 37°C under aerobic and CO2 enrichment atmosphere. Cultures were read for growth density using the semi-quantitative estimation of low, moderate, high, and very high growth density after 24 and 48 hours.7
Identification
Streptococcus pneumoniae
Streptococcus pneumoniae isolates were identified by their α-haemolytic colony morphology and susceptibility to an optochin disc.
Haemophilus influenzae
Tiny colonies appearing like “dew” drops with a distinctive “sweet” smell were considered probable Haemophilus influenzae isolates and they were further analysed for their X (hemin) and V (NAD) factor requirements.
Moraxella catarrhalis
Moraxella catarrhalis isolates were identified by their dull yellow colony morphology, the “sliding” test over the chocolate plate, and the positive oxidase test. Gram negative diplococci in the Gram stain that were methylum belliferyl butyrate positive were identified as M catarrhalis.
Staphylococcus aureus
Staphylococcal isolates were identified by their smooth, slightly domed colony morphology with entire edge 1–2 mm diameter. Staphylococcal colonies with a golden, yellow or creamy pigmentation were considered to be S aureus, while non-pigmented colonies were assumed to be non-aureus staphylococci. S aureus was identified by its power to form potent coagulating substances, coagulases. To differentiate coagulase positive staphylococci (S aureus) from coagulase negative staphylococci (CNS) the production of DNase by a DNA agar plate method and a slide agglutination test (Staphaurex, Wellcome Diagnostics) to detect clumping factor and protein A were used. If both tests were positive, the staphylococcal isolate was identified as S aureus. If both were inconclusive, a tube coagulase test with strain NCTC 6571 as a positive control was performed and read at 4 and 24 hours. CNS were identified by a negative tube coagulase test.
S aureus isolates that grew in the 8 mg/l oxacillin well were presumptively identified as MRSA. A subsequent positive E-test with an MIC of ≥64 mg/l oxacillin confirmed the MRSA identification.8
Aerobic Gram negative bacilli (AGNB)
Aerobic Gram negative bacilli were identified by the ATB system.9
Relatedness of potential pathogens
Relatedness of microorganisms was determined by antibiotyping using extended sensitivity patterns for the enterobacteria, phage typing for S aureus, and pyocin typing for Pseudomonas aeruginosa.10
Definitions
Flora
Microorganisms were classified into potentially pathogenic microorganisms (PPM) and low level pathogens for the lower airways using the virulence or intrinsic pathogenicity of the microorganisms.11 The intrinsic pathogenicity or virulence index of a microorganism was defined as the ratio between the number of patients infected by a particular microorganism and the number of patients carrying that microorganism in the oropharynx. Indigenous flora, including anaerobes and viridans streptococci, rarely cause lower airway infections despite being carried in high concentrations with an index of 0.01–0.03. Enterococci, yeasts, and coagulase negative staphylococci are also carried in the oropharynx in high concentrations by a substantial percentage of patients in intensive care units, but are unable to cause lower airway infections. These are low level pathogens, while high level pathogens such as Salmonella species have an index approaching 1 for the gut.
There are about 14 potentially pathogenic microorganisms with indices between 0.1 and 0.3. These include the five “community” microorganisms—S pneumoniae, H influenzae, M catarrhalis, E coli, and S aureus—present in previously healthy individuals, and the nine “hospital” bacteria carried by patients with an underlying condition both chronic and acute (Klebsiella, Proteus, Morganella, Enterobacter, Hafnia, Serratia, Pseudomonas, Acinetobacter spp and methicillin-resistant S aureus (MRSA)).
Carriage or carrier state
When the same strain of a potential pathogen was isolated from at least two consecutive surveillance samples in any concentrations over a period of at least 1 week, the patient was considered to be in a carrier state. Samples for the detection of the microbial end point of oropharyngeal carriage included throat swabs. If one swab was positive for a potential pathogen that differed from previous isolates, the patient was considered to have acquired a potential pathogen. Oropharyngeal carriage therefore refers to the persistent presence of a PPM in the oropharynx. An acquired opportunistic potential pathogen—that is, the eight abnormal AGNB and MRSA—are thought to be present only transiently in an otherwise healthy host. Acquisition may lead to the abnormal carrier state in the diseased individual.
Normal flora
Individuals who enjoy reasonably good health only carry low level pathogens including the indigenous anaerobes, viridans streptococci, enterococci, coagulase negative staphylococci, yeasts, and the five “community” bacteria. Oropharyngeal carriage of the “opportunistic” AGNB and MRSA is uncommon in healthy people.12
Abnormal flora
Patients with an underlying condition, both acute and chronic, may carry abnormal flora including the opportunistic AGNB and MRSA in the oropharynx. While the indigenous E coli is normal in the gut, oropharyngeal carriage of E coli in high concentrations of ≥3+ or ≥105 microbes/ml saliva (overgrowth) was considered to be an abnormal carrier state. Underlying disease is thought to be the most important single factor associated with increased availability of AGNB receptor sites on the digestive tract mucosa.13–15
Colonisation
Colonisation was defined as the presence of a potential pathogen in an internal organ that is normally sterile. Diagnostic samples from the lower airways yielded <3+ or <105 colony forming units (CFU) of potential pathogens per ml of lower airway secretions. In general, only a few + leucocytes were present in colonised lower airways, on a semi-quantitative scale of + = few, ++ = moderate, and +++ = many leucocytes.
Infection
Infection was defined in this study as a microbiologically proven clinical diagnosis of inflammation, local and/or generalised. This includes not only clinical signs but also the presence of a minimum of moderate ++ leucocytes, and of >3+ or >105 microbes/ml in the diagnostic samples obtained from the lower airways.
Tracheobronchitis
Tracheobronchitis was clinically suspected if the child had a fever of ≥38.5°C, leucocytosis of ≥12 000 × 106/l, or leucopenia of ≤4000 × 106/l, a raised CRP of ≥15 μg/ml, and purulent tracheobronchial secretions yielding ≥3+ or ≥105 CFU in the presence of ++ leucocytes. Changes on the chest radiograph were not required.
Bronchopneumonia
Bronchopneumonia was suspected in the presence of new or progressive pulmonary infiltrates on the chest radiograph in addition to the five clinical and laboratory criteria described above.
Primary endogenous lower airway colonisation/infection
Primary endogenous lower airway colonisation/infection was defined as colonisation or infection of the lower airways caused by a PPM isolated from the lower airway secretions and carried by the patient in the oropharynx at the time of admission to the PICU and/or of placement of the tracheotomy.
Secondary endogenous colonisation/infection
Secondary endogenous colonisation/infection was defined as colonisation/infection of the lower airways caused by a PPM isolated from the tracheal aspirate and not carried in the throat at the time of admission to the PICU and/or tracheotomy, but appearing later.
Exogenous colonisation/infection
Exogenous colonisation/infection was defined as colonisation or infection of the lower airways caused by a PPM isolated from the tracheal aspirate that was not previously carried by the child in the throat at any time.
Statistical analysis
Standard error of differences using a two tailed exact method of proportions analysis with 95% confidence intervals was used for statistical analysis of the data. The null hypothesis was that the prevalence rate is the same when comparing any two populations. Populations were the same for comparison of types of colonisation/infection (primary endogenous, secondary endogenous, exogenous) during the stay in the PICU and respiratory ward. Populations were different when those colonised/infected with community and hospital microorganisms were compared during the two periods in the PICU and respiratory ward.16
RESULTS
Clinical data
A total of 45 children (33 boys and 12 girls) of median age 6.4 months (range 0–180) were enrolled in the study. The two main indications were neurological disorders and airway obstruction. All children were ventilated transtracheally for a median period of 12 days (range 0–103) and after placement of a tracheotomy for a similar period of 12 days (range 1–281).
PPM carried by the children on admission to the PICU were responsible for significantly more episodes of primary endogenous colonisation/infection than bacteria present in the throat flora at the placement of the tracheotomy (76% v 55%, p=0.03). Conversely, PPM associated with the respiratory ward and causing secondary endogenous and exogenous episodes of colonisation/infection were significantly more common during ventilation via tracheotomy than PICU related PPM causing colonisation/infection during transtracheal ventilation (24% v 46%, p=0.02)
Microbiological data
Carriage
Of the 45 children, 25 (55%) were abnormal oropharyngeal carriers of a total of 30 AGNB. Eleven carried P aeruginosa, four had Klebsiella in the oropharynx, while Enterobacter spp, Acinetobacter spp, and E coli were present in the throat of three children each. Seventeen children carried the abnormal flora on admission to the PICU at enrolment in the trial. Eight children developed secondary carriage during the study: one child developed supercarriage with P aeruginosa while on the PICU, the other seven during their stay on the respiratory unit. The bacteria involved were E coli in one child, Enterobacter spp, Acinetobacter spp and P aeruginosa in two children each.
Oropharyngeal carriage of S aureus was 37% (17/45). Thirteen children imported S aureus on admission to the PICU and four patients became S aureus carriers during their stay on the PICU (one patient) or the respiratory ward (three patients). Carriage of “community” bacteria was low: four different children (9%) carried S pneumoniae and M catarrhalis, and H influenzae was carried by five children (11%).
Colonisation of the lower airways
Twenty four children (53%) had 26 episodes of lower airway colonisation while on transtracheal ventilation on the PICU. Following placement of the tracheotomy, 15 more children (total 39 (86%)) developed 56 colonisation events. There was a total of 82 events of colonisation of the lower airways throughout the study. S aureus and P aeruginosa were the predominant PPM during both modes of ventilation. The lower airways were sterile in only six children whether they were ventilated transtracheally or via a tracheotomy tube. They were nearly all normal carriers, with only one child being a carrier of S aureus.
Nineteen colonisation events were primary endogenous—that is, caused by PPM that the child imported on admission to the PICU. There were four secondary endogenous and three exogenous colonisation events resulting from breaches of hygiene during the stay on the PICU while on transtracheal ventilation. A total of 33 PPM were involved in the 26 colonisation episodes in the 24 patients who were mechanically ventilated on the PICU.
Following tracheotomy a total of 56 colonisation events occurred, 31 primary endogenous, 10 secondary endogenous, and 15 of exogenous pathogenesis. A total of 63 PPM caused the 56 colonisation events in 39 patients.
Infection of the lower airways
During transtracheal intubation 13 patients developed 15 infections while on the PICU. Twelve were primary endogenous and they were caused by P aeruginosa (n=6), S aureus (n=4), H influenzae (n=1), and S maltophilia (n=1). P aeruginosa caused one secondary endogenous infection and the two exogenous infections were due to Acinetobacter and S maltophilia.
Seven of the 45 children developed 10 lower airway infections once they were tracheotomised. There were five primary endogenous infections (H influenzae; H influenzae/M catarrhalis; S aureus; S aureus and P aeruginosa), three secondary endogenous (S aureus, Acinetobacter, P aeruginosa), and two exogenous (both S aureus) lower airways infections.
Of the 25 infection episodes, 15 (nine pre-tracheotomy, six post-tracheotomy) were diagnosed as pneumonia and 10 (six pre-tracheotomy, four post-tracheotomy) as tracheobronchitis.
PPM involved in carriage, colonisation, infection
Carriers
During the stay in the PICU 21 “community” PPM were carried by the 45 patients which increased to 29 (p=0.04) when the patients were on the respiratory ward (fig 1). There was no difference in the carrier state of “hospital” PPM in the PICU and on the respiratory ward (21 v 23, p=0.3).

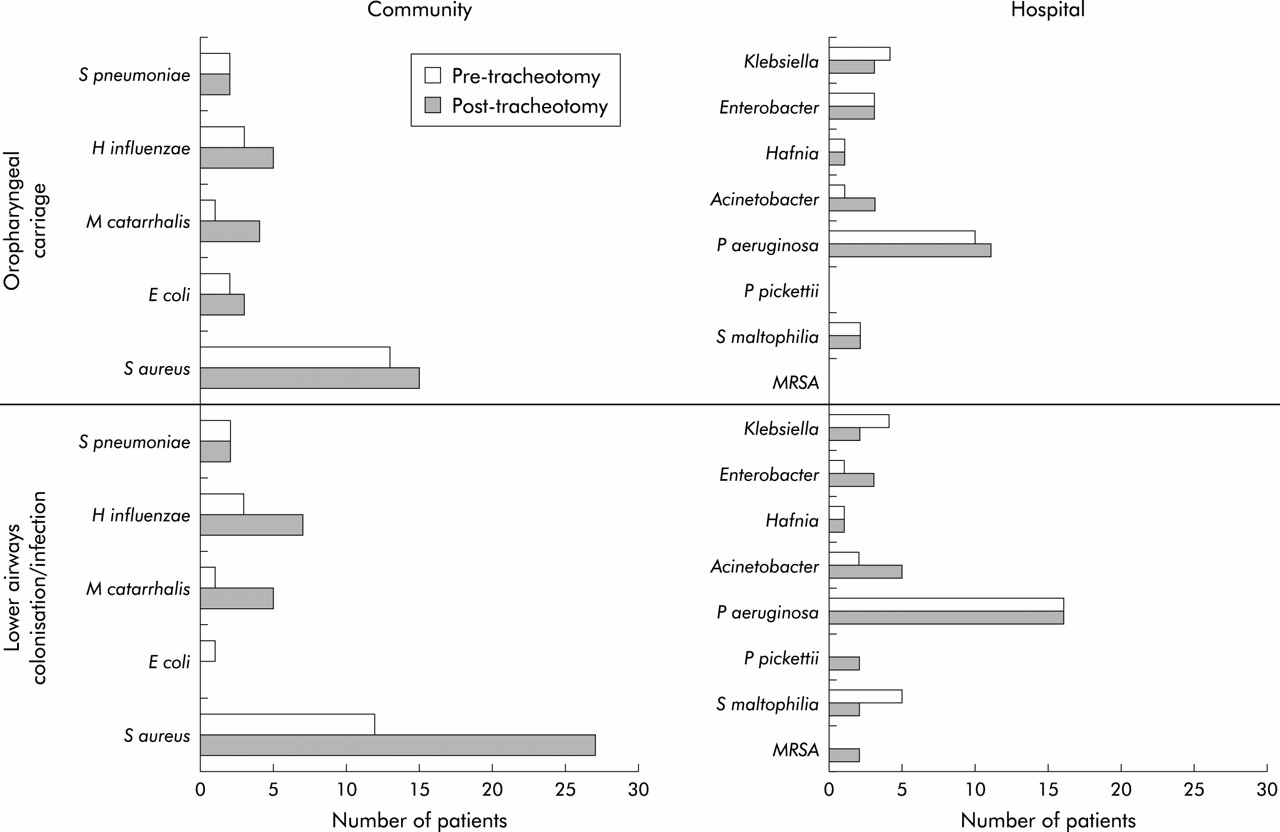{kind=link}
Oropharyngeal carriage profiles for “community” and “hospital” bacteria and colonisation/infection patterns of the lower airways in children requiring long term ventilatory support, first transtracheal followed by tracheotomy (pre-tracheotomy; post-tracheotomy). Staphylococcus aureus caused exogenous colonisation/infection of the lower airways (without previous throat carriage) in children with a tracheotomy.
Colonisation/infection episodes
During their stay in the PICU 24 patients developed 41 colonisation/infection episodes with 48 PPM, while on the respiratory ward 39 patients developed 66 colonisation/infection episodes with 75 PPM. Pre-tracheotomy, of the 48 PPM 19 were “community” bacteria (19/41) while post-tracheotomy, of the 75 PPM isolated from the 39 patients, 42 were “community” microorganisms (42/66, fig 1). The difference was significant (p=0.05), indicating that “community” PPM were more prevalent in the lower airways of the tracheotomised children. During transtracheal ventilation on the PICU significantly more “hospital” bacteria were isolated from the lower airways than following placement of a tracheotomy (29/41 v 33/66, p=0.02).
Nineteen “community” PPM were isolated from the lower airways of 24 patients during the PICU stay compared with 42 from 39 patients on the respiratory ward. The increase in “community” PPM post-tracheotomy was statistically significant (p<0.0001). There was no difference between the ratios of “hospital” PPM per colonised/infected patient during the two modes of ventilation (29/24 vs 33/39, p=0.2).
“Community” PPM therefore increased significantly once the patients received a tracheotomy, independent of the denominator study population, episodes of colonisation/infection, and number of colonised/infected patients. “Hospital” PPM decreased significantly after tracheotomy only when episodes were compared.
DISCUSSION
The two main findings to emerge from this microbiological study were that (1) while there was no change in the number of opportunistic AGNB, community bacteria—particularly S aureus—increased following tracheostomy, and (2) P aeruginosa present in the flora on admission caused primary endogenous colonisation/infection during mechanical ventilation on the PICU while S aureus not carried in the throat was responsible for exogenous colonisation/infection post-tracheotomy.
Half the population carried abnormal flora in the oropharynx, P aeruginosa being the predominant potential pathogen. 37% were carriers of S aureus sensitive to methicillin, S pneumoniae and M catarrhalis were present in 9% of patients, while 11% of the children were oropharyngeal carriers of H influenzae. The number of “community” PPM (S pneumoniae, M catarrhalis, H influenzae, E coli and S aureus) significantly increased following tracheotomy. In contrast, there was no change in the number of abnormal “hospital” bacteria.
The number of patients whose lower airways were colonised/infected post-tracheotomy (39/45, 86%) was significantly higher than in the same population on transtracheal ventilation (29/45, 53%). “Community” bacteria were significantly more prevalent during the period of ventilation via a tracheotomy than during the PICU stay. In contrast, during transtracheal ventilation on the PICU significantly more abnormal opportunistic bacteria were isolated from the lower airways than “hospital” microbes following placement of a tracheotomy.
So long as the child enjoys reasonably good health, the abnormal carrier state of “hospital” bacteria is low (<5%).12 Illness severity is thought to promote abnormal flora. In this study half of the patients were so ill that they were unable to clear abnormal flora from the oropharynx. One third of the study population carried S aureus, in line with the carrier state of healthy children.17S pneumoniae, H influenzae, and M catarrhalis carriage (about 10%) was lower than the normal healthy population (25%).18,19 The healthy state implies the absence of receptors on the oropharyngeal mucosae for adherence of abnormal hospital bacteria. It is hypothesised that a fibronectin layer covering the mucosal cell surface protects the host from the adherence of abnormal bacteria.20
When the flora during the two modes of ventilation were compared, “hospital” bacteria were more prevalent during transtracheal ventilation while “community” organisms were more prevalent during ventilation via a tracheotomy. Children who undergo a tracheotomy are more stable than on admission. The fact that children do not acquire abnormal flora while on the respiratory ward where it is known that there is a high exposure to “hospital” bacteria reflects their recovering health. In a study of adult patients with acute respiratory failure who required mechanical ventilation the abnormal oropharyngeal carrier state returned to control levels within 4 weeks of discharge from hospital.21 The design of our study meant that we were unable to determine whether tracheotomised children would ultimately clear the abnormal bacteria.
Our study population acquired S aureus. This is in sharp contrast with studies of tracheotomised adult patients who invariably acquire abnormal AGNB including P aeruginosa,22S marcescens,23 and Acinetobacter baumannii.24 There are two possible explanations which relate either to the host or the microorganism. In the adult studies the external sources did not contain S aureus but only typical “environmental” bacteria such as Pseudomonas, Acinetobacter, and Serratia spp. These studies might report outbreaks with a particular microorganism during the trial. Alternatively, adults may possess fewer receptor sites for S aureus. Most of the adults studied were older than 60 years and were suffering from chronic underlying conditions such as diabetes, alcoholism, COPD, and malignancies.13–15,25 These abnormalities have been associated with significantly higher rates of carriage and colonisation by AGNB. Macrophages are thought to release elastase in response to these underlying chronic diseases. Elastase is subsequently released in the saliva and denudes the mucosa of fibronectin, making receptor sites available for AGNB. Fibronectin possesses attachment sites for community bacteria including S pneumoniae and S aureus.26
In summary, while P aeruginosa present in the flora on admission caused primary endogenous colonisation/infection during mechanical ventilation on the PICU, S aureus not carried in the throat was responsible for the exogenous colonisation/infection once the patients had undergone a tracheotomy. This observation has important implications for the choice of antibiotic used to treat these patients, and also for the prevention of both these types of infections.
REFERENCES
Footnotes
-
Financial involvement: none.
-
Competing interests: none.