Article Text

Abstract
Background: Opioids are commonly used to treat dyspnoea in palliative medicine but there has been no formal evaluation of the evidence for their effectiveness in the treatment of dyspnoea. A systematic review was therefore carried out to examine this.
Methods: The criteria for inclusion required that studies were double blind, randomised, placebo controlled trials of opioids for the treatment of dyspnoea secondary to any cause. The methods used to identify suitable studies included electronic searching of the literature, hand searching of the literature, and personal contact with relevant individuals and organisations. Random effects meta-analyses were performed on all included studies and on various subgroups (studies involving nebulised opioids or patients with chronic obstructive pulmonary disease (COPD)). Subgroups were compared using meta-regression. Some studies included in the systematic review could not be included in the meta-analysis because insufficient data were presented.
Results: Eighteen studies fulfilled the criteria for the review. The meta-analysis showed a statistically significant positive effect of opioids on the sensation of breathlessness (p=0.0008). Meta-regression indicated a greater effect for studies using oral or parenteral opioids than for studies using nebulised opioids (p=0.02). The subgroup analysis failed to show a positive effect of nebulised opioids on the sensation of breathlessness. The results of the subgroup analysis of the COPD studies were essentially similar to the results of the main analysis.
Conclusion: This review supports the continued use of oral and parenteral opioids to treat dyspnoea in patients with advanced disease. There are insufficient data from the meta-analysis to conclude whether nebulised opioids are effective, but the results from included studies that did not contribute to the meta-analysis suggest that they are no better than nebulised normal saline.
- dyspnoea
- opioids
- palliation
- meta-analysis
Statistics from Altmetric.com
Dyspnoea has been defined as “a subjective sensation of difficulty in breathing”.1 It is a common symptom in patients with advanced disease of mixed aetiology including cancer, respiratory disease, cardiac disease, and neuromuscular disease. The Regional Study of Care for the Dying (RSCD) reported a prevalence of dyspnoea of 54% in patients dying of cancer,2 and of 61% in patients dying of cardiac disease.3 The RSCD also reported that dyspnoea was “very distressing” in 50% of cancer patients and in 43% of cardiac patients.
Dyspnoea in patients with advanced disease may be managed effectively by treating the underlying cause of the dyspnoea, such as pleural effusion or anaemia, but in many cases there is no further treatment for the underlying cause. In many other cases such treatment is deemed inappropriate because of the patient’s poor clinical state. Symptomatic treatment may involve the use of both non-pharmacological methods and pharmacological agents.1 Non-pharmacological methods such as relaxation techniques and breathing training can be useful,4 but most patients require the additional use of pharmacological agents. Although a variety of different drugs have been used in the palliation of breathlessness, including opioids, benzodiazepines, phenothiazines and cannabinoids, there is relatively little evidence to support the use of these agents in this situation.
Opioids are commonly used to treat dyspnoea in palliative medicine. Individual studies have been undertaken to assess their efficacy, but there has been no formal evaluation of the evidence as a whole. Our objective was therefore to review systematically the evidence for the effectiveness of opioids in the management of dyspnoea. A version of this review has been published in the Cochrane Library.5
METHODS
The criteria for inclusion in the review were that studies should be double blind, randomised, placebo controlled trials. Patients suffering from dyspnoea caused by any disease were included. The intervention was any opioid, given in any dose, by any route with the intention of alleviating breathlessness.
The methods used to identify suitable studies included electronic searching of the literature, hand searching of the relevant literature, and personal contact with relevant individuals and organisations. Both published and unpublished data were eligible for inclusion in the study.
The electronic databases searched were: Medline on Silver Platter (1966 to 4/1999); Embase on Silver Platter (1980 to 5/1999); Cancercd on Silver Platter (1988 to 5/1999); CINAHL on Silver Platter (1982 to 5/1999); Cochrane Controlled Trials Register; Cochrane Database of Systematic Reviews; Dissertation Abstracts on Silver Platter; and SIGLE. The search strategy was of the form “(opioids OR synonyms) AND (breathlessness OR synonyms)” and used both MeSH terms and free text. Full details of the search strategy are included in the Cochrane review.5
Hand searching was performed on the reference lists of papers included in the systematic review, on review articles on the management of dyspnoea, and on relevant chapters in core textbooks on palliative medicine. Personal contact was made with the authors of papers included in the systematic review, recognised experts in the field, and the national and European palliative care organisations.
The results from the various searches were merged into a core database using the Reference Manager (Version 8) bibliographic software package. The abstracts of each article were reviewed and relevant studies identified.
The full text articles were reviewed independently by two investigators (ALJ, AD) who assessed the eligibility of the studies and recorded relevant data about the studies on a specifically developed proforma. The Jadad scale (box 1) was used to assess reporting of study quality (range 1–5).6 Concealment of allocation was assessed according to criteria used by the Cochrane Collaboration.5 Differences between the two investigators were resolved by consensus or by consultation with a third reviewer (JH). The authors of articles were approached about the existence of additional data if insufficient data were presented in the articles.
Box 1 Jadad scale
The Jadad scale6 assesses the quality of reporting of a controlled trial in three domains:
Description of randomisation (1 point if mentioned, 2 points if described and appropriate).
Description of double blinding (1 point if mentioned, 2 points if described and appropriate).
Description of withdrawals and dropouts (1 point if described).
The primary outcome measure was a subjective assessment of dyspnoea. In studies of patients at rest the breathlessness measurement recorded nearest to 1 hour after administration of the drug was used, in studies involving exercise tests the breathlessness measure that related to the exercise test was used, and in multiple dosing studies a breathlessness measure relating to an exercise test carried out at the end of each treatment period was used. In one study no such exercise test was carried out and the oxygen cost diagram was used as a breathlessness measure.
In the meta-analysis we used dyspnoea measures that were recorded at a fixed point during exercise or after a fixed length of exercise, and not those that were recorded at maximal exercise. For patients whose exercise tolerance is limited by breathlessness, the breathlessness score at maximal exercise is likely to be the maximum score, whatever the intervention. It was therefore felt that reporting a score at the end of exercise or at maximal exercise rather than at a fixed point during exercise did not give useful information when comparing a treatment against placebo. Studies which did not report this information were included in the review but excluded from the meta-analysis.
The secondary outcome measure was exercise tolerance expressed as exercise duration, distance walked, or maximum power output. Data were also collected on quality of life, arterial blood gases, oxygen saturation, and treatment related side effects.
A meta-analysis was performed for the primary and secondary outcomes where sufficient/suitable data were presented. Results from both periods of crossover trials were used since carry over of effects from one period to another was not considered to be a serious problem. Where more than one dose of the study drug was used, the mean of all doses was used in the meta-analysis. Standardised mean differences (SMD) were used for breathlessness and exercise tolerance since comparable outcomes were measured on different scales. SMDs were signed so that negative values indicated a benefit of opioids.
Clinical heterogeneity was examined before performing the meta-analysis but did not prevent the combination of results. Random effects meta-analyses were undertaken in preference to fixed effect analyses in order to account for residual variation between studies. Subgroup analyses were specified “a priori” and were carried out on studies using nebulised opioids (on the basis that nebulised opioids may exert an effect via a different mechanism—namely, local opioid receptors in the lung) and on studies involving patients with chronic obstructive pulmonary disease (COPD). Differences between subgroups were investigated using meta-regression.7
Paired analyses of crossover trials were undertaken using methods and assumptions described by Elbourne et al.8 When paired analyses were unavailable, a conservative estimate of the correlation between opioid and placebo period outcomes was taken from another study in the same meta-analysis. As a sensitivity analysis, meta-analyses were repeated assuming zero correlation. Our conclusions were robust to the use of imputed correlations.
RESULTS
Eighteen studies fulfilled the inclusion criteria for the review.9–25 All the included studies had a crossover design. Nine studies involving the use of oral or parenteral opioids were identified and included in the review (table 1).9–16 The paper by Eiser et al11 reported the results of two separate studies and these were analysed separately. Oral opioids were used in eight of the studies but in the study by Bruera et al9 subcutaneous morphine was given. Nine studies involving the use of nebulised opioids were identified and included in the review (table 2).17–25 One of these studies25 included data only on exercise tolerance and not on breathlessness. Five of the studies were not included in the meta-analysis either because data were presented with inadequate detail to allow relevant parameters to be calculated,18,23 or because the breathlessness measure was not measured or not reported at a fixed point during exercise.17,20,21
Characteristics of oral and parenteral opioid studies
Characteristics of nebulised opioid studies
Sixteen of the 18 studies scored 4 out of a possible 5 on the Jadad scale for quality. The reason for submaximal scores was that the methods of randomisation were not described in any of the studies. The method of allocation concealment was classified as “unknown” for every study.
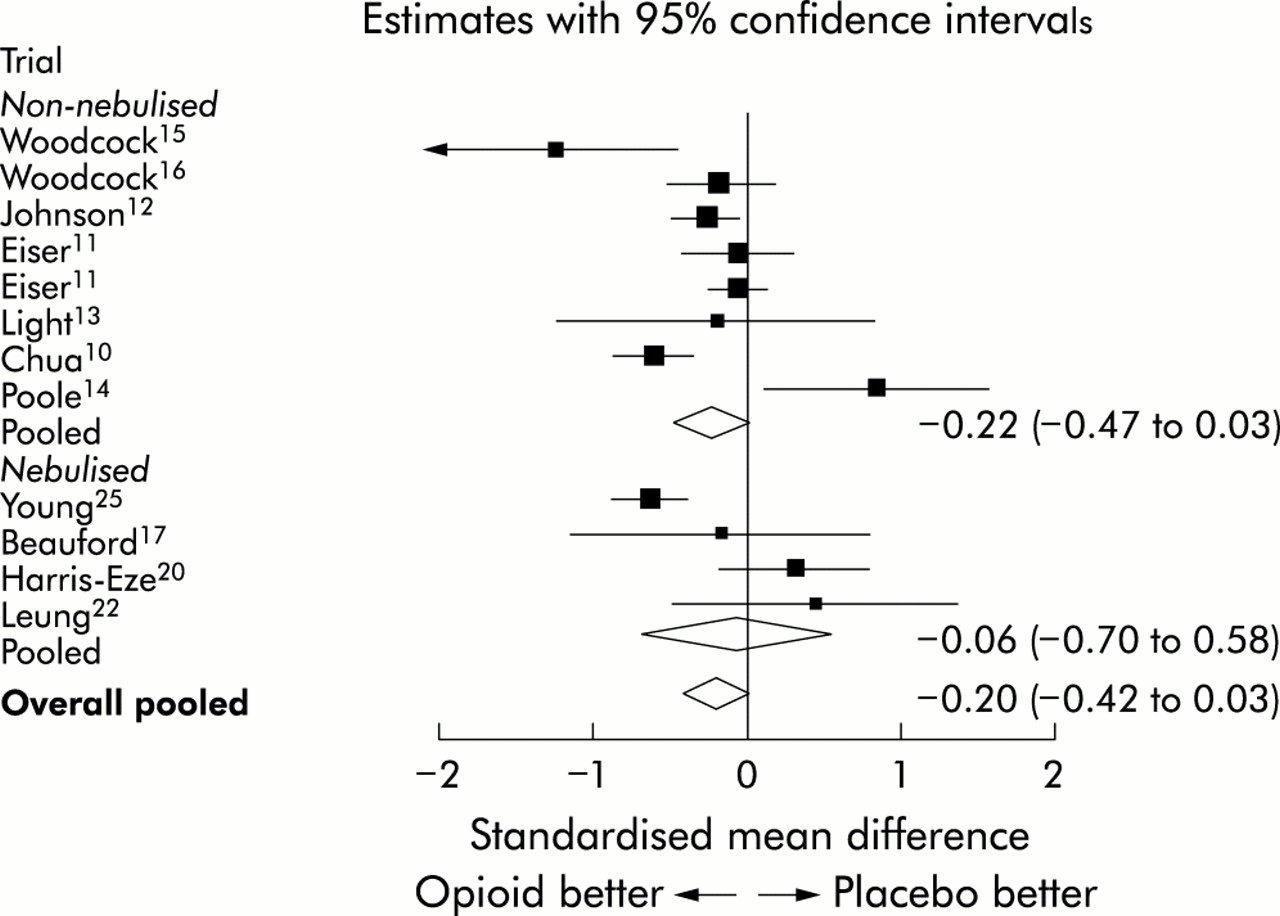
The meta-analysis showed a highly statistically significant positive effect of opioids on the sensation of breathlessness (fig 1, table 3). There was statistically significant heterogeneity between the results of the studies, although the direction of the effect was consistent. Meta-regression showed a greater effect for the studies using oral or parenteral opioids than for those using nebulised opioids (p=0.02). Indeed, subgroup analysis of the three included nebulised studies failed to show a positive effect,19,22,24 Moreover, none of the five excluded nebulised studies that measured breathlessness reported a positive effect.17,18,20,21,23 The results of the subgroup analysis for the COPD studies were essentially similar to those of the main analysis. The meta-analysis did not demonstrate a significant positive effect for opioids on exercise tolerance (fig 2, table 4).
Dyspnoea results
Exercise tolerance results
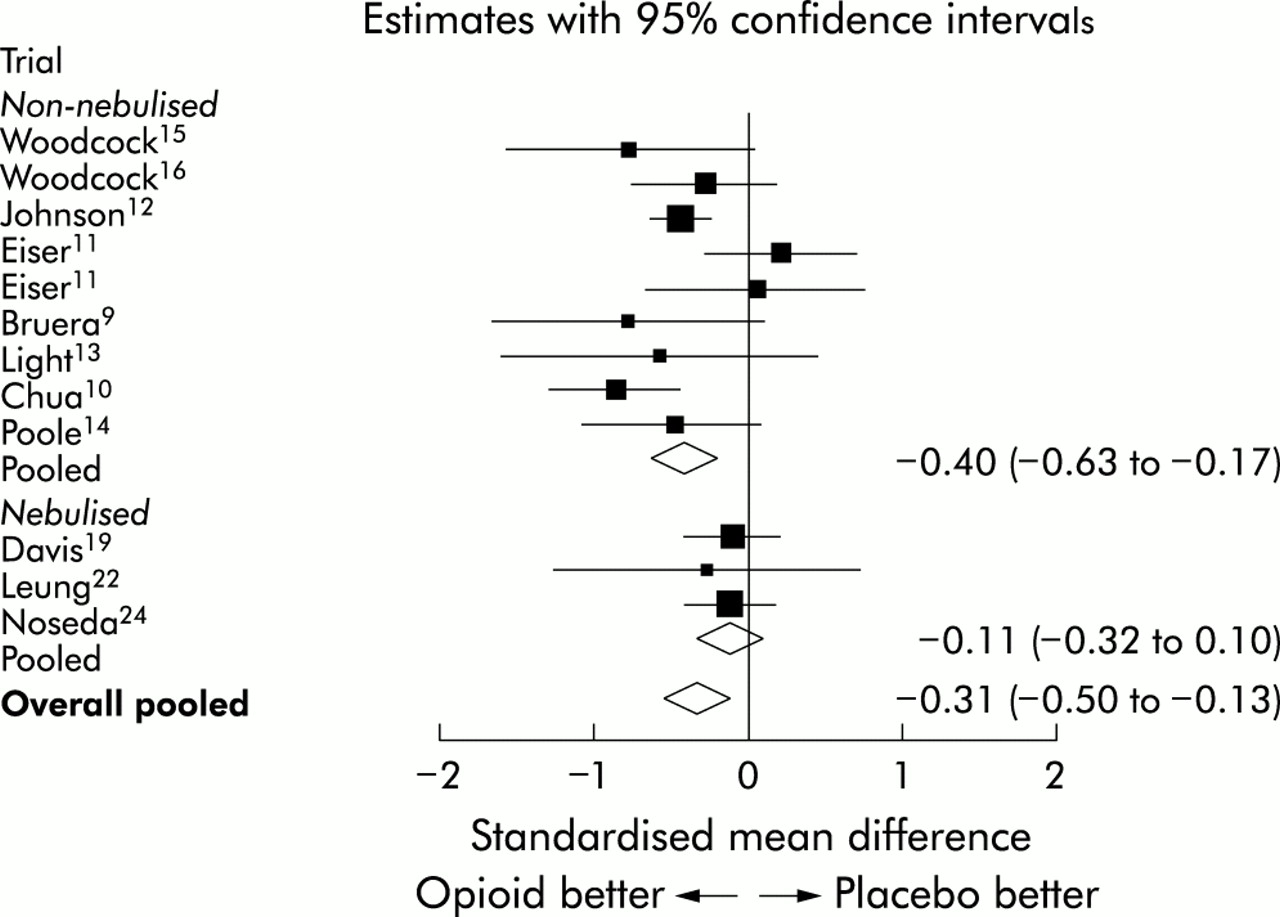
Meta-analysis of dyspnoea outcomes (grouped by route of administration) using standardised mean differences. Changes from baseline within each treatment period were selected in preference to post-treatment measures when both outcomes were available.

{kind=link}
{kind=link}
Meta-analysis of exercise tolerance outcomes (grouped by route of administration) using standardised mean differences. Changes from baseline within each treatment period were selected in preference to post-treatment measures when both outcomes were available.
Additional post-hoc subgroup analysis comparing single dose and multiple dosing studies was performed. There was no significant difference between the results from single dose studies and those from multiple dose studies.
Only one of the studies formally assessed quality of life.14 The authors of this study used the Chronic Respiratory Disease Questionnaire and found no difference in quality of life between the treatment phase and the placebo phase.
Adverse outcomes
Three patients died during the study by Noseda et al.24 The authors concluded that the deaths were not related to the study medication as the patients had very advanced disease and the deaths occurred some time after the study medication had been given (during the night).
The side effects reported with oral opioids were drowsiness, nausea, vomiting, dizziness and constipation and, in two of the four multiple dosing studies, an opioid withdrawal syndrome.
Multiple dosing studies in opioid naïve patients had most problems with adverse effects. In one multiple dose study16 five of 16 patients withdrew because of nausea and vomiting after taking dihydrocodeine, two were constipated and drowsy on the opioid, and two had symptoms of withdrawal after stopping the opioid. In the multiple dose study by Eiser et al11 three of 14 patients complained of constipation or vomiting and “several others” complained of mild nausea. In the study by Poole et al14 there was no difference in the overall incidence of adverse effects but subjects were significantly more likely to report nausea, anorexia, constipation, or drowsiness while receiving morphine. Two of 16 patients withdrew while receiving morphine, one with an infective exacerbation of COPD and one with severe constipation and shakiness secondary to morphine. An opioid withdrawal syndrome was seen in four patients when they stopped taking morphine. In the multiple dose study by Johnson et al,12 however, there was no difference in drowsiness, nausea and constipation between the opioid and placebo groups. Information on withdrawals from studies is summarised in table 5.
Withdrawals/drop outs from studies
In one study using nebulised morphine,24 three patients had minor side effects involving a bitter taste in the mouth, cough, and a pricking sensation in the throat. This same pricking sensation in the throat was also experienced by the same patient with nebulised normal saline. In the other studies using nebulised morphine there were no significant problems with side effects of opioids.
Four studies measured arterial blood gas tensions as part of the protocol.11,16,18 One study involving patients with COPD reported a statistically significant increase in Paco2 during the treatment phase on dihydrocodeine 30 mg three times a day and 60 mg three times a day,16 but in no instance did the Paco2 rise above 5.3 kPa (40 mm Hg) or the Pao2 fall significantly. The other studies reported no significant changes in arterial blood gas tensions during treatment. Nine studies measured oxygen saturation as part of their protocol9–11,13,14,20,21,23,24; none reported a significant change in oxygen saturation during the treatment phase.
No information about cost was recorded. However, the cost of all the drugs used is small and does not vary significantly between drugs.
DISCUSSION
The literature search identified nine trials involving the use of oral or parenteral opioids. These studies were all small in size, with the largest consisting of only 19 patients.12 The literature search also identified nine trials which studied the use of nebulised opioids. These studies were again small in size, with the largest consisting of only 79 patients.19 The total number of patients included in the oral or parenteral studies was 116, while the total number of patients included in the nebulised studies was 177. The studies gave broad details of patient diagnoses (tables 1 and 2) but there was little comment about the potential benefits of opioids in relation to the causes of breathlessness.
This review has found a highly statistically significant effect for oral and parenteral opioids in the management of dyspnoea. The clinical significance of these results can be ascertained by multiplying the overall standardised mean difference by the individual study’s standard deviation. In the study by Johnson et al,12 for example, this represents a difference of approximately 8 mm (on a 100 mm visual analogue scale) between the opioid and placebo treatment periods.
The clinical effect of oral and parenteral opioids appears to be relatively small. However, certain pharmacological aspects need to be considered, including the fact that (a) the opioid doses were relatively small in some of the studies12; (b) the doses were not titrated in any of the studies; (c) the dosing intervals were probably too long in some of the studies11,16; and (d) the opioids would not have reached steady state in the single dose studies.10,11,13,15
This review did not find a statistically significant effect for nebulised opioids in the management of dyspnoea. In the at rest studies there was some improvement in dyspnoea after nebulised morphine, but this was not significantly different from that seen after nebulised saline.19,24 However, nebulised normal saline may not be a true placebo as it has a variety of non-specific actions in patients with dyspnoea,26 including stimulation of facial nerve endings27 and liquefaction of tenacious secretions.28
There was no evidence to indicate that the use of opioids was associated with a deleterious effect on arterial blood gases or oxygen saturation in the patient populations studied. The side effects reported were typical of this group of drugs.29 They should be relatively easy to treat, and should not necessitate the discontinuation of the opioid. In addition, the side effects should be anticipated and prophylactic treatment such as antiemetics and laxatives prescribed.
The possible mechanisms of action of opioids include reduction in the central perception of dyspnoea (similar to the reduction in the central perception of pain), reduction in anxiety associated with dyspnoea, reduction in sensitivity to hypercapnia, reduction in oxygen consumption, and improved cardiovascular function.1,30 It is likely that the influence of these different mechanisms varies in different patients. Although opioid receptors are present throughout the lungs, the results of the nebulised opioid studies suggest that these receptors have little effect in the sensation of breathlessness.
In conclusion, this review supports the continued use of oral and parenteral opioids to treat dyspnoea in patients with advanced disease. There is evidence that oral and parenteral opioids are more effective than nebulised opioids. The data from the meta-analysis are insufficient on their own to conclude whether nebulised opioids are effective, but data from included studies that did not contribute to the meta-analysis do not support their continued use. More research is needed to ascertain the most appropriate treatment regimen. This research needs to be based on sound pharmacological principles and appropriate standardised methods of assessment of dyspnoea and of quality of life are needed.
Acknowledgments
The authors would like to acknowledge the contribution of the other members of the Steering Group: Professor L Adams (Imperial College, London), Dr R A’Hern (Royal Marsden Hospital, London), Dr F Cowan (University College, London), Dr C Davis (Southampton General Hospital, Southampton), Dr W Wedzicha (London Chest Hospital, London), and Dr A Wilcock (Hayward House, Nottingham). They would also like to acknowledge the contribution of the Systematic Review Training Unit, Institute of Child Health, London, and of the Cochrane Pain, Palliative Care and Supportive Care Group. This review was sponsored by the Palliative Care Research Fund of the Royal Marsden Hospital, London and by a donation from the Sackler Foundation.
REFERENCES
Footnotes
-
This paper is based on a Cochrane review published in The Cochrane Library 2002, Issue 1 (see www.CochraneLibrary.net for information). Cochrane reviews are regularly updated as new evidence emerges and in response to comments and criticisms from readers. The Cochrane Library should be consulted for the most recent version of the review.