Article Text

Abstract
Background: Published data on the frequency and types of flexible bronchoscopic airway appearances in children with non-cystic fibrosis bronchiectasis and chronic suppurative lung disease are unavailable. The aims of this study were to describe airway appearances and frequency of airway abnormalities and to relate these airway abnormalities to chest high resolution computed tomography (cHRCT) findings in a cohort of children with non-cystic fibrosis chronic suppurative lung disease (CSLD).
Methods: Indigenous children with non-cystic fibrosis CSLD (>4 months moist and/or productive cough) were prospectively identified and collected over a 2.5 year period at two paediatric centres. Their medical charts and bronchoscopic notes were retrospectively reviewed.
Results: In all but one child the aetiology of the bronchiectasis was presumed to be following a respiratory infection. Thirty three of the 65 children with CSLD underwent bronchoscopy and five major types of airway findings were identified (mucosal abnormality/inflammation only, bronchomalacia, obliterative-like lesion, malacia/obliterative-like combination, and no macroscopic abnormality). The obliterative-like lesion, previously undescribed, was present in 16.7% of bronchiectatic lobes. Structural airway lesions (bronchomalacia and/or obliterative-like lesion) were present in 39.7% of children. These lesions, when present, corresponded to the site of abnormality on the cHRCT scan.
Conclusions: Structural airway abnormality is commonly found in children with post-infectious bronchiectasis and a new bronchoscopic finding has been described. Airway abnormalities, when present, related to the same lobe abnormality on the cHRCT scan. How these airway abnormalities relate to aetiology, management strategy, and prognosis is unknown.
- bronchiectasis
- bronchoscopy
- children
- airway lesions
Statistics from Altmetric.com
Bronchoscopy, an important tool for respiratory physicians, is increasingly used for diagnostic, therapeutic, and research purposes. In paediatrics indications for flexible bronchoscopy include prolonged cough and recurrent respiratory infections where airway abnormalities such as tracheobronchomalacia may be found.1–3 An objective definition of bronchomalacia is not currently available and bronchoscopy remains the current “gold standard” for establishing the diagnosis.2 In children with localised bronchiectatic changes, bronchoscopy is indicated to evaluate the possibility of obstructive causes such as foreign bodies.
Chronic suppurative lung disease (CSLD), undefined in standard paediatric respiratory textbooks,4,5 is used by clinicians to describe children who have had a productive and/or moist cough for a prolonged period of time. CSLD encompasses a range of diseases such as cystic fibrosis, primary ciliary dyskinesia, idiopathic lung abscess, and bronchiectasis where chest high resolution computed tomographic (cHRCT) scanning has replaced bronchography as the gold standard for defining bronchiectasis.6 cHRCT abnormalities in bronchiectasis are well described and scoring systems have been developed.7 In contrast, there are no published data (Medline search 1966 to November 2001) that describe bronchoscopic appearances or the frequency of airway lesions in children with non-cystic fibrosis bronchiectasis and CSLD. In Stradling’s book8 a number of airway appearances are described: bronchial displacement associated with lobar collapse, mucosal abnormalities (inflammation, atrophic mucosa, and secretions and bleeding), and descriptions of chronic and acute bronchitis (flaccidity and hypertrophy of elements in wall, longitudinal corrugations, mucosal reddening, increased vascularity, dilated ducts).
This study was undertaken to describe airway appearances and frequency of airway abnormalities and to relate these airway abnormalities to cHRCT findings in a cohort of children with non-cystic fibrosis CSLD.
METHODS
Study subjects
Indigenous children with non-cystic fibrosis CSLD (>4 months moist and/or productive cough) were prospectively identified and collected over a 2.5 year period (June 1999 to December 2001) at two centres. Their medical charts were retrospectively reviewed. Only those who had undergone bronchoscopic evaluation were included in the study. Reasons for bronchoscopic examination were clinically based: (A) recurrent (≥2 episodes) pneumonia in the same lobe, (B) exclusion of foreign body when cHRCT scan showed single lobe involved, (C) chronic (>3 months) collapse of one or more lobes on the chest radiograph, (D) assessment of airway anatomy when recurrent clinical aspiration present, (E) assessment of upper airway in the presence of stridor, and (F) clinical picture not compatible with HRCT findings.
The study was part of a larger clinical review and was approved by the local institution’s human ethics committee.
Bronchoscopic examination
Flexible bronchoscopy (Pentax FB10) was performed under general gaseous anaesthesia in all children by the same respiratory paediatrician (ABC) when the child was in a stable state (elective admissions). The vocal cords were sprayed with xylocaine and the child breathed spontaneously throughout the procedure; positive end expiratory pressure was not usually applied except during periods of assessment of malacia. The bronchoscope was passed into the airway through a port in the connector to the face mask. Anatomical sites and the type of lesion were evaluated after gentle suctioning (if necessary) and recorded to the relevant third airway generation.9 The classification of airway generations used was that outlined by Nunn.9 To assess airway obliteration or closure, 10 ml of air was rapidly injected via the suction channel and the bronchus was considered to be obliterative-like when the airway opening was absent or markedly reduced (compared with the adjacent segmental opening). Bronchoscopic airway lavage (BAL) fluid was obtained using 10 ml saline instilled into the most macroscopically inflamed bronchus and suctioned into a mucus trap. Specimens were cultured locally and differential cell counts were performed by an external cytology service.
HRCT scanning
cHRCT scanning was performed in the prone position with images taken at suspended inspiration under general anaesthesia if necessary in children unable to cooperate with the breath holding manoeuvre. All cHRCT scans were assessed by a paediatric radiologist (JPM) who was unaware of the children’s clinical data. Bronchiectasis was diagnosed if the inside bronchial diameter was greater than that of the adjacent (apparently normal) artery (ratio >1). Bronchi with mucus plugging (no air content) and clearly larger (not including irregular interstitial disease) than the adjacent artery were included. Occasional mildly abnormal bronchi as isolated findings with otherwise normal findings were not included.7 When radiological features were absent, children were considered to have clinical CSLD.
Analysis of data
The χ2 test was used to examine the relationship between airway abnormalities and abnormalities on the cHRCT scan and a two-tailed p value of <0.05 was considered significant.
RESULTS
All but two children were from Central Australia. Of the 65 children with CSLD, 33 underwent bronchoscopic evaluation. The median age of these 33 children (18 female) at diagnosis was 3.8 years (range 0.6–14.9). The median percentage predicted forced expiratory volume in 1 second (FEV1) in children who could perform spirometric tests (n=10) was 65% (range 42.3–87) and the forced vital capacity (FVC) was 70% (54.5–85.8). Twenty eight of the children had radiological bronchiectasis and five had clinical CSLD. Haemoptysis was absent in all children. In all but one child the aetiology of the bronchiectasis was presumed to be following respiratory infection (table 1).
Characteristics of study subjects
In the 28 children with radiological bronchiectasis, 12 had one bronchiectatic lobe, 14 had two, and two had three, giving a total of 48 bronchiectatic lobes. The most common lobe involved was the left lower lobe (n=18, 34%), followed by the right lower lobe (n=11, 20.8%), the right middle lobe (n=9, 17%), the right upper lobe (n=6, 11.3%), the left upper lobe, and the left lingula (each n=2, 3.8%). When bronchomalacia was present it occurred at either the lobar (2–3rd generation) or segmental (4th generation) bronchi, whereas obliterative lesions were only seen in the segmental or subsegmental (5th generation) bronchi. Five major airway types were identified: I (mucosal abnormality/inflammation only), II (bronchomalacia, fig 1), III (obliterative-like, fig 2), IV (malacia/obliterative-like combination), and V (no abnormality). The most frequent abnormality was type I (n=28, 58.3%), followed by types II (n=9, 18.8%), III (n=8, 16.7%), IV (n=2, 4.2%), and V (n=1, 2.1%). All of these bronchial abnormalities, when present, corresponded to the site of abnormality on the HRCT scan. Specific airway types were not related to any specific lobe (p=0.49). Of the five children with CSLD, three had type I airway abnormality, one had bronchomalacia, and one had macroscopically normal airways. When combined, structural airway lesions were present in 39.7% of children.

Bronchomalacia (airway type II) of the right middle lobe (child 7 in table 1).
{kind=link}
{kind=link}
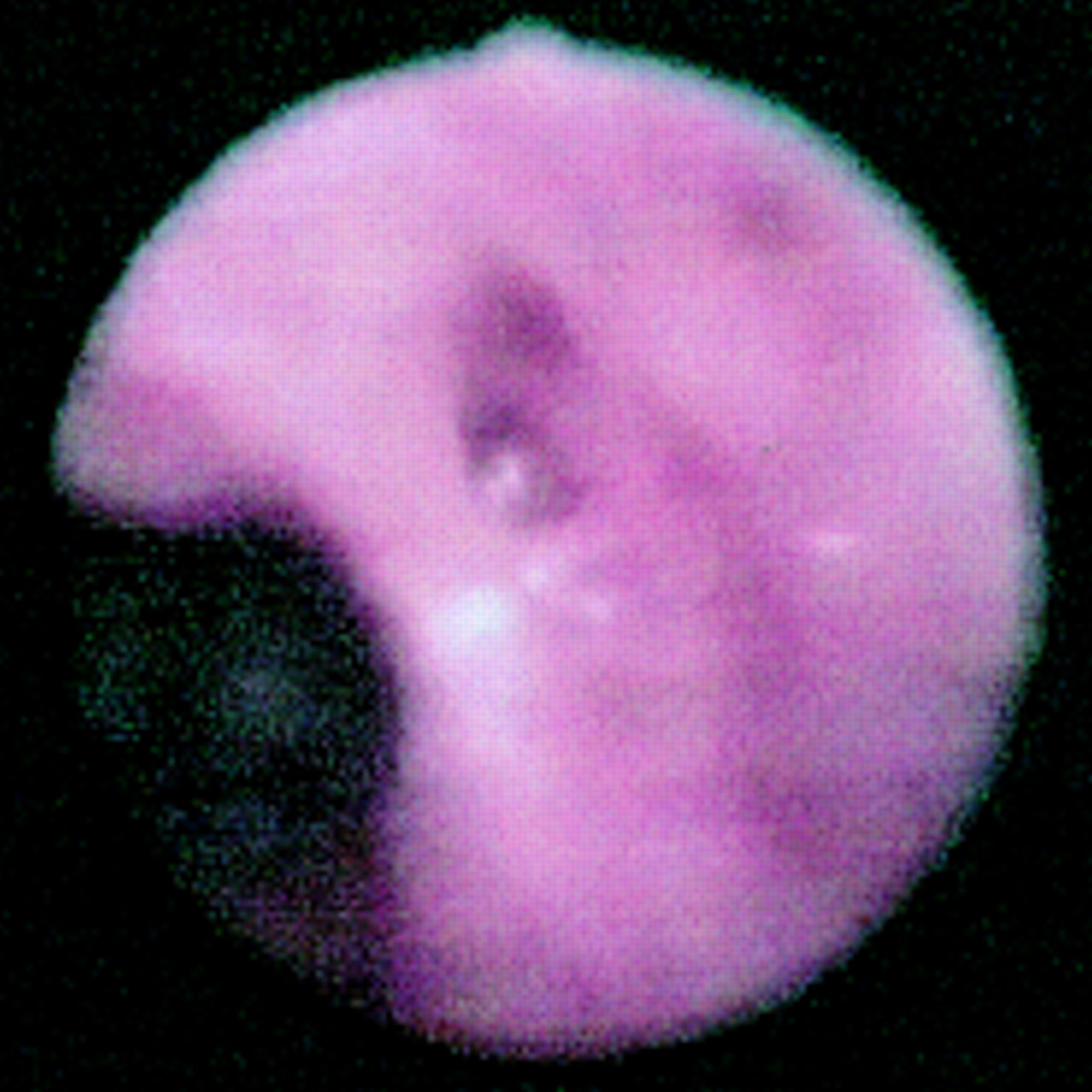
Obliterative-like lesion (airway type III) seen in the segmental bronchus (middle of picture) while the adjacent bronchus is widely patent and more inflamed (child 9 in table 1).
In the BAL fluid the median percentage of neutrophils, macrophages, and lymphocytes was 69.5% (range 18–98), 16.5% (range 2–71), and 6% (range 0–50), respectively. Eosinophils were not found in any specimen. Single organisms were isolated from seven specimens (Haemophilus influenzae (n=5), Mycobacterium tuberculosis (n=1), Candida (n=1)). In four specimens two organisms were cultured (H influenzae and Streptococcus pneumoniae in three, S pyogenes and M catarrhalis in one). Cultures were negative in the remaining 22 specimens.
DISCUSSION
We have shown that flexible bronchoscopy large airway findings in children with non-cystic fibrosis bronchiectasis can be macroscopically grouped into five types and that an obliterative-like lesion, a previously undescribed airway abnormality, can be found in these children.
The rarity of non-cystic fibrosis bronchiectasis in industrialised societies is attributed to improvements in living conditions, nutrition, universal immunisation, and availability of antibiotics.10 There are appreciable social inequities and difficulties within healthcare services for indigenous Australians,11,12 and it is not surprising that bronchiectasis is common (prevalence of at least 4.2 per 1000 children, unpublished observation) in remote indigenous Australians, the most severely disadvantaged group.12 As non-cystic fibrosis bronchiectasis is now rare in developed countries, it is not surprising that, despite the wide use of bronchoscopy in children, published data on airway lesions in non-cystic fibrosis bronchiectasis are unavailable. The descriptions by Stradling8 of various possible findings in bronchiectasis, acute and chronic bronchitis have been listed in the introduction. In this study we have found that accompanying airway lesions are common (39.7%) in this group of children with post-infectious bronchiectasis. Bronchomalacia associated with bronchiectasis is thought to be related to chronic inflammation,13 although it is unknown if these malacia lesions predate the recurrent respiratory infections. It is well known that children with bronchomalacia are prone to recurrent respiratory infections.2 Lobar differences in airway inflammation and infection have been described.14 Whether the different types of airway lesions reflect the intensity of infection and/or inflammation is unknown. Higher by-products of the inflammatory cascade have been shown to be related to disease severity in adults with bronchiectasis.15 How these airway lesions relate to prognosis is also unknown. Airway malacia disorders can lead to secretion retention2 and subsequent infection, and it can be postulated that lobes with accompanying airway structural abnormalities may have a worse prognosis than those without any accompanying abnormality, as physiologically these airway lesions impede removal of airway secretions.2
A macroscopic obliterative-like lesion, previously undescribed, was found in our cohort of children. Why this has never previously been described and occurred in our cohort is subject to speculation. Firstly, flexible bronchoscopy only became widely available in the last two decades whereas non-cystic fibrosis bronchiectasis, termed an “orphan” disease because of its perceived rarity and limited published research,16 markedly declined 30–40 years ago in countries where flexible bronchoscopy is readily available.10 Secondly, indigenous children living in remote communities have early nasal bacterial colonisation, chronic nasal discharge, and high rates of nasal bacterial carriage,17 factors that may contribute to the intensity and persistence of neutrophilic inflammation, a known major contributor of airway destruction.15 In animal studies it is known that infection is necessary for the development of bronchiectasis.18 Thirdly, the neutrophilic inflammatory response of indigenous children has been found to be increased or exaggerated19 and genetic polymorphism differences in proinflammatory and metabolising enzymes have recently been described in a group of indigenous Australians.20,21 These factors may contribute to ongoing airway destruction.
Whether airway obliteration can be found in other disease processes is unknown but, anecdotally, our collective experience of over 1500 paediatric bronchoscopic examinations suggests that this particular airway finding is only found in children following infectious airway diseases (bronchiectasis and radiologically defined bronchiolitis obliterans22). The obliterative-like lesions described here are distinct from pathological and radiological definitions of bronchiolitis obliterans that has many possible aetiologies.13 We were unable to identify a predilection of specific airway lesions for specific lobes or associated cHRCT features. Whether certain clinical features such as rate of progression or frequency of exacerbation are associated with specific airway lesions cannot be determined in this study because of the small numbers and retrospective design. Bronchoscopy on all children with bronchiectasis is not advocated and remains a clinical decision. A prospectively collected clinical profile of these children comparing lobes with and without airway lesions would be beneficial.
In conclusion, a structural airway abnormality is commonly found in children with post-infectious bronchiectasis and a new bronchoscopic finding has been described. Airway abnormalities, when present, related to the same lobe abnormality as that seen on the cHRCT scan. How these airway abnormalities relate to aetiology, management strategy, and prognosis is unknown and deserves further research.