Article Text

Abstract
The presentation of syphilitic aortitis is often atypical and available serological tests are non-specific. The diagnostic gold standard remains direct identification of microorganisms in tissue. We present a case of syphilitic aortitis that presented as a mediastinal mass and report the use of polymerase chain reaction for Treponema pallidum to diagnose syphilitic aortic disease.
- syphilis
- aortic aneurysm
- polymerase chain reaction
Statistics from Altmetric.com
CASE REPORT
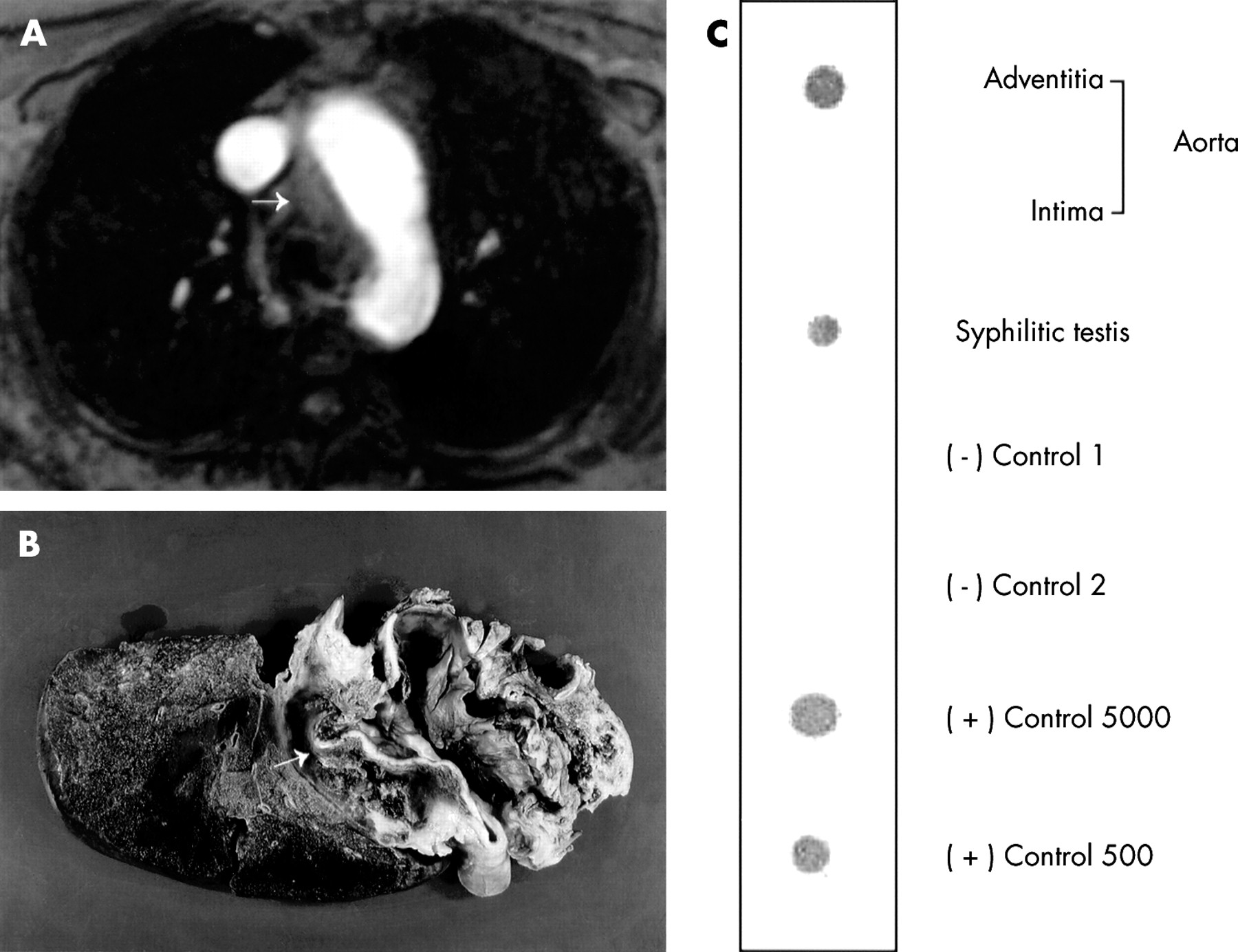
A 70 year old woman presented with acute onset of chest tightness and right shoulder discomfort. She had a history of essential hypertension. She was married, lived with her husband, had a 100 pack year smoking history, and a family history of lung cancer. There were no risk factors for HIV infection and no recent travel. Physical examination was normal. A diagnosis of myocardial infarction or aortic dissection was considered. The chest radiograph, electrocardiogram, and laboratory studies including cardiac enzymes were normal. Transoesophageal echocardiography revealed normal cardiac function and neither aortic dissection nor aneurysm formation. A chest MRI scan showed a diffuse, infiltrative, subaortic, extravascular mediastinal mass that displaced the trachea rightward (fig 1A, arrow). These findings were considered suggestive of malignancy. At fibreoptic bronchoscopy no endobronchial lesions were seen and no tumour cells or microorganisms were found in specimens of bronchial lavage fluid. The patient developed sudden massive haemoptysis and expired, despite aggressive resuscitative efforts. Necroscopic examination revealed an aneurysm of the ascending aorta that had ruptured into the right bronchus (fig 1B, arrow). “Tree barking” was evident in the aortic intima and suggested tertiary syphilis as the aetiology of the ruptured aneurysm.
{kind=link}
(A) MRI scan of the mediastinum showing an infiltrating mass displacing the trachea to the right (arrow). (B) Necropsy specimen revealing an ascending aortic aneurysm (arrow) that has ruptured into the right main stem bronchus. (C) Treponema pallidum PCR amplicons from the resected aorta and appropriate controls (see text) are confirmed by Southern blot analysis using a T pallidum specific oligonucleotide probe. Note that T pallidum DNA is present in the aortic adventitia but not in the aortic intima.
Before death a diagnosis of syphilitic aortitis had not been considered and thus serological studies for syphilis were not available. To confirm the diagnosis of syphilitic aortitis DNA was extracted from the adventitia and from the intima of the formalin fixed aorta and amplified by polymerase chain reaction (PCR) using oligonucleotide primers targeting the TpN47 gene of Treponema pallidum.1,2 As a positive control, DNA was extracted from paraffin embedded T pallidum infected rabbit testicular tissue and amplified. Separately, 5000 and 500 T pallidum genome equivalents were also amplified. As negative controls, these two reactions were carried out omitting T pallidum DNA. The presence of amplifiable human DNA in the clinical samples was confirmed with an independent PCR reaction for β-globin DNA. T pallidum amplicons were detected in the samples from the aortic adventitia, which contained the vasa vasorum, plus the three positive controls. Positive reactions were confirmed by Southern blot using a 32P-labelled internal oligonucleotide probe (fig 1C). No amplicon was detected in the sample from the aortic intima or from the negative controls.
DISCUSSION
Cardiovascular syphilis is rarely encountered and often omitted from the antemortem differential diagnosis. Its hallmark is aortitis which, by necropsy, may occur in 70–80% of patients with untreated syphilis and causes aortic valve insufficiency, coronary ostial stenosis, or ascending aortic aneurysm.3 Aneurysms usually expand anteriorly and rightward and can compress the bronchus or vasculature, or rupture into the bronchus, pleural space or pericardium. Luminal dilatation in syphilitic aneurysms can be difficult to detect by radiological studies because of the minute communications between the aortic lumen and the aneurysm or obliteration of the lumen by mural thrombus. In addition, contained rupture of the aneurysm or localised aortitis may form mass like lesions in the mediastinum.3 A non-vascular mediastinal mass is therefore often misdiagnosed in syphilitic aortitis. The pathological hallmark of syphilitic aortitis is “tree barking” or longitudinal wrinkling of the aortic media. This results from ischaemic necrosis and scarring of the aortic media due to an obliterative endarteritis of the vasa vasorum. “Tree barking” is not considered pathognomonic of syphilis and occurs in aortitis resulting from other diseases such as systemic lupus erythematosus.4 The diagnostic gold standard therefore remains direct identification of microorganisms in tissue.
Treponema pallidum can be detected in a sensitive and specific fashion in clinical specimens using a controlled PCR assay.2 This is the first such description in the aorta. The presence of T pallidum DNA in the adventitia and its absence in the intima is consistent with the classic localisation of syphilitic infection in the aortic vasa vasorum rather than in the aortic luminal wall. PCR can provide a rapid definitive diagnosis of spirochaetal infection when biopsy material is available and can confirm this diagnosis at necropsy in the setting of compatible pathology. The epidemic of primary syphilis in the United States in the early 1990s and the increased progression to tertiary syphilis in patients with HIV infection serves as a reminder that cardiovascular syphilis will still be encountered in the future.5