Article Text

Abstract
Background: There is evidence that the bronchial microcirculation has the potential to contribute to the pathophysiological mechanisms of exercise induced bronchoconstriction (EIB) in asthmatic subjects. Vascular endothelial growth factor (VEGF), which is highly expressed in asthmatic airways, increases vascular permeability. The relationship between VEGF levels in induced sputum and the severity of EIB in asthmatic subjects was studied.
Methods: The concentration of VEGF in induced sputum was examined in 23 asthmatic subjects and 11 normal controls. The asthmatic subjects performed an exercise test and the % maximal fall in forced expiratory volume in 1 second (FEV1) was measured. Beclomethasone dipropionate (BDP) 400 μg twice daily was administered to the asthmatic subjects for 8 weeks and the exercise test and sputum induction were repeated.
Results: The concentration of VEGF in induced sputum was significantly higher in asthmatic subjects than in normal controls. There was a significant correlation between the concentration of VEGF and the % maximal fall in FEV1 (r=0.826, p=0.0001) and between the concentration of VEGF and airway vascular permeability index (r=0.621, p=0.0037). After treatment with inhaled BDP there was a significant decrease in the concentration of VEGF in the asthmatic subjects (before treatment: 7051 (2361) pg/ml, after treatment: 4498 (2135) pg/ml, p<0.0001). The change in the concentration of VEGF was significantly correlated with the change in the % maximal fall in FEV1 (r=0.463, p=0.031).
Conclusions: Excessive production of VEGF in asthmatic airways may contribute to the pathogenesis of EIB via increased airway vascular permeability.
- vascular endothelial growth factor
- exercise induced bronchoconstriction
- bronchial asthma
Statistics from Altmetric.com
Exercise induced bronchoconstriction (EIB) is used to describe the increase in airway resistance that follows exercise in asthmatic patients. Two major hypotheses have been put forward to explain the mechanism of EIB. One suggests that evaporative water loss associated with exercise causes a transient increase in osmolarity of the fluid interface of the mucosal surface in the airways, resulting in mast cell degranulation.1 The second hypothesis proposes that EIB is a mechanical event in which the airways are rapidly rewarmed by reactive hyperaemia of the bronchial circulation with subsequent oedema of the airway wall.2 However, since mast cell derived mediators such as histamine and leukotrienes may cause airway oedema, it is possible that both of these hypotheses explain EIB in asthmatic subjects. There is no doubt that the bronchial microcirculation has the potential to contribute to the pathophysiological mechanisms of EIB in asthma.
Vascular endothelial growth factor (VEGF) is one of the most potent inducers of endothelial cell growth.3 It also increases vascular permeability,4 allowing plasma proteins to leak into the extravascular space leading to mucosal oedema and thereby narrowing of the airway diameter which could amplify the effects of airway smooth muscle contraction. VEGF is widely expressed in many highly vascularised organs including the lung.5 Hoshino et al6 recently reported that VEGF positive cells are significantly increased in the airway mucosa of patients with bronchial asthma compared with healthy control subjects. However, there have been no reports of the possible role of VEGF in EIB in asthma. We therefore examined the relationship between VEGF levels in induced sputum and the severity of EIB in patients with asthma.
METHODS
Subjects
Twenty three non-smoking asthmatic patients of mean (SD) age 34.8 (7.8) years, forced expiratory volume in 1 second (FEV1) 90.1 (5.4)% who satisfied the American Thoracic Society criteria for asthma participated in the study.7 Eleven healthy, life long non-smoking volunteers of mean (SD) age 34.1 (7.7) years, FEV1 106.6 (5.7)% with no history of lung disease formed the control group.
Methacholine inhalation challenge testing was performed in the patients with asthma. All challenge tests were performed at 13.00 hours to eliminate the effect of diurnal variation. Following baseline spirometric tests and inhalation of diluent to establish the stability of FEV1, the subjects were instructed to take slow inspirations in each set of inhalations. All the asthmatic patients had bronchial hyperreactivity to methacholine. Their regular medication consisted of β2 agonists and theophylline, and none were receiving oral or inhaled corticosteroids. Medications were not changed during the month before the study and were withdrawn for at least 12 hours before the methacholine challenge and exercise test. All patients were clinically stable and none had a history of respiratory infection for at least 4 weeks before the study.
All subjects gave their written informed consent for participation in this study which was approved by the ethics committee of Osaka City University, Japan.
Sputum induction and processing
Spirometric tests were performed before inhalation of 200 μg salbutamol via a metered dose inhaler. All subjects were instructed to wash their mouth thoroughly with water. They then inhaled 3% saline at room temperature, nebulised by an ultrasonic nebuliser (NE-U12; Omron Co, Tokyo, Japan) at maximum output. They were then asked to cough deeply at 3 minute intervals. After sputum induction the spirometric tests were repeated. If the FEV1 fell, the subjects were required to wait until it returned to baseline value. The sputum samples were kept at 4°C for no longer than 2 hours before further processing. A portion of the sample was diluted with phosphate buffer solution (PBS) containing 10 mmol/l dithiothreitol (DTT) (Sigma Chemical Co, St Louis, MO, USA) and gently vortexed at room temperature. It was then centrifuged at 400g for 10 minutes and the cell pellet was resuspended. Total cell counts were performed with a haemocytometer and slides were made using a cytospin (Cytospin 3; Shandon, Tokyo, Japan) and stained with May-Grunwald-Giemsa stain for differential cell counts. The mean differential cell counts of at least two chest physicians on separate occasions in a blind manner were used.
The supernatant was stored at –70°C for subsequent assay for albumin, VEGF, and eosinophil cationic protein (ECP). The concentration of VEGF was measured using an enzyme linked immunosorbent assay kit (R&D System Inc, Minneapolis, MN, USA), ECP concentration was measured using a radioimmunoassay kit (Pharmacia Diagnostics, Uppsala, Sweden), and albumin was measured by laser nephelometry. We thus could calculate the airway vascular permeability index (ratio of albumin concentrations in induced sputum and serum).
All subjects produced an adequate specimen of sputum of at least 2 ml with differential cell counts of <10% squamous cells.
Exercise challenge testing
Three days after sputum induction the exercise test was performed at approximately 13.00 hours to eliminate the effects of diurnal variation. Exercise challenge testing was performed on an electrically driven treadmill (Q55xt, Series 90; Quinton Instrument Co, Seattle, WA, USA) for 6 minutes with a fixed workload adjusted to increase the cardiac frequency to 90% of the maximum predicted for the age of the patient.8 All subjects breathed unconditioned room air (temperature 22–25°C) and were trained to overcome hyperventilation during testing. A single lead electrocardiogram (ECG) and pulse oximeter (502-US; CSI, Tokyo, Japan) were monitored continuously. The criteria for exclusion were the presence of coronary artery disease or cardiac arrhythmias. A spirometer (Chestac–25F; Chest Co, Tokyo, Japan) was used to obtain spirometric measurements before and after exercise challenge. The higher of two measurements of FEV1 obtained before exercise challenge was taken as the baseline value. Single measurements of FEV1 were obtained 1, 3, 5, 10, 15, 20, 25 and 30 minutes after completion of the exercise challenge. The response to exercise challenge was taken to be the percentage fall in FEV1 after exercise:
% fall in FEV1 = (FEV1 (baseline) – FEV1 (after exercise))/(FEV1 (baseline)) × 100
For 8 weeks after the first exercise test beclomethasone dipropionate (BDP) 400 μg twice daily was administered to the asthmatic patients. During this 8 week period all subjects continued their previous treatment of β2 agonists and theophylline. All of the above tests were repeated following treatment with BDP.
Statistical analysis
All data are expressed as mean (SD) values. The Mann-Whitney U test was used for intergroup comparisons and Wilcoxon’s signed rank test was used to compare paired values. The significance of correlation was evaluated using Spearman’s rank correlation coefficients. A p value of <0.05 was considered significant.
RESULTS
The clinical characteristics of the 23 asthmatic subjects and 11 age matched normal controls are shown in table 1. The percentage of eosinophils and the concentration of ECP in induced sputum were significantly higher in asthmatic subjects than in normal controls. The concentration of VEGF in induced sputum was also significantly higher in patients with asthma than in normal controls. There was a significant correlation between the concentration of VEGF and the % maximal fall in FEV1 (r=0.826, p=0.0001; fig 1) and between the concentration of VEGF and the airway vascular permeability index (r=0.621, p=0.0037; fig 2).
Clinical characteristics of the study subjects

Correlation between VEGF levels in induced sputum and % maximal fall in FEV1 in asthmatic patients.

Correlation between VEGF levels in induced sputum and airway vascular permeability index in asthmatic patients.
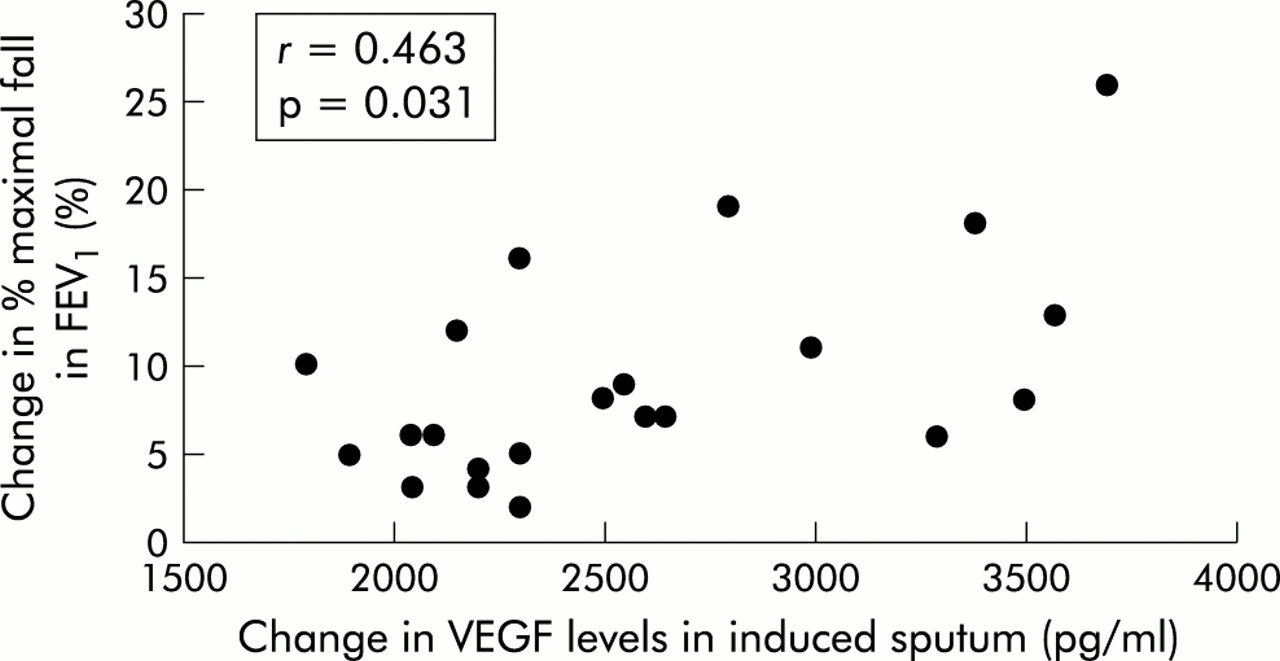
After treatment with inhaled BDP there was a significant decrease in the percentage of eosinophils (from 17.0 (6.9)% before treatment to 0.8 (1.1)% after treatment; p<0.0001), the concentration of ECP (from 705 (288) ng/ml to 117 (100) ng/ml; p<0.0001), and in VEGF (from 7051 (2361) pg/ml to 4498 (2135) pg/ml; p<0.0001) in patients with asthma. The severity of EIB was also significantly decreased after treatment with inhaled BDP (% maximal fall in FEV1 24.0 (13.3)% before treatment v 14.7 (9.4)% after treatment, p<0.0001). The change in the concentration of VEGF was significantly correlated with the change in the % maximal fall in FEV1 (r=0.463, p=0.031; fig 3). In contrast, neither the change in percentage of eosinophils nor in the concentration of ECP was significantly correlated with the change in the % maximal fall in FEV1.

{kind=link}
{kind=link}
{kind=link}
Correlation between change in VEGF levels in induced sputum and change in % maximal fall in FEV1 in asthmatic patients. Each value was calculated as the difference between the values before and after treatment with beclomethasone dipropionate (BDP).
DISCUSSION
Higher levels of VEGF were found in induced sputum from asthmatic patients than from normal controls. Moreover, there was a significant correlation between the concentration of VEGF and the severity of EIB. After treatment with inhaled BDP the concentration of VEGF was significantly decreased, and the change in VEGF levels was correlated with the change in the severity of EIB. These findings suggest a role for increased production of VEGF in asthmatic airways in the pathogenesis of EIB.
Bronchial asthma is a chronic airway inflammatory disease associated with airway wall remodelling which includes the growth and proliferation of new blood vessels. It was recently reported that both the number and percentage of vessels in biopsy specimens taken from asthmatic patients were increased compared with normal controls.9 Moreover, it has been recognised that airway mucosa is oedematous and contains dilated and congested blood vessels even in mild asthma.10 VEGF is known as a vascular permeability factor. It was previously reported that VEGF induced fenestration in endothelial cells in both in vitro11 and in vivo models.12 We have clearly shown that VEGF induces increased vascular permeability in asthmatic airways, which may cause leakage of the mucosal and submucosal capillary beds and induce airway wall thickness. We found that VEGF levels in induced sputum was significantly decreased after treatment with inhaled BDP. This is supported by a previous report which showed that the transcription of VEGF mRNA and the secretion of VEGF protein were downregulated in the presence of corticosteroids.13 Interestingly, although eosinophilic airway inflammation was completely inhibited by inhaled BDP in the patients with asthma, the concentration of VEGF was still higher in the asthmatic subjects than in controls and the asthmatic subjects subsequently exhibited EIB.
The importance of the vasculature in EIB has previously been suggested.14 In asthmatic subjects the bronchial capillary bed is hypertrophied and hyperplastic. Because of its location and its ability to alter its size in the asthmatic state, the bronchial circulation could exert an important influence on airway geometry—vascular engorgement, capillary leakage, and oedema formation could induce airway narrowing. Many of the inflammatory mediators thought to cause constriction of bronchial smooth muscle can also cause dilatation and leakage of the mucosal and submucosal capillary beds and induce thickening of the airway wall. A previous study suggested that small increases in wall thickness induced by airway inflammation could produce striking changes in airway responsiveness to various stimuli such as exercise, even with a very small increase in resting airway muscle tone.15 Thus, mucosal oedema may have a profound effect on airway function and might explain the heightened reactivity characteristic of bronchial asthma. Capillary leakage and airway mucosal oedema formation induced by VEGF may therefore contribute to the airway narrowing after exercise. Yong et al16 recently reported that VEGF levels in sputum are significantly increased even in patients with stable asthma and are higher in an acute asthmatic attack. However, Demoly et al17 found no significant difference in VEGF levels in bronchoalveolar lavage (BAL) fluid in asthmatic subjects and normal controls and reported that VEGF levels in asthmatic airways did not correlate with plasma extravasation. This discrepancy may be explained by the use of different biological samples or different asthma states. The dilution in BAL fluid might have resulted in very low VEGF levels which would make it difficult to detect a significant difference between asthmatic subjects and normal controls. Nitric oxide (NO) is a potent vasodilator in the bronchial circulation and increases airway vascular leakage, leading to airway wall oedema.18 Scollo et al19 reported that NO levels were correlated with the magnitude of bronchoconstriction induced by exercise challenge. In our earlier study we suggested that NO is associated with EIB and contributes to the prolonged airway narrowing phase evoked by exercise.20
In conclusion, our findings suggest that excessive production of VEGF in asthmatic airways contributes to the pathogenesis of EIB via increased airway vascular permeability. It is important to measure the concentration of VEGF in induced sputum when predicting the severity of EIB in patients with asthma. The role of VEGF in modulating EIB warrants serious consideration.
Acknowledgments
This work was supported by grant-in-aid for Scientific Research (1360611) from the Ministry of Education, Science and Culture, Japan.