Article Text

Abstract
Background: The effects on morbidity were examined of providing an educational intervention and a written guided self-management plan to the parents of pre-school children following a recent attendance at hospital for asthma or wheeze.
Methods: A prospective, randomised, partially blinded, controlled trial was designed at two secondary care centres. Over a 13 month period 200 children aged 18 months to 5 years at the time of admission to a children's ward or attendance at an accident and emergency department or children's (emergency) assessment unit (A&E/CAU) with a primary diagnosis of acute severe asthma or wheezing were recruited. 101 children were randomised into the control group and received usual care and 99 were assigned to the intervention group and received: (1) a pre-school asthma booklet; (2) a written guided self-management plan; and (3) two 20 minute structured educational sessions between a specialist respiratory nurse and the parent(s) and child. Subjects were assessed at 3, 6, and 12 months. The main outcomes were GP consultation rates, hospital re-admissions, and attendances at A&E/CAU. Secondary outcomes included disability score, caregivers' quality of life, and parental knowledge of asthma.
Results: There were no statistically significant differences between the two groups during the 12 month follow up period for any of the main or secondary outcome measures.
Conclusions: These results do not support the hypothesis that the introduction of an educational package and a written guided self-management plan to the parents of pre-school children with asthma who had recently attended hospital for troublesome asthma or wheeze reduces morbidity over the subsequent 12 months.
- asthma
- children
- parental education
- self-management plan
Statistics from Altmetric.com
Asthma has been the focus of much recent research into the effectiveness of guided self-management and the provision of education.1–9 The British Thoracic Society (BTS) guidelines recommend that “all patients should be given information about features which indicate when their asthma is worsening and what to do under those circumstances. Giving those with asthma written self-management plans . . . reduces morbidity and health costs”.10
Recent studies into the effects on morbidity of education and self-management for children with asthma have shown positive results. Ronchetti et al11 found that using an established educational intervention significantly reduced the number of emergency treatments required by a group of children, particularly for the children with more severe asthma. Madge et al8 found significantly fewer re-admissions in a group of hospitalised children who received a structured nurse-led discharge package (8.3%) compared with a control group (24.8%). Wesseldine et al9 found similar results, with 15% of the children who received a structured nurse-led discharge package being readmitted to hospital compared with 37% in a group of children who received only standard discharge care. Re-attendance at the A&E department was also lower in the intervention group (8% v 38%), as were GP consultations for problematic asthma (39% v 90%). Both the latter studies represent practicable and easily transferable interventions with parents and children in the intervention group receiving a booklet, a written agreed management plan, and an education session.
The present study was designed to examine the effects of providing a guided self-management plan to the parents of pre-school children with asthma or wheeze in a secondary care setting. It was conducted in two centres and dealt both with inpatients and emergency attenders. The intervention was designed to be practicable. While the main objective was to assess the effect of the intervention on the number of hospital re-admissions and GP consultations, the effects on the quality of life of the child and his/her family and their knowledge of asthma were also investigated.
This study aimed to test the hypothesis that the introduction of an educational package and self-management guide to the parents of pre-school children who have recently attended hospital with a primary diagnosis of troublesome asthma or wheeze will reduce morbidity.
METHODS
The study was a prospective, randomised, partially blinded, controlled trial. It comprised two centres: the Children's Hospital, Leicester Royal Infirmary (LRI) and Booth Hall Children's Hospital, Manchester (BH).
Subject recruitment and randomisation
Children eligible for inclusion in the study were aged 18 months to 5 years inclusive at the time of admission to a children's ward or attendance at either an accident and emergency (A&E) department or the children's (emergency) assessment unit (CAU at LRI) with a primary diagnosis of acute severe asthma or wheezing. 69% of those recruited had been admitted for asthma on at least one previous occasion. Children could only be recruited to the study once. The parents of eligible children were given a written information sheet explaining the study. Informed signed consent was obtained from the parents of all subjects and the study was approved by the Leicestershire research ethics committee.
Children were recruited over a period of 13 months and, following parental consent, were randomly assigned to either an intervention or a control group. Randomisation was achieved by generating numerical codes in random permuted blocks of 10. Codes were held in individual sealed numbered envelopes. Separate lists were generated for each patient group (inpatient and A&E/CAU) and for each study centre (LRI and BH).
Children admitted to hospital as inpatients were recruited on the day of discharge. Not all eligible children admitted as inpatients during the study period were included as recruitment did not take place over weekends or when a specialist respiratory nurse was not available. Children who had attended A&E/CAU but were not admitted were contacted by telephone at home on the first working day after the day of attendance. Thus, all parents of children admitted to A&E/CAU during the study period were asked to participate in the study. Recruitment of children and data collection was carried out at LRI by two researchers (CS and LW) while the intervention was given by two specialist respiratory nurses (MG and LW). At BH children were recruited and data were collected by one researcher (AD) and the intervention was given by one specialist respiratory nurse (JF).
At recruitment parents were asked to complete two questionnaires. The baseline questionnaire assessed the child's previous hospital admissions, pattern and severity of asthma symptoms, atopic disease, known precipitating factors for wheeze, and medication on discharge. A second questionnaire recorded parent's recall of the information they had received about asthma at the time of their child's discharge from hospital, its source, how long it took to impart, whether written or verbal, and how useful they found it. Parents of children admitted to a ward were asked to complete it once they were home, following their child's discharge from hospital. Parents whose children attended A&E/CAU were given the questionnaire at the time of recruitment (before any educational intervention). They were all asked to return it in a freepost envelope. Discharge medication was decided by clinical staff who were unaware of the group to which a child had been assigned.
Intervention
Children assigned to the intervention group received: (1) a general education booklet about asthma in pre-school children (excluding babies); (2) a written guided self-management plan; and (3) two 20 minute structured educational sessions given on a one to one basis by a specialist respiratory nurse with a diploma in asthma care to the parent(s) and child. Children recruited as inpatients received the first session on the ward on the day of discharge and returned to a special outpatient clinic 1 month later for the second session. Children recruited from A&E/CAU received their initial education session in the outpatient clinic within 2 weeks of attendance at A&E/CAU and returned 1 month later for their second visit. Those who failed to attend on any occasion were telephoned to arrange one further appointment.
The first educational session focused in sequence on the topics covered in the booklet and included personalisation of the self-management plan. The second session was aimed to be parent-led, discussing issues raised by the parents with a review of parents' techniques in administering medicines to their child. The 12 page A5 booklet written specifically for use in this study was adapted from the booklet used by Wesseldine et al.9 It covered symptoms, common triggers and how to avoid them, and the treatment of asthma. It emphasised practical steps for parents to manage their child's wheezing and provided spaces in which parents could individualise the information. The booklet was assessed for readability using the SMOG grading formula at grade 7.12 The portable, 10 × 10 cm folded self-management plan provided instructions on when to use reliever medication, what to do if the child's asthma worsened, signs of severe asthma, and appropriate actions to be taken. These actions were, as a first step, to give the child 2–4 puffs of reliever, depending on response, to be repeated every 3–4 hours if necessary and, as a second step, to start prednisolone (if provided) and to go to the GP. A large volume spacer (Volumatic, GSK or Nebuhaler, Astra Zeneca) and metered dose inhaler (with or without facemask, depending on the age of the child) were the standard devices. The plan provided spaces for the specialist respiratory nurse to enter the child's current asthma medications. The draft booklet and self-management plan were reviewed by two specialist respiratory nurses (LW and JF) and two consultant paediatricians (MS and JC). The cost of providing the written information amounted to £22.71 per subject while the education sessions cost £27.46 per subject.
Children assigned to the control group received usual care (a range of medical and nursing approaches used at present, according to the skills of the health professionals).
Outcomes
Outcomes were measured at 3, 6, and 12 months following recruitment. The main outcomes were GP consultation rates, hospital re-admissions, and attendances at A&E or CAU. These were collected from the child's GP records and from hospital notes and records.
Secondary outcome measures included the child's asthma symptoms and consequent level of disability as perceived by the parents, assessed using Usherwood's13 index of perceived symptoms in asthmatic children (IPSAC) measure with minor adaptations. On this measure a higher score represented greater perceived disability or extent of symptoms. The qualtiy of life of the parents or caregivers was assessed using Juniper's14 paediatric asthma caregiver's quality of life questionnaire (PACQLQ) with minor adaptations. Lower scores represent more severe impairment.
Symptom diaries completed over the 4 weeks before each follow up visit were used to measure morbidity and the appropriateness of the parents' or caregivers' responses to changes in the child's asthma. The diaries were scrutinised blind—that is, by a member of the team who had not been involved in the educational intervention. Episodes were identified as two or more days of worsening asthma symptoms as determined from each child's baseline asthma symptoms. The parents' responses were classified as appropriate if they changed their child's treatment in accordance with the self-management plan.
Two further measures were developed for use in this study. In a 42 item caregivers' knowledge of asthma questionnaire administered at the first follow up visit respondents were required to indicate whether a statement about asthma was true or false. All the questions were based on topics covered in the educational sessions and booklet. Scores could range from 0 to 42. An attempt was also made to measure the perceived confidence of the parents or caregivers in caring for their child. Parents were asked to respond to 14 statements using a 4 point scale on which total scores could range from 0 to 56.
Pilot tests of all the measures used in the study were undertaken with up to 10 respondents. No major problems were found with any of the measures.
Data management and statistical analysis
A sample size of 200 (100 per group) has 80% power to detect differences of 0.4 SD between two groups at a 5% significance level and differences of 20% in categorical data.
The SPSS statistical package was used to analyse the data. Between group differences were examined using a t test, χ2 test, or the Mann-Whitney U test as appropriate. Although it was not the primary aim, some subgroup analysis was performed comparing children recruited from A&E/CAU with those recruited as inpatients, and a comparison of patients at LRI with those at BH. The results were analysed on an intention to treat basis.
RESULTS
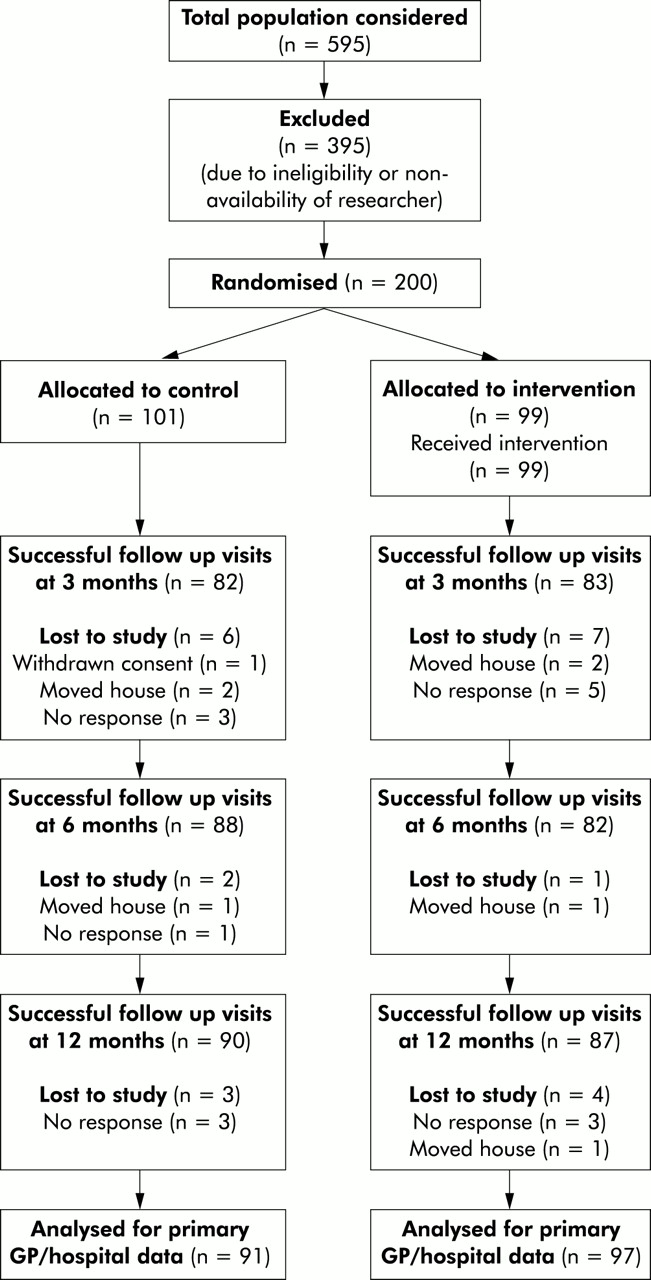
From February 1998 to March 1999, 200 children were recruited to the study of which 177 were successfully followed for 12 months, 87 in the intervention group and 90 in the control group. Figure 1 shows a trial profile of the children eligible for the study. The main reasons for drop out from the study were either a lack of response to letters, telephone or personal calls or that the family had moved house. GP and hospital data were collected for 91 children in the control group and 97 in the intervention group.

{kind=link}
Trial profile showing the drop outs at each assessment stage. Families who were assessed 12 months after recruitment but were unavailable for earlier assessments were not classed as drop outs.
The two groups were comparable at baseline (table 1). The age of the children ranged from 14 to 61 months and the population reflected the ethnicity of the communities served by the two study centres. Both groups cited colds as the main trigger for coughing or wheezing episodes. For 56% of the children colds were the only trigger for wheeze. Approximately half of the children in each group also suffered from eczema. While 69% of the children had been given a diagnosis of asthma, many were classed as having mild asthma with 42% on step 1 of the BTS guidelines10 and 45% on step 2 of the guidelines. Attendance at the first and second education sessions was 100% and 73%, respectively, for the inpatients and 93% and 68% for the A&E/CAU subjects.
Demographic and clinical characteristics of study children at baseline
The information recalled by parents shortly after discharge from hospital was most reliably evaluated in those families whose child was an inpatient, as it is known who had received the information package prior to completion of the questionnaire. For those discharged as inpatients and allocated to the control group, 49% of parents (26/53) recalled receiving verbal information compared with 94% (46/49) in the intervention group. In practice, all those in the intervention group were given verbal information. Parents recalled that imparting this information took 5 minutes or less for 73% (19/26) of the control group, while for 85% (39/46) of the intervention group it took 10 minutes or more. In practice, a mean of 23 minutes was taken for the first education session and 20 minutes for the second session. Only 15% (8/53) in the control group reported receiving written information, but all found it at least of some use. The most frequently discussed topics were symptoms of asthma and what to do when the child's asthma gets worse. Of the control families recruited as A&E/CAU attenders, 23% (10/43) recalled being given verbal information and 5% (2/43) written information.
Main outcomes
There were no statistically significant differences between the two groups during the 12 month follow up period for any of the main outcome measures: number of GP consultations, inpatient admissions, attendance at A&E, or prescriptions recorded (table 2). Subgroup analysis showed no statistically significant differences between the control and intervention groups for recruitment centre (LRI v BH), place of recruitment (inpatient ward v A&E/CAU), or for those who had had previous admissions or no previous admissions.
Health care resource utilisation in the 12 month study period (collected from GP and hospital records)
Secondary outcomes
There was no significant difference between the two groups on Usherwood's13 IPSAC measure at 3, 6, or 12 months after recruitment (table 3). Differences between daytime symptom scores at the final assessment were approaching significance. Scores in both groups were higher at baseline than at subsequent assessments, reflecting the fact that the child had recently attended hospital. Following the initial assessment scores tended to be low, reflecting low levels of disability and symptoms.
Quality of life scores
Parental or caregivers' quality of life scores14 showed no statistically significant differences between the two groups at 3, 6, or 12 months (table 3). However, the difference between the scores approached significance in the activity domain at 12 months with the control group (mean 5.77) scoring higher (better outcome) than the intervention group (mean 5.33, mean difference –0.44, 95% CI −0.89 to 0.02, p=0.06), whereas at baseline the intervention group scored higher, reflecting less restriction on activity. Following the trend of the IPSAC13 scores, the PACQLQ14 scores in both groups were lower at baseline than at subsequent assessments, indicating greater impairment at the time of recruitment.
The parents' or caregivers' knowledge of asthma scores showed no statistically significant difference between the two groups (median scores 35.0 for the intervention group (n=81) v 33.0 for the control group (n=83), median difference −1.0, 95% CI −2.0 to 1.0, K=2695).
No significant differences were found between groups in scores assessing the confidence of the parents or caregivers in caring for their child (median score 46.5 at the final assessment for the intervention group v 45.0 for the control group, median difference 0, 95% CI −2.0 to 1.0, K=3208).
The data from the symptom diaries showed no statistically significant differences between the two groups in terms of number, length or severity of episodes, or the appropriateness of treatment response at any assessment stage.
DISCUSSION
The aim of this study was to test the hypothesis that the introduction of an educational package and a written guided self-management plan to the parents of pre-school children who had recently attended hospital for troublesome asthma or wheeze would reduce morbidity over the subsequent 12 months. The results do not support the hypothesis. For all the main and secondary outcome measures there were no statistically significant differences between the two groups at any time point.
Possible explanations for the results of this study include issues related to the clinical trial methodology, the effectiveness of the educational techniques employed, and the appropriateness of the advice given which, although based on published guidelines,10 is essentially derived from an adult model of asthma.
Firstly, were there technical inadequacies in the design of the study and in the way it was conducted? The study was designed and conducted as a randomised controlled trial and strictly adhered to randomisation with the use of sealed numbered envelopes. The study was not blind but neither general practitioners nor hospital doctors were aware of the group to which a child had been assigned. Recruitment to the study continued for 13 months, avoiding seasonal selection. The trial involved two centres which should reduce locality effects or selection bias. Dilution of the effects of the intervention is a possibility as many of the control group recall being given verbal information although not in as great depth as that given to the intervention group.
The treatment received by the study subjects on discharge from hospital was determined by the responsible clinicians rather than the trialists, so the subjects did not receive standardised treatment. This may have been a disadvantage in the design of the study. To have prescribed prednisolone in the self-management plan as a treatment for acute episodes of wheezing may have been helpful. However, there is no evidence to support the use of oral steroids for viral episodes of wheeze in the youngest age groups.
The validity of the questionnaires used to assess the parents' confidence in caring for their child with asthma or wheeze and the parents' or caregivers' knowledge about asthma can be questioned as the measurement tools had not been developed using a rigorous validation process. Furthermore, knowledge gained by parents before recruitment (table 1), during admission, or following discharge will have reduced the power of the questionnaire to identify knowledge gained as a result of the intervention. The frequency and intensity of assessments may have influenced the behaviour of all the subjects in the study, thus reducing the power of the intervention. However, no statistically significant difference was found between the two groups for the main outcome measures at the first assessment stage. In the main, there seem to be no grounds to question the validity of the main outcome measures of GP consultation rates, hospital re-admissions, and attendances at A&E/CAU, none of which showed any significant effect of the intervention.
Another explanation for the findings of this study is that the intervention was inadequately designed. The booklet and education sessions were modelled on those used successfully by Wesseldine9 and on published principles for providing asthma education.15–17 Previous studies8,9 using similar methods have shown education to be very effective in reducing hospital admissions. The asthma booklet was assessed for readability using the SMOG12 grading formula and should have been appropriate to parents with a reading age of 12 years. This compares favourably with the National Asthma Campaign booklet “Asthma in the under fives”18 booklet which was found on average to require a SMOG reading grade of 9, representing a reading age of 14.
This study differed from the successful studies of Madge et al8 and Wesseldine et al9 in two major ways. Firstly, the previously successful interventions were carried out by a single highly motivated individual at one site while, in the present study, the intervention was carried out by three specialist nurses at two sites. However, since there was close cooperation in the development of the programme and since one of the three specialist nurses (LW) had already implemented a previously successful intervention, it is difficult to believe that this is the explanation for the lack of effect in the present study. The second major difference between this and previous studies may therefore hold the explanation for the present findings—namely, that the previous studies recruited children aged 2–16 years of age while the present study recruited children of pre-school age.
Further analysis of the data from the study by Wesseldine et al9 shows that the effects of the intervention were weakest in the children aged 5 years and younger. In that study, while GP and A&E attendances were significantly fewer in the intervention group over the 6 month follow up period in the children aged 2–5 years, the difference in hospital readmissions between the intervention and control groups was not statistically significant. In the study by Madge et al8 which also showed a significant intervention effect, almost 60% of those recruited were aged 6 years and older.
Why should advice suitable for older children not be effective in pre-school children? Young children are particularly likely to suffer from episodic viral asthma. In the present study this was the case for 56% of those recruited. Although 96% of those recruited had experienced at least one episode of wheezing during the previous 12 months, for almost 46% of these children the admission when they were recruited to the study was their first hospital admission and 87% were on steps 1 or 2 of the BTS guidelines10 (although this grading may not be an appropriate measure of severity for episodic pre-school wheeze). Symptom diary data suggest that these children had few interval symptoms despite suffering from episodes severe enough to warrant secondary care. Thus, the advice given during the educational intervention may have been inappropriate and it may be that the standard medical advice based on the BTS guidelines10 given to the parents of pre-school children with asthma is not sufficiently evidence based. There is evidence to question the efficacy of current treatment in young children, especially those in the youngest age groups.19,20
Despite the evidence for the efficacy of guided self-management in older children, this study did not find that the introduction of a standard educational package and a written guided self-management plan to the parents of pre-school children with asthma who have recently attended hospital for troublesome asthma reduced morbidity. These findings suggest that further work is required to establish the efficacy and appropriateness of the treatment guidelines suggested for pre-school children with asthma or wheeze. Classification of pre-school wheezy children by pattern of disease (persistent or episodic) or aetiology (atopic or non-atopic) may be a starting point for clinical trials aimed at expanding the therapeutic evidence base. Further work should seek to clarify the most appropriate advice for the parents of pre-school children with asthma or wheeze, the most appropriate method for providing this, and the most appropriate methods of assessing the effects of such an intervention.
Acknowledgments
The authors thank Melanie Gillespie (MG) and Jane Farrell (JF), specialist respiratory nurses for giving the educational sessions and running the outpatient sessions. They are indebted to all those families who participated in this study.
REFERENCES
Footnotes
-
This study was funded by the NHS Executive Mother and Child Health Programme (MCH 16-15). Dr Martyn Partridge helped to prepare the initial research proposal under the auspices of the UK National Asthma Campaign.