Article Text

Abstract
Background: Traditionally, patients with acute respiratory failure due to chronic obstructive pulmonary disease (COPD) admitted to the intensive care unit (ICU) are believed to have a poor outcome. A study was undertaken to explore both hospital and long term outcome in this group and to identify clinical predictors.
Methods: A retrospective review was carried out of consecutive admissions to a tertiary referral ICU over a 6 year period. This group was then followed prospectively for a minimum of 3 years following ICU admission.
Results: A total of 74 patients were admitted to the ICU with acute respiratory failure due to COPD during the study period. Mean forced expiratory volume in 1 second (FEV1) was 0.74 (0.34) l. Eighty five per cent of the group underwent invasive mechanical ventilation for a median of 2 days (range 1–17). The median duration of stay in the ICU was 3 days (range 2–17). Survival to hospital discharge was 79.7%. Admission arterial carbon dioxide tension (Paco2) and APACHE II score were independent predictors of hospital mortality on multiple regression analysis. Mortality at 6 months, 1, 2, and 3 years was 40.5%, 48.6%, 58.1%, and 63.5%, respectively. There were no independent predictors of mortality in the long term.
Conclusions: Despite the need for invasive mechanical ventilation in most of the study group, good early survival was observed. Mortality in the long term was significant but acceptable, given the degree of chronic respiratory impairment of the group.
- chronic obstructive pulmonary disease
- acute respiratory failure
- intensive care
Statistics from Altmetric.com
Patients with chronic obstructive pulmonary disease (COPD) requiring admission to the intensive care unit (ICU) usually have severe pre-existing limitation of function. It is commonly believed that these patients have a poor outcome and consume a large amount of intensive care resources, particularly if they need endotracheal intubation. Interpretation of the few existing outcome studies has several problems. Decisions with regard to ICU admission or ventilation of patients with COPD may not only vary between units, but also between physicians.1 Some studies include patients for whom the reason for acute deterioration was not primarily an exacerbation of COPD but pneumonia, pulmonary oedema, or pulmonary embolism.2 There is also a lack of data on long term survival after hospital discharge in this group of patients. We aimed to provide comprehensive data on the prognosis of these patients by documenting in-hospital and long term survival of patients admitted to a tertiary referral ICU over a 6 year period. We also sought predictors of both hospital and long term outcome that might assist the clinician to make difficult decisions about whether or not intensive care management should be offered to these chronically impaired patients.
METHODS
Patient selection
The clinical notes of all patients admitted to the ICU with a diagnosis of respiratory failure or respiratory arrest during the period from 1 January 1989 to 31 December 1994 were reviewed. Only those with a primary admission diagnosis of acute respiratory failure secondary to COPD were included. COPD was identified by the characteristic findings on history and examination with or without typical radiographic or pulmonary function test abnormalities.3 Patients admitted to the ICU with COPD but in whom this was not the primary reason for admission (such as those with COPD admitted after surgery or trauma) were excluded as were patients in whom the primary cause of respiratory failure was pneumonia, pulmonary oedema, pulmonary embolism, or pneumothorax.
The intensive care specialist on duty managed patients admitted to the ICU with COPD during the study period. All patients received regular nebulised β agonists, nebulised anticholinergic therapy, and intravenous steroid treatment. Additional nebulised or intravenous β agonists were given to patients with resistant wheeze; antibiotics were administered at the discretion of the intensive care specialist. Controlled oxygen therapy was administered to spontaneously breathing patients. The decision to intubate was made by the physician caring for the patient and was made on the basis of either respiratory arrest, deteriorating level of consciousness, or exhaustion despite maximal medical treatment. Weaning from mechanical ventilation began as soon as the patient was capable of initiating a spontaneous breath; in practice, this meant that patients were changed from synchronised intermittent mandatory ventilation (SIMV) to pressure support ventilation (PSV) as soon as possible and were then weaned by progressive reduction in PSV as tolerated.
Data collection
The following data were collected retrospectively by reviewing patient charts.
Hospital admission
Age, sex, number of previous hospital admissions with an acute exacerbation of COPD, and number of episodes of prior mechanical ventilation were recorded.
Baseline data: baseline spirometry was defined as the best recorded forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) during a stable outpatient visit or immediately preceding hospital discharge. The level of usual dyspnoea and activity was graded on a 4 point scale, a modified version of that used by Menzies,4 as follows:
Grade 1: independent, capable of work or living without any assistance.
Grade 2: restricted, able to leave the house but severely limited in exercise ability.
Grade 3: house bound, leaves the house rarely but able to perform self-care.
Grade 4: bed or chair bound, unable to perform self-care.
Pre-admission treatment such as the use of oral steroids, home oxygen, and home ventilation was also documented.
ICU admission
Initial white cell count and haemoglobin concentration was recorded. Arterial blood gas measurements were documented directly before institution of mechanical ventilation or for spontaneously breathing patients on admission to the ICU. The level of consciousness was also graded on a scale of 1–4 as follows:
-
Grade 1: alert
-
Grade 2: drowsy but responds to verbal stimulus
-
Grade 3: responsive to painful stimulus only
-
Grade 4: comatose/respiratory arrest.
The APACHE II score5 was collected prospectively by means of the binational intensive care database known as the Australia and New Zealand Intensive Care Society (ANZICS) database.
ICU course
The need for and timing of intubation and duration of mechanical ventilation were recorded.
Outcome and follow up
The duration of intensive care stay and hospital stay were recorded. Long term follow up on those who survived the hospital admission was achieved by checking patients studied against the New South Wales death register on 16 March 1998 for all patients who had a New South Wales address. For the maximum possible matches the following combinations were used: patient surname soundex and postcode, patient surname soundex and date of birth, and postcode and date of birth. The resulting matches were then confirmed by visual inspection. Patients who had given an interstate address on admission were contacted from the outset by telephone. The remainder were traced by telephone contact either directly or via next of kin or local medical officer.
The Central Sydney Area Health Service ethics review committee granted permission for the review of clinical notes and checking the death register.
Statistical analysis
Analysis was performed using SPSS PC+ for Windows Version 7.0 or LogXact. Descriptive data are given as mean (SD) or as median (range). Independent predictors of hospital survival and the need for intubation were identified using logistic regression analysis. The long term survival of those discharged from hospital was analysed using Cox's proportional hazards models. Kaplan-Meier curves were used to demonstrate survival distribution.
RESULTS
During the years 1989–94 there were 82 admissions to the ICU (74 patients) identified with a primary admission diagnosis of COPD. Eight patients had one readmission each during the study period. Where a patient presented to the ICU on more than one occasion with acute respiratory failure due to COPD, only data from the first admission were used. Demographic and ICU data are shown in table 1. Before intensive care admission, 40.5% of the patients were housebound (functional level grade 3 or 4) and 14.9% were receiving home oxygen. The mean APACHE II score was 22, median ICU stay was 3 days and hospital stay 12 days.
Baseline and ICU data for the 74 study patients. Predictors for intubation and hospital mortality on multivariate logistic regression analysis are also shown
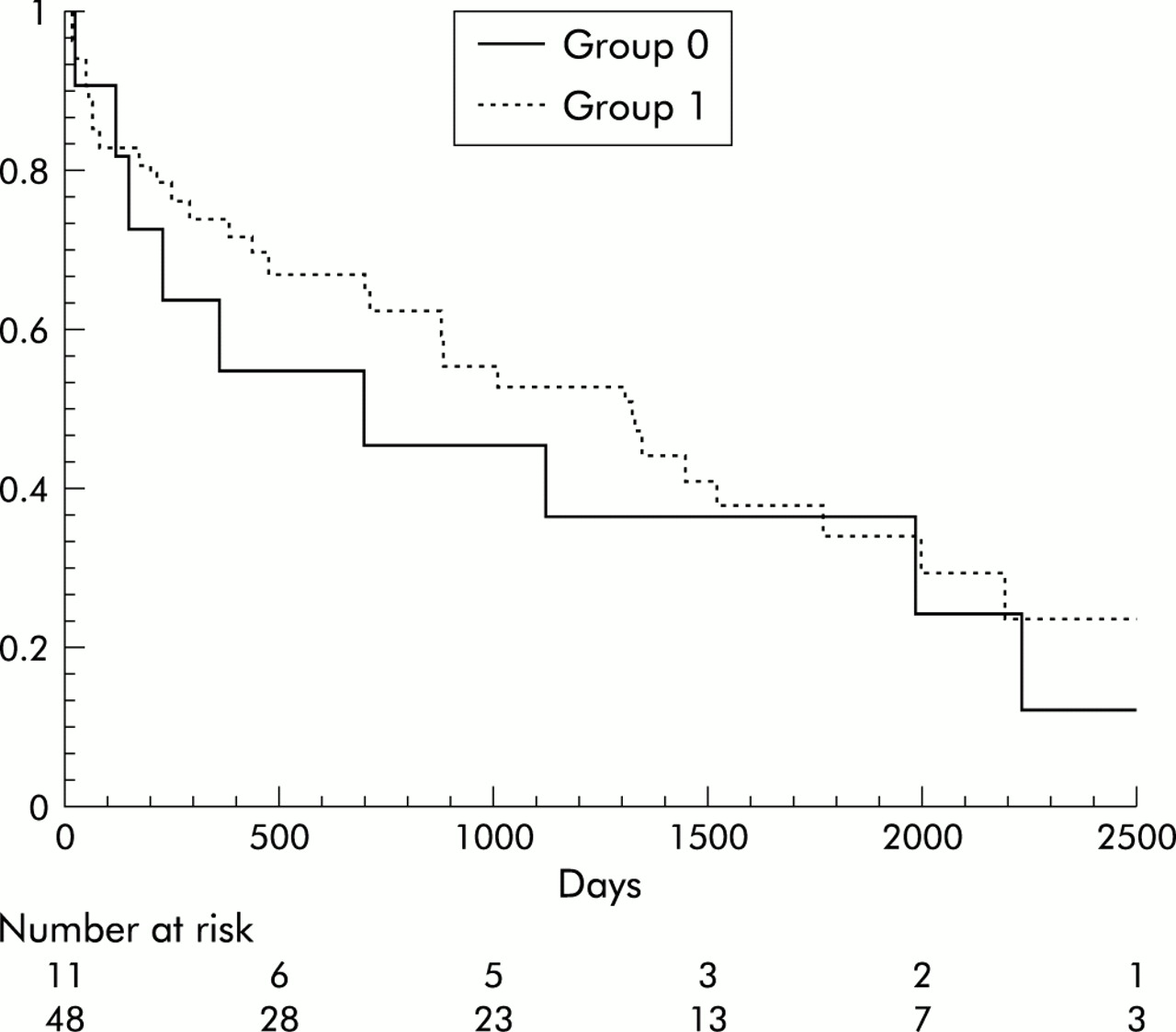
Sixty three patients (85.1%) received mechanical ventilation via an endotracheal tube for a median of 2 days. As expected, this group had a significantly longer stay in the ICU than patients who were not intubated (table 2). Two patients received mask continuous positive airway pressure (CPAP) but no patient received non-invasive positive pressure ventilation (NIPPV). Of the factors available at the time of ICU admission, only FEV1 was found to be an independent predictor of the need for mechanical ventilation on multivariate analysis (odds ratio 0.14, p=0.05, confidence interval=1.0). Age, sex, APACHE II score, previous intubation, previous hospital admission, steroid use, functional level, FVC, Paco2, Pao2, pH, Fio2, white cell count, and haemoglobin concentration were not predictive. A Kaplan-Meier curve of survival following discharge according to intubation status is shown in fig 1.
Intensive care data and length of stay of intubated and non-intubated COPD admissions during the study period

Survival curve for survival following discharge from hospital by intubation status (group 0 = non-intubated; group 1 = intubated).
Ten patients died in the ICU and five later after discharge to the ward. Mortality at hospital discharge was therefore 20.3%. Age, sex, FEV1, FVC, Pao2, pH, Fio2, the need for mechanical ventilation, previous intubation, previous hospital admission, presence of arrest/coma, steroid use, functional level, white cell count, and haemoglobin concentration were not predictive of hospital mortality. Although invasive ventilation had some effect as a univariate predictor, this was not seen in multivariate analysis. However, Paco2 and APACHE II score were significant independent predictors of hospital mortality (odds ratio 0.96, p=0.05, confidence interval=1.0; odds ratio 1.2, p=0.01, confidence interval=1.3, respectively).
Checking of the remaining 59 patient names against the New South Wales death register produced 43 matches. Only one person had an interstate address and telephone contact with the next of kin yielded the date of death in this case. Two patients were lost to follow up. Of the remaining 13, one person had died shortly after the date of crosschecking against the death register and the other 12 were traceable by telephone.
The mortality rate at 6 months was 40.5%, 48.6% at 1 year, 58.1% at 2 years, and 63.5% at 3 years. A survival curve is presented in fig 2. None of the variables collected were predictors for long term survival.

{kind=link}
{kind=link}
Survival curve for the 74 patients admitted to the ICU with acute respiratory failure due to COPD.
DISCUSSION
The findings of this retrospective review show that good early survival can be obtained when patients with COPD are admitted to the ICU, even where there is significant acute physiological derangement.
Eighty five percent of the study population underwent endotracheal intubation and mechanical ventilation. This is a higher proportion than in other series of patients with COPD in the ICU.6–8 We believe there are two reasons for this and the low rate of less invasive support: (1) the early part of the study predated the common use of NIPPV in COPD and (2) later in the study period NIPPV was administered in a specialised respiratory ward outside the ICU and this potentially biased our study population to a group who would not be suitable for or who had failed on this treatment. Indeed, the mean APACHE II score was higher than that published in a similar review by Moran et al6 (22 (7) v 18 (5)) with a corresponding higher hospital mortality (20% v 11%). The high Pao2 and Paco2 for the group may suggest that some patients required ventilation as a result of uncontrolled oxygen therapy (mean Fio2 for the whole group 0.37 (0.14)). It must also be noted that arterial blood gas measurements were those taken directly on admission to ICU and in some cases following the decision to intubate, in which case correction of hypoxaemia would be a higher priority than avoidance of hypercapnoea. Although values for Pao2 and Paco2 were higher in those who received mechanical ventilation, the difference between the two groups was not significant. In addition, the only independent predictor for the requirement for mechanical ventilation was premorbid FEV1. Pao2, Paco2, pH, Fio2, and APACHE II scores were not predictive. This apparent paradox may suggest that, in patients with acute respiratory failure and COPD, the need for ventilation relates more to the underlying respiratory reserve than the magnitude of measurable physiological disturbance on presentation to the ICU.
Despite the high rate of invasive ventilation, the mortality rate in our study is similar to that reported by Seneff et al7 in a recent series of 362 COPD admissions to an ICU (mortality rate 24%, ventilation rate 47% on day 1). In a review by Weiss and Hudson2 of 11 studies, the combined mortality rate was 20.3% and ventilation rates were 9.8–67.6%; however, the authors stress the heterogeneity of patients in the different studies. Series which include all patients requiring hospital admission with acute respiratory failure due to COPD have reported a hospital mortality of 6–42%.9–13
In the present study intubated patients had a longer stay in the ICU but there was no difference in the duration of hospital stay (table 2). Furthermore, as in other reports,6,7 our analysis showed that the use of invasive ventilation was not an independent predictor of either short term or long term mortality; however, this may have been influenced by the small number in the non-intubated group.
It is commonly believed that patients with COPD require prolonged ventilation once intubated. In a recent series of 41 ventilated patients with COPD in the ICU the median duration of ventilation was 6 days.14 Similarly, studies comparing NIPPV with standard treatment report a mean duration of intubation and ventilation of 1 week or more in the invasive group.15–17 In contrast, in our study the mean duration of ventilation was 3.2 days (median 2 days) with only 13% requiring ventilation for longer than 1 week. Thus, we believe the need for intubation and ventilation in patients with acute respiratory failure due to COPD is not necessarily associated with failure to wean from mechanical ventilation and does not presuppose that outcome will be poor.
Premorbid information thought to be of prognostic value such as age, baseline spirometry, and level of functional activity were not predictive of short term mortality in our series. In particular, pH was not predictive in our series, despite the findings of others.18 In contrast, Paco2 has not been shown to be helpful in predicting short term mortality in patients with acute respiratory failure in previous studies,4,19–21 but in our analysis Paco2 and APACHE II score were independent predictors. As stated by Seneff et al, the effect of physiological scoring systems in predicting mortality in this group of patients has not been widely studied. In their large series they demonstrated the influence of APACHE III score on both prediction of hospital and death rate following discharge from hospital. In the case of hospital mortality, when the relative contribution of the components of the APACHE III score was explored, it was found that the non-respiratory variables of the acute physiology score had a greater explanatory power than the respiratory variables.7 It is possible that the effect of other organ dysfunction may explain why in our study the APACHE II score appears to have an effect independent of Paco2.
There is little recent information on the long term outcome of patients with COPD after an ICU stay. Mortality following ICU admission has been reported to be between 25% and 47%6,7 at 6 months and between 59% and 66% at 1 year.4,7,14
The degree of reduction of baseline FEV1 in patients with COPD admitted to the ICU during the study period is comparable the that reported elsewhere.6,22 Although baseline spirometry was not found to be a determinant of long term mortality after an episode of respiratory failure in this study, it has been shown to be useful in defining the natural history of COPD in the general population.23,24 Our 3 year mortality data are similar to those reported in patients with COPD with equivalent baseline spirometry (FEV1 <0.75 l).25–27 Our long term outcome is also comparable to a large study which examined the effect of domiciliary oxygen therapy on 270 severely hypoxaemic COPD patients.28 This suggests that admission to an ICU (with or without mechanical ventilation) has little effect on the long term outcome in patients who survive the initial episode of acute respiratory failure due to COPD.
Our study has a number of limitations—not least that, in retrospectively reviewing a cohort of intensive care patients, we have excluded those who did not have aggressive management because they refused or were deemed inappropriate. Notwithstanding these restrictions, we had a follow up rate of the initial group of more than 97% and we believe that our findings provide useful information on the outcome of management of COPD in the ICU.
We conclude that patients with COPD requiring intensive care admission have a realistic chance of surviving to hospital discharge, but in the longer term the mortality rate is high with nearly two thirds having died at 3 years. However, this outcome is similar to the background mortality of patients with equivalent severe underlying respiratory disease. Although physiological derangement at presentation may help to predict hospital outcome, no predictors of survival in the longer term were identified. In particular, the need for mechanical ventilation did not distinguish long term survivors from non-survivors.