Article Text

Statistics from Altmetric.com
Introductory article
Immediate and long term effects of weight reduction in obese people with asthma: randomised controlled study
B Stenius-Aarniala, T Poussa, J Kvarnstrom, E L Gronlund, M Ylikahri, P Mustajoki
Objective: To investigate the influence of weight reduction on obese patients with asthma. Design: Open study, two randomised parallel groups. Setting: Private outpatients centre, Helsinki, Finland. Participants: Two groups of 19 obese patients with asthma (body mass index (kg/m2) 30 to 42) recruited through newspaper advertisements. Intervention: Supervised weight reduction programme including 8 week very low energy diet. Main outcome measures: Body weight, morning peak expiratory flow (PEF), forced vital capacity (FVC), forced expiratory volume in one second (FEV1); and also asthma symptoms, number of acute episodes, courses of oral steroids, health status (quality of life). Results: At the end of the weight reducing programme, the participants in the treatment group had lost a mean of 14.5% of their pretreatment weight, the controls 0.3%. The corresponding figures after one year were 11.3% and a weight gain of 2.2%. After the 8 week dieting period the difference in changes in percentage of predicted FEV1from baseline in the treatment and control groups was 7.2% (95% confidence interval 1.9% to 12.5%, P=0. 009). The corresponding difference in the changes in FVC was 8.6% (4. 8% to 12.5%, P<0.0001). After one year the differences in the changes in the two groups were still significant: 7.6% for FEV1 (1. 5% to 13.8%, P=0.02) and 7.6% for FVC (3.5% to 11.8%, P=0.001). By the end of the weight reduction programme, reduction in dyspnoea was 13 mm (on a visual analogue scale 0 mm to 100 mm) in the treatment group and 1 mm in the control group (P=0.02). The reduction of rescue medication was 1.2 and 0.1 doses respectively (P=0.03). After one year the differences in the changes between the two groups were –12 for symptom scores (range –1 to –22, P=0.04) and –10 for total scores (–18 to –1, P=0.02). The median number of exacerbations in the treatment group was 1 (0–4) and in the controls 4 (0–7), P=0.001. Conclusion: Weight reduction in obese patients with asthma improves lung function, symptoms, morbidity, and health status. (BMJ 2000;320:827–832)
Background
Obesity and asthma are both chronic conditions affecting millions worldwide. Over the last 20 years there has been a rapid increase in the prevalence of both of these conditions. Traditionally, adult overweight has been defined as a body mass index (BMI) of 25–29.9 kg/m2. Adult obesity is represented by a BMI of ⩾30.0 kg/m2. In the USA between 1960 and 1994 the prevalence of overweight has increased from 30.5% to 32% and obesity has increased from 12.8% to 22.5%.1 The rise in obesity has been especially notable in women where the prevalence has increased from 15.1% to 24.9%.1 Most of these changes in prevalence occurred between 1976 and 1994. In 1995 the total cost of obesity in the USA amounted to $99.2 billion, of which $51.6 billion were direct medical costs associated with diseases attributable to obesity.2 Globally, obesity has also increased, with an estimated 300 million obese adults worldwide in the year 2000 compared with 200 million in 1995.3 Although traditionally thought of as a problem of westernised countries, an estimated 115 million obese adults reside in developing countries.3
The prevalence of adult asthma is also increasing in the USA. Between 1980 and 1994 the prevalence of self-reported asthma increased from 30.7 to 53.8 per 1000.4 There has also been a disparate increase in the prevalence of asthma in women, with an increase of 80% in women between 1982 and 1992 but by only 29% in men. The attributable cost related to asthma in the USA was estimated at $6.1 billion in 1990.5 Although lack of a standardised definition of asthma precludes precise prevalence trends in older adults, the worldwide prevalence of asthma also continues to rise in children and young adults.6 ,7
Given the parallel increases in obesity and asthma, it is not surprising that the prevalence and incidence of asthma and its related symptoms and phenotypes have been increasingly associated with BMI and obesity. The cross sectional diagnosis of asthma has been associated with obesity in both children8-10 and adults.11-16 Several of these studies noted the relationship only in women12 ,13 ,15 or men.16 Similarly, increasing BMI has been associated with asthma symptoms,9 ,14 ,15 ,17-19 airways hyperresponsiveness,20-22 and atopy.22 ,23
The incidence of asthma has also been related to pre-existing obesity. In a prospective study of 85 911 women in the Nurses' Health Study, 1596 incident cases of doctor diagnosed asthma were identified. Using a multivariate analysis, the relative risk of asthma was 2.7 (95% CI 2.3 to 3.1) for women with a BMI of ⩾30 kg/m2compared with those in the reference group (BMI 20.0–22.4 kg/m2).24 Furthermore, increasing weight gain in these women led to a higher risk of asthma. Women who had gained 10–20 kg since the age of 18 had a relative risk of 1.4 (95% CI 1.2 to 1.7) of developing asthma compared with women whose weight remained stable, while those who had gained more than 25 kg since the age of 18 had a much higher relative risk of developing asthma of 2.7 (95% CI 2.2 to 3.4).24 A recent abstract focusing on the Growing Up Today cohort of children noted 140 cases of incident asthma in boys over a 1 year period and 160 cases of incident asthma in girls. Comparing the highest to the lowest quintile of BMI, the relative risk of asthma during that time was 2.3 (95% CI 1.3 to 4.1) in boys and 1.5 (95% CI 0.9 to 2.6) in girls.25
Introductory article
The study by Stenius-Aarniala and colleagues26 is the first of its kind to evaluate the effects of medical weight loss on a variety of asthma outcome measures. Using a non-blinded, randomised clinical trial, obese subjects with asthma from Helsinki, Finland were assigned to either an intensive dietary programme or to a control group. Asthma was carefully defined during a run in period by the presence of either diurnal peak flow variability or by a bronchodilator response of at least 15%. The mean change from baseline forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) was significantly greater at all time periods up to 1 year following the 8 weeks of dieting in the treatment group compared with the controls. While such a consistent relationship was not found for symptoms, at various times during follow up the treatment group did demonstrate less dyspnoea, use of rescue medications, and overall symptom, impact, activity, and total health status scores. At the end of the 1 year follow up period the treatment group continued to have fewer symptoms and better total health status scores than the controls.
The strength of the study lies in the success of the weight loss programme overall (mean weight loss of 14.2 kg after the dieting period and 11.1 kg after 1 year) and in the consistency of this relationship to the follow up levels of pulmonary function and symptoms in a randomised clinical trial. Ascertainment and follow up were 100% and data were analysed by intention to treat, minimising biases due to non-compliance. There are a few limitations to this study. After extensive exclusion criteria, the remaining sample size was small and randomisation resulted in differences in pulmonary function and sex at baseline. While sex was addressed by evaluating the spirometric outcomes from the change in the percentage predicted, no attempt was made to adjust for baseline level of pulmonary function. Given non-blinding, bias could have played a role with respect to recall during the questionnaires and during administration of spirometric tests. Finally, it would have been beneficial to have evaluated pulmonary function as it pertains specifically to asthmatic subjects. Even without testing for airways hyperresponsiveness, peak flow variability and bronchodilator responsiveness, which were established at baseline, could have been evaluated as primary outcomes. The changes seen in this study were a parallel decrease in FEV1 and FVC, which might be seen in any study of weight loss in obese individuals and may not be specific for obese asthmatic patients. Nevertheless, by noting weight dependent changes in pulmonary function, symptoms, and quality of life that persist over time, the authors have added insights to the pathophysiological relationship between obesity and asthma.
Other evidence for a temporal relationship between weight loss and asthma
Several other studies have evaluated the relationship between weight loss and asthma. Two studies27 ,28 which focused on asthma medication usage before and after gastric bypass surgery reported a decrease in postoperative medication usage of 50% and 100%, respectively. Dixon et al 29 evaluated symptom scores from 32 obese asthmatic subjects before and after gastric bypass surgery; mean BMI decreased from 45.7 kg/m2 preoperatively to 32.9 kg/m2 at the time of follow up and 26 of the 32 patients reported decreased medication usage postoperatively. The mean scaled asthma symptom score decreased from 44.5 to 14.3 (p<0.001). Of the 10 patients with “severe” asthma before surgery, none remained in this category at follow up. Similar improvements in symptoms, medication usage, and asthma severity were noted postoperatively in a study of 40 obese asthmatics by Macgregor and Greenberg.30Weight loss has also been associated with improvement in pulmonary function in one other study of medical weight loss in obese asthmatics.31 In addition to the parallel increase in FEV1 and FVC noted in the introductory article, this study added the significant contributions of noting both decreased peak flow variability and decreased static airways resistance in these asthmatics after weight loss. Overall, reductions in obesity, both medically and surgically, have resulted in improvements in asthma symptoms, medication usage, and severity, and improvements in multiple aspects of pulmonary function in every study that has evaluated these outcomes.
Causal hypotheses
The consistency of the relationship, the temporal association, the dose-response curve, and the association with intermediate phenotypes has caused at least one author to suggest that there could be a causal relationship between obesity and the onset of asthma.32 In order to implicate a causal hypothesis, however, one or more plausible biological mechanisms must be established. Although few studies have specifically addressed this question, specific mechanisms relevant to this association can be easily elicited. Obesity may directly affect the asthma phenotype by direct mechanical effects, by enhancing the immune response, through related genetic mechanisms, and by sex specific influences (hormones). Alternatively, obesity may be closely linked to other environmental factors such as physical activity, diet, and birth weight. These environmental influences, in combination with genetic susceptibility, may then lead to enhanced susceptibility to asthma (box 1). The salient features of these mechanisms will be reviewed below.
Mechanisms relating obesity to asthma
- Mechanical
Alterations in tidal stretch leading to latch
Gastro-oesophageal reflux
- Immune modification
TNFα
IL-1β
IL-6
Leptin
- Genetic effects
Common candidate genes (TNFα, β2 adrenergic receptor)
Candidate regions (5q, 6p, 11q, 12q)
Obesity candidate genes related physiologically to asthma
Sex
Airway size differences
Inflammatory mediators enhanced in women
Oestrogen
Gene × environment interactions
Physical activity
Diet
Developmental
Fetal programming
Mechanical effects of obesity
Physically, obesity may affect asthma directly by decreased tidal excursion leading to smooth muscle latching and indirectly by enhancement of gastro-oesophageal reflux. The most consistent alteration in lung function found in obesity is a reduction in functional residual capacity (FRC) due to the effect of the abdominal contents on the position of the diaphragm.33 ,34Obesity has also been associated with decrements in tidal volume35 which fails to increase during times of dynamic stress such as exercise.36 ,37 Moreover, in morbid obesity, the majority of tidal breaths are taken around the closing volume.38 ,39 Decrements in FRC and low tidal volumes infer small cycling rates, resulting in the conversion of airway smooth muscle from rapidly cycling actin-myosin cross bridges to slowly cycling latch bridges (fig 1).40-42 The attainment of the latch state has been hypothesised to be the reason that obstruction persists in asthmatic airways.40 ,42 The latch state has also been postulated to result in increased airways responsiveness.40 ,42 Furthermore, these effects may be enhanced by breathing around the closing volume.42-45 The latch state may thus explain the observations that decrements in FRC, as occur in obesity, have been tightly correlated with increased airways resistance34 ,46 and responsiveness to methacholine.44

The Latch hypothesis. Obesity leads to decrements in functional residual capacity (FRC) and tidal volumes (Vt), resulting in dynamic decreases in smooth muscle stretch. The resultant latching of the smooth muscle leads to enhanced airways reactivity and irreversibility of obstruction. These effects may be enhanced by breathing around the closing volume, which is characteristic of morbid obesity.
In addition to its effects on FRC, tidal volume, and closing volume, obesity has been associated with decrements in forced expiratory flow in the mid portion of FVC (FEF25–75).47 ,48In turn, the FEF25–75 when related to vital capacity (FEF25–75/FVC) improves significantly with weight loss.31 The FEF25–75/FVC ratio has also been independently associated with methacholine responsiveness of the airways.49
Gastro-oesophageal reflux (GER) is commonly associated with asthma. The estimated prevalence of GER in asthmatics is 60–80% in adults and 50–60% in children.50 Possible mechanisms for GER related asthma symptoms include acid induced bronchoconstriction, either by direct microaspiration or by vagally mediated reflex.51 Medical or surgical treatment of GER results in an improvement in asthma symptoms in about 70% of patients.52 Obesity has been frequently cited as an independent risk factor for GER and GER symptoms,53-57although isolated studies have refuted this.58Mechanically, this effect may be mediated via increased abdominal pressures which increase the gastro-oesophageal pressure gradient.59 ,60 Both medical61 and surgical57 weight loss regimens have been associated with improvement in GER symptoms. These findings have led to the speculation that GER might mediate the relationship between asthma and obesity.27 ,29
Immune modification by obesity
There is increasing evidence in the literature that obesity is an inflammatory state. Studies to date have shown associations between tumour necrosis factor alpha (TNFα), interleukin 6 (IL-6), IL-1β, and C-reactive protein and the obese state.62-66Moreover, IL-6 and TNFα have been found to be constitutively expressed by adipocytes and to correlate with total fat mass.67 ,68 Finally, leptin—the protein product of the putative ob gene—is increased in the majority of obese individuals, probably due to insensitivity to endogenous leptin.69 In animal models exogenous leptin has been found to increase macrophage phagocytosis as well as to increase production of TNFα, IL-6, and IL-12 from lipopolysaccharide stimulated macrophages.70
Clearly, asthma is also a disease characterised by inflammation. While most of the recent focus has been on IL-4 and IL-5 as the primary cytokine mediators of extrinsic (allergic) asthma, there remains a substantial body of literature dedicated to the role of other cytokines in this disease. A brief review of the inflammatory markers noted in obesity and their role in asthma follows. Although leptin has not been studied in asthma, and C-reactive protein is generally considered a non-specific marker, IL-1 activity has been shown to increase in asthma.71 IL-1β has, in turn, been associated with induction of increased levels of IL-5 from CD4+ T cells.72In asthma, levels of circulating TNFα are increased and, upon exposure to allergens, the production of TNFα further increases.73 TNFα increases IL-4 mRNA production while IL-4 subsequently decreases TNFα production.74 TNFα also increases production of IL-5 by bronchial epithelial cells.75 IL-6 production is increased in asthma and has been associated with histamine, IL-4, TNFα, and IL-1 stimulation.73 ,76 It has been postulated that IL-6 is responsible for the modulation of IgE production by IL-4.77 Enhancement of IL-5 production has also been associated with IL-6 levels.72 Finally, it has been demonstrated that IL-6 causes substantial subepithelial fibrosis in animal models and may be a key modulator of airway remodelling in asthma.78
Genetic effects of obesity
Extensive genetic epidemiological studies individually focusing on asthma or on obesity have been performed in recent years. Reviews of the genetic epidemiology of these complex genetic traits are readily available.79-86 There are several ways in which obesity genes might influence the asthma phenotype. Firstly, genetic studies of each of these individual disease states have revealed several candidate genes that have been linked or associated with both obesity and asthma. Secondly, other obesity candidate genes are clustered in chromosomal regions that have been linked to asthma. Their close proximity may indicate increased potential for inheritance of these two traits simultaneously. Finally, candidate genes for obesity may encode protein products that may directly influence the asthma state, such as the cytokines noted in the previous section.
There are two genes in which linkage or strong associations have been found for both the obesity and asthma disease phenotypes. These singular candidate genes include genes encoding for the β2 adrenergic receptor and TNFα. The gene encoding for the β2 adrenergic receptor is located on chromosome 5q31–q32. Polymorphisms of the β2 adrenergic receptor are thought to be associated with specific asthma phenotypes and response to treatments. In studies to date, the Gln27→Glu polymorphism of this receptor has been found to be associated with increased serum IgE levels87 and a protective effect against the methacholine challenge.88 The Agr16→Gly polymorphism has been associated with nocturnal asthma89and treatment response to β agonist agents.88 ,90
In obesity it is felt that genes involved in the regulation of catecholamine function may be of great importance because of the role they play in energy expenditure, both as hormones and as neurotransmitters. The Gln27→Glu polymorphism of the β2adrenergic receptor has been found to be significantly associated with overall obesity in a number of studies91 ,92 as well as with obesity in sedentary men.93 Although the Arg16→Gly polymorphism has not directly been associated with obesity, the Gly16 allele has been shown to be associated with a greater ability to lose weight than in those without the mutation.94
The TNFα gene complex is located on chromosome 6p21.3. The TNFα-30895 ,96 and LTαNcoI95 polymorphisms have each been associated with asthma. The LTαNcoI/TNF-308*2 extended haplotype, both individually97 and in conjunction with the HLA-DRB1*02 allele,98 has been associated with the prevalence of asthma in an Australian population. The latter haplotype98and the isolated TNF-308*2 polymorphism99 have also been associated with airway hyperresponsiveness. Concurrently, the TNFα gene has been linked to obesity in a population of Pima Indians.100 Additionally, polymorphisms at the TNFα-308 region have also been associated with BMI101 and obesity.102
Genome wide scans of asthma to date have noted several consensus regions of linkage.103 These regions include portions of chromosomal areas of 5q, 6p, 11q, and 12q. Comparative analysis of these positional loci for asthma with those of candidate genes for obesity shows considerable overlap (table 1). This supports the hypothesis that the underlying genetic susceptibility to asthma may be shared with that for obesity.
Some asthma linkage loci (associated asthma candidate genes) and obesity candidate genes in the same regions
Two positional candidate obesity genes with potential physiological relevance to asthma will be mentioned. The glucocorticoid receptor gene is located on chromosome 5q31–32. Polymorphisms in the glucocorticoid receptor gene have been associated with obesity, both at the Asn363→Ser locus104 and at theBclI restriction site.105 ,106Markers surrounding this gene have also been linked to obesity in a small study of obese French families.107 In asthma, increases in the numbers of the glucocorticoid receptor beta have been associated with increased disease severity and fatality.108 ,109 This, along with the prominent therapeutic role played by steroids in asthma, has led to the proposal of the glucocorticoid receptor gene as a candidate gene for asthma84 ,110 and asthma gene therapy.111 The gene encoding insulin-like growth factor 1 (IGF-1) is located on chromosome 12q23. The 5′ region of this gene contains a dinucleotide (CT)n repeat. Comparison of the homozygous wild type (189 bp) IGF-1 gene with persons containing at least one longer allele has shown a significant association between baseline percentage body fat, fat free mass, and change in fat free mass with exercise and the IGF-1 polymorphic alleles.112 This same study evaluated sibling pairs and noted a significant linkage of the IGF-1 region with change in fat free mass.112 In the airway, bronchial epithelial cells have been found to produce IGF-1 after injury, stimulating myofibroblast proliferation,112 and to act as a mitogen for airway smooth muscle cell proliferation when co-cultured with leukotriene D4.113 This has led to the hypothesis that IGF-1 may be of importance in the airway remodelling characteristic of chronic asthma.113-115
Sex specific effects of obesity
The association between obesity and asthma has been particularly strong in adult women and postpubertal girls. In a survey of 19 126 Dutch adults, women with a BMI of ⩾30 had 1.8 times the risk of having asthma than non-obese women.12 This relationship was not seen in men. Other studies which have found differences between men and women in the association between asthma and BMI have reported that the association is found exclusively in women13 ,22 or is stronger in women than in men.15 In a study of 16 862 children aged 9–14, BMI correlated with the prevalence of asthma in both boys and girls. Interestingly, asthma risk was negatively related to Tanner stage in boys (RR of 0.3 for stage V compared with stage I) but was positively related to Tanner stage in girls (RR of 1.6 for stage V compared with stage I).25
The sex differences noted in obese asthmatic subjects may be just a reflection of the increased incidence116 and prevalence4 ,117 ,118 of asthma in women of any size. This has been postulated as a primary airway size effect.116However, women also appear to have a higher prevalence of airway hyperresponsiveness than men119 ,120 which persists despite adjustment for airway size. Although the mechanisms behind these associations have yet to be clarified, obesity may amplify these associations via the mechanical effects noted above. Similarly, leptin levels121-123 are higher in women than in men and may portend to an enhanced inflammatory state.
One other potential reason for the sex difference noted is that of the sex hormone oestrogen. Postmenopausal hormone replacement therapy (HRT) has been associated with a significantly increased relative risk of incident asthma in women (RR 1.49 for ever using HRTv never using HRT).124 In obesity, although androgen levels are increased, peripheral aromatisation of androstenedione to oestrone and testosterone to oestrogen occurs within the stroma of adipose tissue.125Combined with decreased sex hormone binding globulin found in obesity, this results in an oestrogen amplification effect on sensitive tissues.125 During the menstrual cycle, peak oestrogen levels have been associated with increased symptoms and decreased pulmonary function in asthmatic women.126 Recent data have shown that oestrogen administration results in a shift in the immunological reaction from a Th1 to a Th2 type.127 Other studies have demonstrated that oestrogen increases IL-4 and IL-13 production from blood monocytes128 and increases eosinophil recruitment129 and degranulation.130 These changes exemplify those typically found in asthma.
Gene × environment interactions in the asthma-obesity relationship
Despite numerous genetic and environmental associations relating asthma to obesity, it is unlikely that the noted relationship is due to any one single factor. Rather, it is the interactions between genes and environment131 that may best explain the variability of the expressed obese asthmatic phenotype. We will briefly touch upon the potential aetiological roles of physical activity, diet, and the in utero environments in the subsequent development of obesity and asthma.
Physical activity and asthma
Studies of the association between obesity and asthma have noted the expected negative relationship and close correlation between physical activity and body mass index.24 ,132 Several authors have speculated that the relationship between obesity and asthma may just be a reflection of a sedentary lifestyle.10 ,133 Lack of full lung expansion associated with exercise may lead to increased airways responsiveness.45 ,134 In recent studies, increased physical fitness has been associated with decreases in the relative risk of incident asthma in schoolchildren135 and in twins discordant for the diagnosis of asthma.136 In the study of schoolchildren, decreased physical fitness was also significantly correlated with the subsequent development of airways hyperresponsiveness to methacholine.135
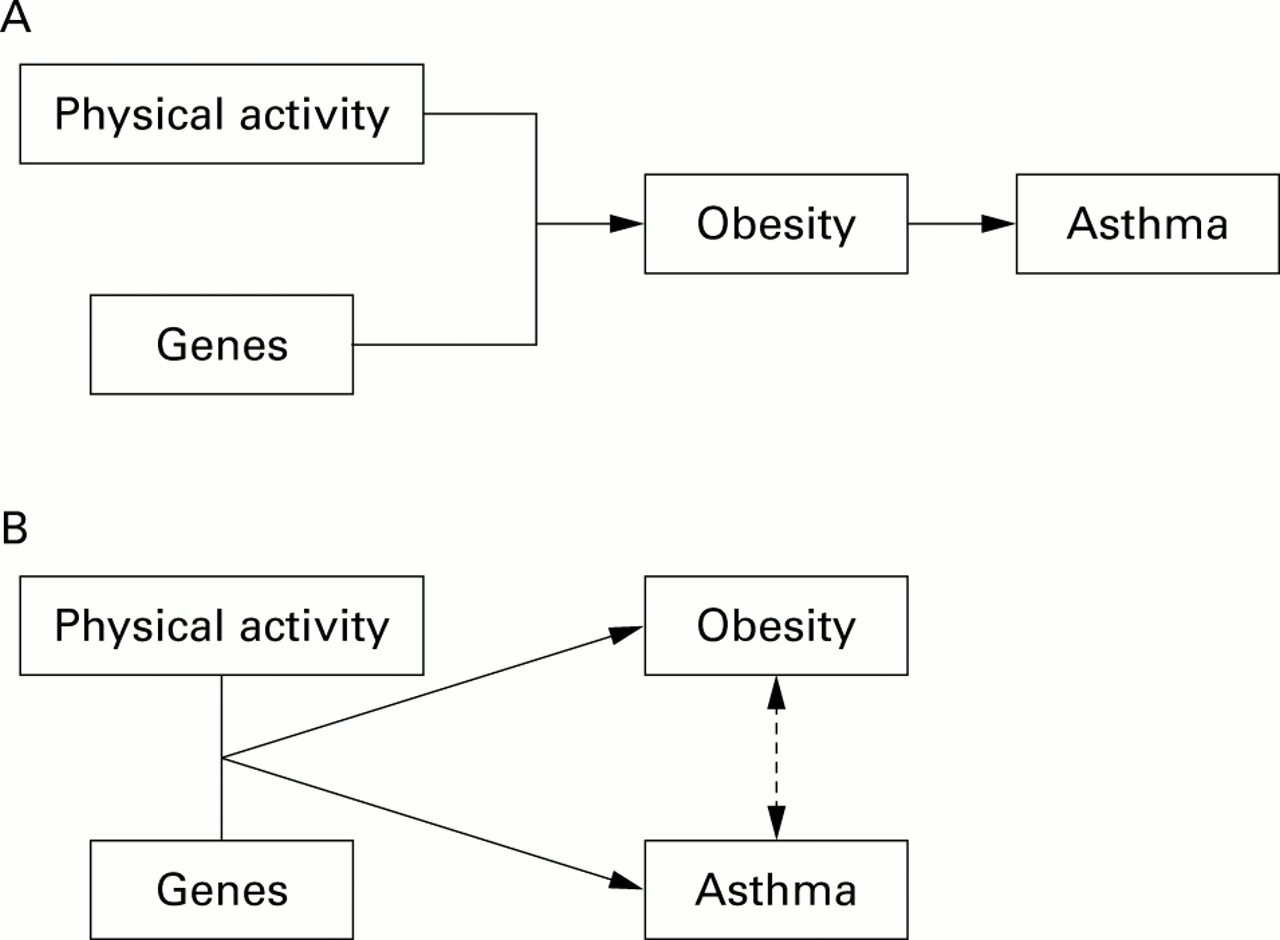
While the level of physical activity may be an independent risk factor for the development of asthma, it may also interact with genetics in its association with asthma. There are two possible mechanisms for such gene × environment interactions in the relationship between obesity and asthma (fig 2). Firstly, environmental factors such as physical activity may interact with genetic predisposition to produce obesity which subsequently leads to the development of asthma via the pathways described above. Alternatively, the same environmental and genetic influences may result in the independent development of both asthma and obesity. The association between asthma and obesity may then be further influenced by the mechanisms previously described. As an example, in a recent abstract137 BMI and the Arg16→Gly polymorphism of the β2 adrenergic receptor were associated with incident asthma, but only in a subset of sedentary women.
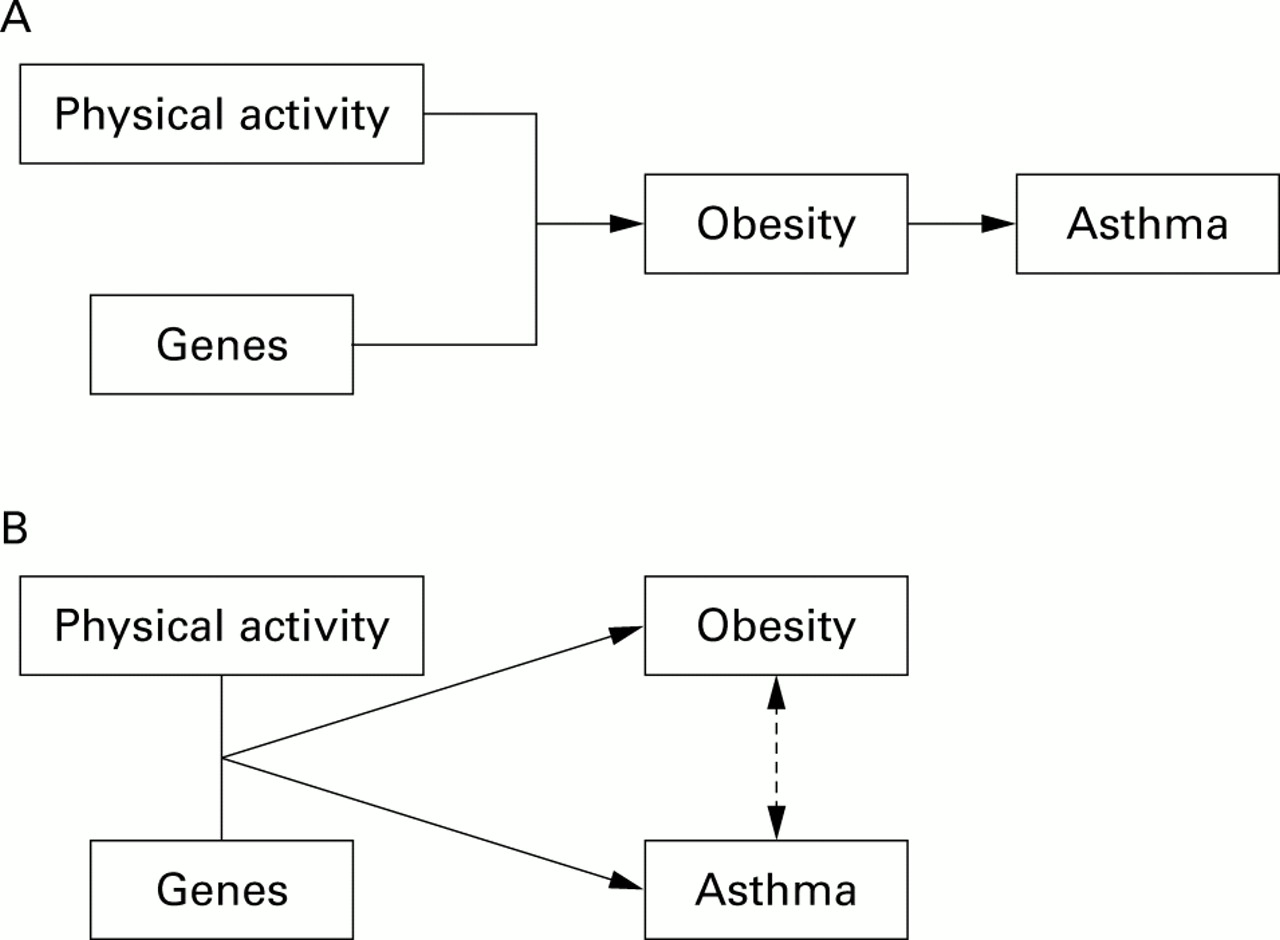
Possible mechanisms for gene × environment interactions in the relationship between obesity and asthma. (A) Altered physical activity levels may interact with genetics resulting in obesity which subsequently leads to the development of asthma. (B) Alternatively, physical activity and genetic influences may portend to the independent development of asthma and obesity. Asthma and obesity may then further influence the expression of each other. Other environmental factors such as diet may interact with obesity and asthma via similar mechanisms.
Diet and asthma
The relationship between diet and obesity is an obvious one. Interestingly, obese subjects may consume no more calories than lean controls.138 Analysis of the NHANES I data based on 24 hour food recalls actually found a negative correlation between overeating and overweight.139 However, the type of food consumed by obese individuals tends to be of poor nutritive value138 and to be rich in total fat.140 ,141Levels of vitamins A, C, E, carotenes, riboflavin, pyridoxine, zinc, and magnesium have been noted to correlate negatively with body fat.142 ,143 Paradigms for the treatment of obesity include decreasing total fat intake and ensuring adequate intake of vitamins and minerals.2
The dietary factors mentioned above may affect asthma as well. Total fat intake has been associated with the diagnosis of asthma.144 ,145 Zinc and magnesium deficiencies have been associated with asthma symptoms and bronchial reactivity.146-148 Zinc deficiency may also lead to an enhanced Th2 immune response.149 Oxidant stress may enhance the inflammatory response of the respiratory tract, so much attention has been devoted to the relationship between dietary antioxidants and asthma. While vitamins A, E, carotene, riboflavin, and pyridoxine have been associated with reduced lung function and asthma, their role remain controversial.150-152 The role of vitamin C is more compelling. Lower vitamin C levels have been associated with a high prevalence of asthma in adults153and in children,154 increased respiratory symptoms,155 reduced pulmonary function,156-158 and increased airways responsiveness.146 Supplementation with vitamin C has been shown to decrease asthma severity and frequency,159exercise induced bronchospasm,160 and airways responsiveness to methacholine.161
While no specific gene × environment studies of diet in relation to obesity and asthma have been performed, based on the above associations one can postulate that the paradigm illustrated in fig 2applies to dietary influences as well—that is, genes in combination with dietary foods which are high in total fat and low in nutritive value and antioxidants lead to obesity. These may also lead to asthma, either via obesity or by exerting independent effects on the asthma phenotype.
One other nutrient should be mentioned—namely, sodium. BMI and salt load are closely correlated with each other.162 Blood pressure studies have revealed decreased levels of atrial natriuretic factor163 ,164 and increased aldosterone relative to plasma renin levels164 ,165 in obesity. Additionally, adipocytes are known to produce angiotensin II166 and leptin has direct sympathetic effects on the renal outflow tract,167 both of which may lead to the sodium retention seen in obesity. In asthma, excess sodium has been associated with increased airways reactivity in a number of studies,168-171 although other studies did not note this finding.172-174 Following sodium restriction in three double blind clinical trials, improvements were noted in airways responsiveness,175 ,176FEV1,176 ,177 and asthma symptoms.176 ,177
Learning points
Obesity has been associated with increases in the incidence and prevalence of asthma in a number of epidemiological studies of adults and children.
Weight loss in obese asthmatic subjects results in an improvement in overall pulmonary function and asthma symptoms, as well as decreases in asthma medication usage.
Obesity may directly affect the asthma phenotype by mechanical effects including airways latching, by cytokine modulation via adipose tissue, through common genes or genetic regions, or by sex specific effects including the hormone oestrogen.
Obesity may also be related to asthma by genetic interactions with environmental exposures, including physical activity and diet.
The Barker hypothesis may underscore the developmental relationship of obesity with asthma.
Developmental effects
Asthma is primarily a disease of early childhood with 90% of all cases being diagnosed by the age of 6. There is increasing evidence that prenatal, neonatal, and early childhood events affect the subsequent development of asthma.178-182 The idea that fetal programming can affect the subsequent development of chronic disease was popularised by Barker and colleagues183-186and is often referred to as the Barker hypothesis. This fetal origins hypothesis proposes that these diseases originate through adaptations which the fetus makes when it is undernourished. Such diseases may be consequences of “programming” whereby a stimulus or insult at a critical sensitive period of early life results in long term changes in physiology or metabolism.187-189 Maternal nutrition may play a role in this programming, although this remains controversial.190 Associations have been noted between low maternal BMI191 and failure to gain weight during the first trimester192 and lower birth weight. Similarly, higher maternal BMI and excessive weight gain tends to result in infants with a higher birth weight.192-194
Fetal programming and birth weight have been correlated with the subsequent development of obesity. Studies have noted that low birth weight is associated with increased percentage body fat195and central fat distribution in children.196 These findings have been confirmed in a recent analysis of NHANES III data.197 Increased arm fat in small for gestational age babies has been noted as early as 2–5 months of age when compared with average babies.195 Low birth weight has also been associated with centripetal obesity in adolescents198 and adults.199-201 At the other extreme of birth weight, fetal macrosomia has been associated with the subsequent accumulation of excess subcutaneous fat in childhood202 and the development of obesity as adults.203 One plausible biochemical link between these apparently disparate associations is leptin. Umbilical cord leptin levels are increased both in large for gestational age neonates204 ,205 and in intrauterine growth retarded humans204 and animals.206Thus, infants exposed to poor nutrition during the early trimesters may be programmed for enhanced leptin production and subsequent adipose tissue deposition, while those overweight infants exposed to high nutrition, especially late in pregnancy, exemplify increased leptin concentrations typical of the obese adult.
Low birth weight has also been associated with asthma risk. Barkeret al noted that lower birth weight was associated with lower lung function and increased risk of death from obstructive airways disease in adults.207 Since then, consistent reports of associations between low birth weight and an increased risk of asthma have appeared.15 ,208-213 The mechanism behind this relationship may be a compromised development of the lungs.207 ,214 ,215 Asthma has not been associated with high birth weights, although asthma216 and increased IgE levels217-220 have been correlated with large head circumference at birth.
The prototypical example of the relationship of fetal development to both asthma and obesity is the Dutch winter famine of 1944–5. Women exposed during early and mid pregnancy to the severe nutritional limitations imposed by the famine had offspring of reduced birth size.221 ,222 The risk of obstructive airways disease was also increased in those exposed to famine in early and mid gestation, but not in late gestation.223 Interestingly, in separate follow up studies, the prevalence of obesity was higher in men exposed to famine during early to mid gestation and lower in those exposed during the last trimester,224 and higher in women exposed early in gestation.225
Ultimately, all fetal programming phenomena must have their basis in the altered expression of genes.190 Interactions of the in utero environment with fetal genes may thus also contribute to the development of obesity and asthma (fig 3). Studies investigating this relationship are in progress.

{kind=link}
{kind=link}
{kind=link}
In combination with genetic influences, alterations in the intrauterine nutritive environment can lead to diminished fetal growth (IUGR) during early gestation or increased birth weight during late gestation. Both are associated with the subsequent development of obesity. Fetal programming and the extremes of birth weights may also lead to asthma.
Conclusion
We conclude that there is a significant temporal relationship between alterations in body mass and asthma. While probably multifactorial, the potential independent effects of biomechanics, inflammation, genetics, and sex specific effects belie the closeness of the obese and asthma phenotypes. The likelihood of additional direct, interactive, or otherwise related contributions of physical activity, diet, and in utero development to the relationship between BMI and asthma further strengthens this notion. That there are so many theoretical hypotheses underlying this relationship only enhances the intrigue related to suspected causality.
Acknowledgments
Supported by NIH 2T32: HL07427–21, The Clinical Epidemiology of Lung Diseases and by NIH R01: HL66795, Innate Immunity in Heart, Lung, and Blood Disease.