Article Text

Abstract
BACKGROUND Permanent smoking cessation reduces loss of pulmonary function. Less is known in the long term about individuals who give up smoking temporarily or quitters with lower initial pulmonary function. Little is known also about the relationship between decline in pulmonary function and mortality. We examined these aspects and the association between smoking, decline in pulmonary function, and mortality.
METHODS Two middle aged male Finnish cohorts of the Seven Countries Study and their re-examinations on five occasions during a 30 year period of follow up were analysed.
RESULTS During the first 15 years (n=1007) adjusted decline in forced expiratory volume in 0.75 seconds (FEV0.75) was 46.4 ml/year in never smokers, 49.3 ml/year in past smokers, 55.5 ml/year in permanent quitters, 55.5 ml/year in intermittent quitters, and 66.0 ml/year in continuous smokers (p<0.001 for trend). Quitters across the entire range of baseline FEV0.75 had a slower decline in FEV0.75 than continuous smokers. Among both continuing smokers and never smokers, non-survivors had a significantly (p<0.001) more rapid decline in FEV0.75 than survivors. The adjusted relative hazard for total mortality was 1.73 (95% confidence interval (CI) 1.41 to 2.11) and 1.24 (95% CI 1.02 to 1.52) in the lowest and middle tertiles of decline in FEV0.75. Never smokers, past smokers, and quitters had significantly lower total mortality than continuous smokers, partly because of their slower decline in FEV0.75.
CONCLUSION These results highlight the positive effect of smoking cessation, even intermittent cessation, on decline in pulmonary function. Accelerated decline in pulmonary function was found to be a risk factor for total mortality. The beneficial effect of smoking cessation on mortality may partly be mediated through a reduced decline in pulmonary function.
- smoking cessation
- lung function
- mortality
Statistics from Altmetric.com
Pulmonary function declines with the process of ageing and smoking is a major environmental factor in accelerating the decline in pulmonary function.1-9 Giving up smoking permanently has been shown to reduce loss of pulmonary function,1-9but less is known about decline in pulmonary function in individuals who give up smoking and later start to smoke again.2 ,10-12 Little is also known about the long term decline in quitters with impaired baseline pulmonary function, although they have benefited from smoking cessation in short follow up studies.1 ,2 Few previous studies have examined the association between the decline in pulmonary function and mortality.13-15 The association between smoking cessation and mortality is better described,16-18 but research into the question of whether reduction in the decline in pulmonary function is an intermediate link in the chain of causation between smoking cessation and mortality is lacking.
The Seven Countries Study provides data on pulmonary function for 30 years in a general population of middle aged Finnish men. This has given us an opportunity to examine the long term influence of cigarette smoking and smoking cessation, both permanent and temporary, on the decline in pulmonary function across the entire range of baseline pulmonary function. In mortality analysis we examined the effects of smoking cessation and decline in pulmonary function on all cause mortality and attempted to clarify the possible intermediate role of the decline in pulmonary function in the association between smoking cessation and mortality.
Methods
SUBJECTS
In 1959 all men (n=1711) aged 40–59 years from two rural areas in Finland were invited to participate in an international longitudinal study called the Seven Countries Study19 ,20 (the details of the Finnish study population have been described previously16). Re-examinations of the Finnish cohorts were performed in 1964, 1969, 1974, 1984, 1989 and the latest in 2000 (which does not include a measurement of pulmonary function). All deaths between 1959 and 1994 are known; the collection of death certificates was performed as described previously.16 In this study those men with complete data on smoking habits and decline in pulmonary function between 1959 and 1974 (n=1007) and between 1959 and 1989 (n=411), respectively, were included in the analyses. When analysing the association between the decline in pulmonary function (1959–1974) and total mortality (1974–1994) only those men with the full data needed for multivariate analyses were included (n=932).
LUNG FUNCTION MEASUREMENTS AND CALCULATION OF RATE OF CHANGE
Between 1959 and 1974 forced expiratory volume in 0.75 seconds (FEV0.75) derived from spirometric tests was used as a measurement of pulmonary function. The spirometric test was performed using the McKerrow spirometer and the technique has been described before in detail.16 In 1984 and 1989 spirometric recordings were performed with the Vitalograph. In these years the best value from the two acceptable recordings—that is, within 200 ml of each other—in the standing posture was taken as FEV0.75. These values were, as before, corrected to BTPS and recorded in litres. The number of spirometric recordings was 1614, 1504, 1341, 1084, 646, and 410 in 1959, 1964, 1969, 1974, 1984, and 1989, respectively. (The number of men examined (alive) was 1675 (1711), 1558 (1595), 1393 (1428), 1174 (1225), 716 (770), and 470 (526) in 1959, 1964, 1969, 1974, 1984 and 1989, respectively.)
The adjustment of FEV0.75 values for height was achieved by dividing observed values by the square of each subject's standing height and then multiplying these figures by the square of the mean sample height.4 The annual change in height adjusted FEV0.75 values was calculated by using within-person linear regression for each subject having at least three acceptable FEV0.75 measurements. Of the men with both complete data on smoking habits and a linear regression during 1959–1974 (n=1007), 92 had three and 915 had four measurements of pulmonary function. Forty six men were excluded from the study because they had only two measurements between 1959 and 1974. Of those measured between 1959 and 1974, 411 survived until 1989 and had a linear regression during 1959–89 (of these, seven had three pulmonary function measurements, 12 had four, 77 had five, and 315 had all six measurements).
OTHER MEASUREMENTS
The recording of smoking habits has been explained in detail previously.16 For this study the men were classified as never smokers, past smokers at baseline, those who quitted smoking permanently (between 1959 and 1974) or intermittently, and continuous smokers. Subjects who were termed “intermittent quitters” were either baseline past smokers who reported smoking in at least one of the subsequent re-examinations or baseline smokers who relapsed back to smoking after giving up. Those smokers who did not give up smoking until the latter half of the follow up period were included as continuous smokers. The duration of smoking was measured at baseline in 1959 by asking the years of smoking.
Weight, height, blood pressure, electrocardiography (ECG), and total cholesterol measurements have been described elsewhere.20Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. The presence of coronary heart disease at each examination was defined as electrocardiographic evidence of old myocardial infarction—that is, a major Q wave on the ECG scan or a smaller Q wave with ST segment changes corresponding to Minnesota code items 1:1 or 1:2 and 5:1–221—a history of myocardial infarction verified in a hospital, or definite or probable angina pectoris assessed by a standard questionnaire.20 The presence of respiratory disease (physical or history of bronchial asthma, pulmonary emphysema, chronic bronchitis, pulmonary tuberculosis, bronchiectasis, pulmonary fibrosis, and thorax deformity) was evaluated each time by the examining physician.
STATISTICAL METHODS
Statistical analyses were performed using SPSS for Windows. The differences in the mean annual decline in FEV0.75 between smoking groups were evaluated by ANCOVA and the results are presented with an adjustment for age and initial level of pulmonary function. Only those men who had a within-person linear regression and complete data on smoking habits during the follow up period were included in ANCOVA analyses (n=1007 and n=411 in 1959–74 and 1959–89, respectively).
Cox's proportional hazards regression model was used to examine the effects of smoking status and annual decline in FEV0.75during 1959–74 on total mortality in 1974–94 after adjusting for other potential risk factors. To clarify the possible intermediate role of decline in pulmonary function in the association between smoking status and mortality, two models were fitted, one without decline in pulmonary function (model 1) and one in which decline in pulmonary function was included (model 2).
A total of 932 men were included in the mortality analyses. For these analyses the decline in FEV0.75 between 1959 and 1974 was divided into three tertiles. Initial pulmonary function and values (in 1974) of diastolic blood pressure and total cholesterol were included in the models as continuous variables, the presence of coronary heart disease between 1959 and 1974 was included as a dichotomous variable, and BMI (in 1974) was included as a variable with three categories (⩽18.99, 19.00–24.99, ⩾25.00). Smoking status was classified into five categories on the basis of smoking data from 1959–74 (never, past, permanent and intermittent quitters, and continuous smokers). An additional adjustment for smoking was made using the baseline duration of smoking as a continuous variable and the baseline amount of smoking as a dichotomous variable (<20 and ⩾20 cigarettes/day). Additional adjustment was also made for the presence of respiratory disease between 1959 and 1974 (a dichotomous variable).
Results
The adjusted decline in FEV0.75 during the first 15 years was significantly slower in never smokers, past smokers, permanent and intermittent quitters than in subjects who continued to smoke (table 1). The test for a linear trend between smoking categories was also significant. The duration of baseline smoking was significantly (p<0.001) shorter in past smokers, permanent and intermittent quitters than in continuous smokers (17.8, 24.9, 21.8, and 27.1 years, respectively). Adjusting for the duration of smoking did not, however, change the differences in decline in FEV0.75between smoking categories, nor did adjustment for the baseline number of cigarettes smoked or for a prevalent respiratory disease during the follow up period (not shown).
Mean annual decline1-150 in FEV0.75 during the first 15 years
Smoking cessation diminished the decline in FEV0.75 across the entire range of baseline FEV0.75 (table 2) with p<0.001 for smoking cessation and p=0.044 for tertile of baseline FEV0.75 (ANCOVA). Both past smokers and permanent quitters were included in the category of quitters to ensure a reasonable number of men for the analyses. The interaction effect between smoking cessation and tertile of baseline FEV0.75 on the decline in FEV0.75 was not significant (p=0.765) which means that the beneficial effect of smoking cessation on the decline in FEV0.75 was similar at all tertiles of baseline FEV0.75.
Mean annual decline2-150 in FEV0.75 during the first 15 years by smoking status and baseline tertile of FEV0.75 2-151
During 1959–89 never smokers, past smokers, permanent and intermittent quitters lost significantly less FEV0.75 than subjects who continued to smoke (table 3). Adjusting for the baseline duration of smoking, the baseline amount of smoking, or for a prevalent respiratory disease during the follow up period did not change this result either (not shown).
Mean annual decline3-150 in FEV0.75 during the whole 30 years
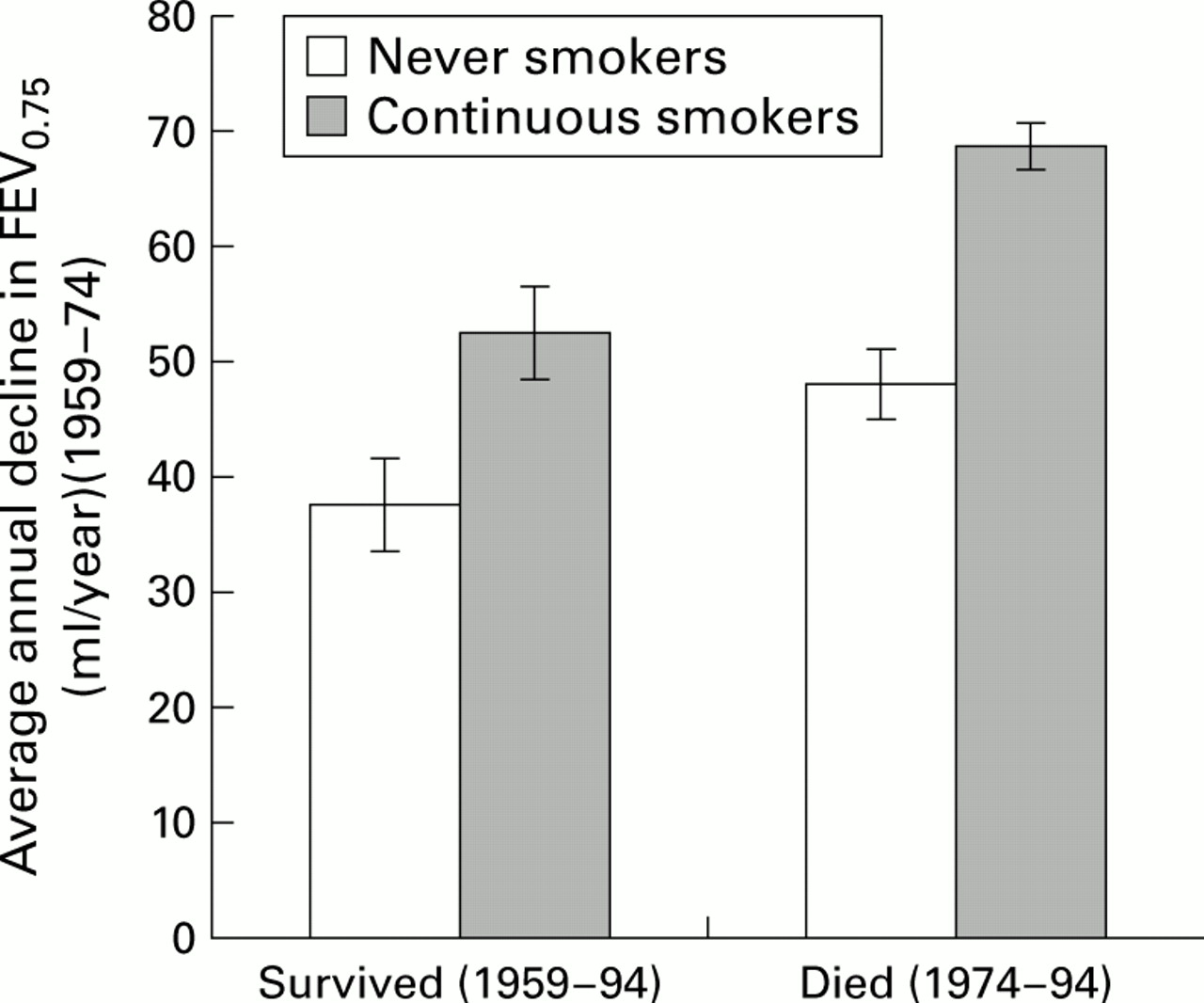
Among both continuing smokers and never smokers, non-survivors had a more rapid decline in FEV0.75 than survivors (fig 1). Differences in the decline in FEV0.75 had a significant effect on survival (p<0.001) and smoking (p<0.001) but there was no significant effect of the interaction of smoking and survival (p=0.365). The duration of baseline smoking was significantly shorter in surviving than in non-surviving continuous smokers (24.3 and 26.6 years, respectively). However, among smokers, additional adjustment for the baseline duration of smoking was not significant (p=0.938, not shown).

Mean annual decline in FEV0.75 (ml/year) with standard error bars in selected smoking groups by survival status adjusted for age, baseline pulmonary function, and smoking. p<0.001 for age, p<0.001 for baseline pulmonary function, p<0.001 for smoking, p<0.001 for survival, and p=0.365 for smoking*survival (all ANCOVA).
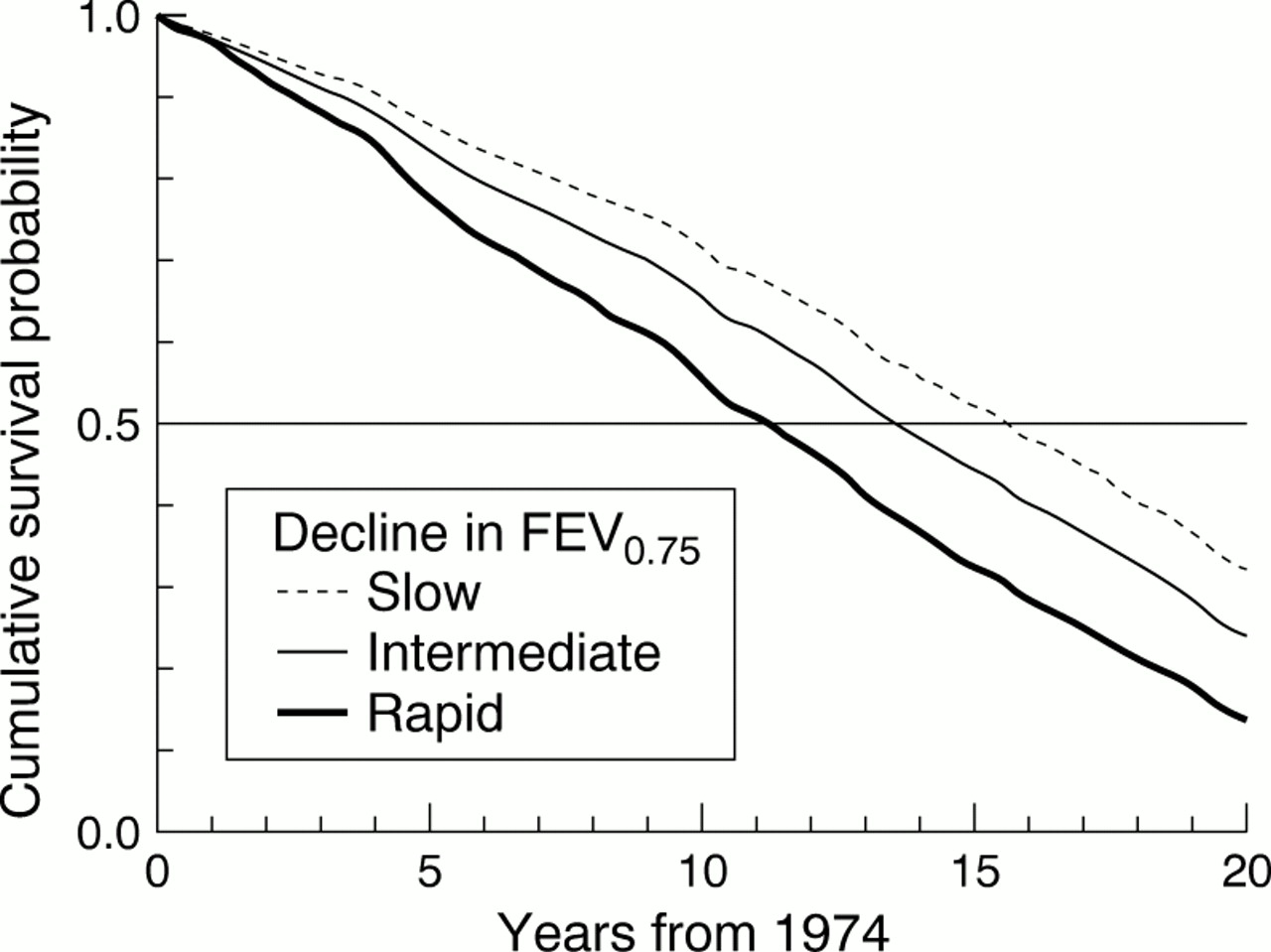
During 1974–94 there were 684 deaths. According to model 2 (table 4), both smoking status between 1959 and 1974 and annual decline in FEV0.75 between 1959 and 1974 predicted significantly and independently the total mortality between 1974 and 1994. Additional adjustment for the baseline duration of smoking, the baseline amount of smoking, or for a prevalent respiratory disease during the follow up period did not change the observed association between accelerated decline in FEV0.75 and increased all cause mortality (not shown). Figure 2 illustrates the effect of the rate of decline in FEV0.75 on survival.
Multivariate adjusted hazard ratios4-150 for all cause mortality during 1974–94 by selected variables
{kind=link}
{kind=link}
Cumulative survival probability curves for 1974–94 in the three tertiles of FEV0.75 decline (1959–74) based on Cox's proportional hazards regression model (adjusted for age, baseline pulmonary function, body mass index, diastolic blood pressure, total cholesterol, smoking status, and coronary heart disease).
The possible intermediate role of decline in pulmonary function in the causal pathway from smoking (and smoking cessation) to mortality can be assessed by comparing the differences between smoking categories based on model 1 which includes only control variables and smoking status and on model 2 which includes control variables, smoking status and decline in pulmonary function. The results show that the introduction of decline in pulmonary function into the model clearly reduced the differences between smoking categories. This suggests that part of the effect of smoking habits and changes in these habits on total mortality is due to their effect on the decline in lung function. For example, in model 1, those who had stopped smoking had 30% lower total mortality (HR 0.73 (95% CI 0.59 to 0.89) than continuous smokers; adjusting for decline in FEV0.75 reduced the difference to 20% (HR 0.80 (95% CI 0.65 to 0.99)). Thus, it can be estimated that about one third of the effect of smoking cessation on the decline in total mortality was mediated through its effect on pulmonary function.
Discussion
In this study never smokers, past smokers, those who quitted smoking permanently or intermittently lost less of their pulmonary function in later adult life than continuous smokers. The beneficial effect of smoking cessation on decline in FEV0.75 was similar in all tertiles of baseline FEV0.75. The rates of decline are consistent with those published in previous studies.2-4 Decline in pulmonary function was evaluated in a relatively large sample of men who lived in a non-polluted rural area, most of whom were farmers or forestry workers. Spirometric tests were performed using standard criteria during the same season of the year, and 87–97% provided satisfactory spirometric data in all surveys. The random variability of the change in FEV0.75was reduced by restricting the analysis to those subjects with at least three measurements. The number of men excluded because they had only two measurements was low. Since impaired pulmonary function is a risk factor for failure to perform acceptable spirometric tests later,22 selective attrition could occur in those subjects with low pulmonary function and rapid rates of decline4 ,23 which would actually attenuate the association between smoking and decline in pulmonary function.22 ,24
The results can be compared with other studies which have used FEV1 because FEV0.75 can be assumed to measure approximately the same as FEV1 (FEV0.75 needs to be multiplied by 1.09 to estimate FEV1).25The estimated mean annual decline in FEV0.75 between examinations may have been affected by the change in the equipment and the posture of measurement during follow up, and this may be one of the reasons why the annual decline in FEV0.75 was slower during the whole follow up period than at the beginning. However, the changes in the equipment and the posture of measurement do not disturb the comparisons between smoking categories because all participants were measured similarly in each examination.
Our finding of a significant trend across smoking categories from non-smokers through quitters to continuous smokers highlights greater benefits of earlier smoking cessation. When the duration of smoking is shorter, the effects of smoking are partially reversible—that is, the bronchoconstrictive or inflammatory effects may become normalised.6 In two earlier studies the decline in pulmonary function was faster in those who relapsed back to smoking than in continuous smokers.10 ,11 In contrast, our data support the findings of the Lung Health Study that intermittent quitters also benefit from smoking cessation, which suggests that continuous stimulation of the inflammatory response may lead to more profound functional and anatomical changes in the lungs.12
Fletcher et al have reported that smokers not susceptible to chronic airflow limitation may have only a slightly worse decline in pulmonary function than never smokers.7Thus, longitudinal studies may underestimate the effect of smoking on the decline in pulmonary function because of the survivor effect, particularly among the elderly.6 ,26 In our study surviving never smokers lost less FEV0.75 than surviving smokers. On the other hand, during the first half of the follow up period surviving smokers had a slower decline in FEV0.75than those smokers who did not survive. However, there was a similar but smaller difference between surviving and non-surviving never smokers. This result suggests that survivors generally have a tendency to a slower decline in FEV0.75. The reasons may be genetic and include, among other things, bronchial hyperresponsiveness,27 or they may be behavioural and include other protective factors such as higher physical activity28 or a higher intake of fruit and vegetables,29 both factors associated with better pulmonary function.
In this study we found that accelerated decline in FEV0.75was associated with increased all cause mortality. A few earlier studies have described the association between the decline in pulmonary function and mortality.13-15 In the Honolulu Heart Program a 6 year decline in FEV1 was significantly related to all cause mortality in smokers.13 In the Busselton Health Study a 6 year decline in FEV1 predicted increased all cause mortality significantly among women.14 In the Baltimore longitudinal study of ageing, an accelerated decline in FEV1 increased cardiac mortality.15
In a previous study we found that quitters had lower total mortality and lower mortality from cardiovascular disease than continuous smokers, which was probably explained mainly by atherosclerotic and thrombotic mechanisms.16 We also found that men with impaired initial pulmonary function had an additional benefit from smoking cessation on mortality from cardiovascular disease, which we thought resulted from a decrease in the decline in pulmonary function. Our present results support this hypothesis because we have now found that part of the reduction in total mortality among quitters is explained by their slower decline in pulmonary function.
An increased decline in pulmonary function can lead to the development of chronic obstructive pulmonary disease2 ,5 and it also seems to be a risk factor for mortality. It is therefore crucial to identify measures to prevent any additional deterioration. In our study smoking cessation had a great advantageous effect. However, it has been shown that, for many smokers, the process of quitting requires several attempts before the habit is eliminated.30 It is therefore encouraging that intermittent quitters, as well as smokers across all levels of baseline pulmonary function, gain protection against an accelerated loss of pulmonary function. Thus, too much emphasis cannot be given to the importance of smoking cessation. Further studies are needed to elucidate the other mechanisms which result in a decline in pulmonary function.
References
Footnotes
Supported by grants from the Finnish Academy, the Finnish Anti-Tuberculosis Association Foundation, the Finnish Lung Health Association, and the National Institute on Aging, USA (grant EDC-1 1 RO1 AGO8762–01A1).