Article Text

Abstract
BACKGROUND For patients with non-small cell lung cancer the TNM staging system and other conventional prognostic factors fail to predict accurately the outcome of treatment and survival. This study attempts to determine the prognostic value for survival of the proportions of CD4+ lymphocytes in the pleural cavity (PLY) of patients with resectable non-small cell lung cancer.
METHODS Lymphocytes in the pleural cavity separated from 51 patients with non-small cell lung cancer were examined by flow cytometry to measure the proportions of CD4+ PLY. Univariate and multivariate analyses were performed to assess the association between the proportion of CD4+ PLY and survival.
RESULTS The 5 year survival rate of patients with percentage CD4+ PLY of ⩽30% was 84% whereas that of patients with %CD4+ PLY >30% was 26.9%. The difference in survival between the %CD4+ PLY ⩽30% and %CD4+ PLY >30% groups was significant (p<0.0001). The %CD4+ PLY in those who survived for 5 years was significantly lower than that in the patients who died within 5 years (p<0.0001). The difference in survival between patients with stage IA and IB lung cancer with %CD4+ PLY ⩽30% and those with %CD4+ PLY >30% was also significant (p =0.015). Multivariate analysis showed that the proportion of CD4+ PLY (hazard ratio=6.9, 95% CI 0.045 to 0.47) and nodal status (hazard ratio=22.7, 95% CI 0.006 to 1.806) are significant and independent prognostic factors for the survival of patients with lung cancer.
CONCLUSIONS The proportion of CD4+ PLY may help to select patients who are likely to have a poorer prognosis after surgery and therefore may be suitable for consideration of adjuvant treatments. These results need confirmation in a larger prospective study.
- lung cancer
- prognosis
- CD4
Statistics from Altmetric.com
For patients with lung cancer, conventional prognostic factors such as TNM stage, the extent of lymph node metastasis, and performance status currently determine the choice of treatment. However, considerable differences in outcome after treatment are seen between patients with the same initial stage and performance status.1 ,2 The influence of additional variables may explain this heterogeneous prognosis. New prognostic factors are needed to improve the understanding of the biological behaviour of lung cancer and to recognise patients with a good or poor prognosis.
The cell mediated arm of immune surveillance plays a major role in the destruction of cancer cells. A quantitative measure of cell mediated immunity is the measurement of proportions of CD4+ and CD8+ lymphocytes. The proportion of CD4+ cells in peripheral blood lymphocytes (PBL) in patients with malignancy decreases according to tumour progression and the decrease in the proportion of CD4+ PBL is associated with a poor prognosis.3-5 Impaired cellular immunity can be associated with a change in the proportions of these cells.
Malignant pleuritis is frequently observed in lung cancer6-11 and patients with malignant pleuritis have a poor prognosis. In malignant pleural effusions CD4+ cells are dominant, and the proportion of CD8+ cells is significantly lower than that of CD4+ cells.12-15 In contrast, the proportion of CD4+ cells in the pleural cavity of lung cancer patients without malignant effusion is significantly lower than that of CD8+ cells.16 ,17 Invasion of cancer cells into the pleural cavity may be affected by both the nature of the cancer cells and host factors of patients with lung cancer.18
We have examined the proportions of CD4+ and CD8+ lymphocytes in the pleural cavity (PLY) of patients with resectable non-small cell lung cancer to determine whether the proportions of these cells have a prognostic value for patient survival.
Methods
PATIENTS
The study subjects comprised 51 patients (42 men) of median age 66 years (range 46–83) with resectable primary lung cancer not associated with malignant pleural effusion. None of the patients had received any anticancer therapy prior to the study. Computed tomographic scanning and magnetic resonance imaging were used to determine whether a pleural effusion was present. The clinical characteristics of the patients are summarised in table 1. Histologically, there were 25 squamous cell carcinomas, 24 adenocarcinomas, and two large cell carcinomas. The TNM classification system (1997 international staging system for non-small cell lung cancer) was used for staging the disease. The degree of pleural invasion by lung cancer (p factor) was grade 0 (no visceral pleural invasion) in 34 patients, grade 1 (pleural invasion limited to the visceral pleura) in six patients, grade 2 (pleural invasion extending beyond the visceral pleura but not extending to the neighbouring lobe or chest wall) in three patients, and grade 3 (pleural invasion extending beyond the neighbouring lobe or chest wall) in eight patients. The degree of pleural invasion by cancer was determined by histological examination; 29 patients were classified as n0, seven as n1, 13 as n2, and two as n3. All of these patients were confirmed to have no malignant pleural effusion at the time of thoracotomy. Eight other lung cancer patients with malignant pleural effusion, who were not candidates for surgery, were also examined.
Clinical features of study patients
ISOLATION OF LYMPHOCYTES IN PLEURAL CAVITY
After obtaining informed consent, pleural lavage was performed as previously described.16 ,17 At thoracotomy it was confirmed that no malignant pleural effusion was present. The pleural cavity was then lavaged with 1000 ml of 0.9% NaCl solution at 37°C. The lavaged fluid was collected aseptically in heparinised (10 U/ml) centrifuge bottles and centrifuged at 1200 rpm (400g) for 10 minutes. The cell pellets were resuspended in 15 ml phosphate buffered saline and mononuclear cells were separated from the lavage fluid by discontinuous gradient centrifugation in lymphocyte separation medium. The absence or presence of malignant cells among the washed mononuclear cells was determined morphologically using May-Grunwald Giemsa staining. The lavage and isolation methods used yielded a mean 22.3 (SD26.9) × 106(range 1–117 × 106) mononuclear cells per patient. These cells consisted of 56.7 (13.1)% PLY. Isolation of PLY was immediately followed by FACScan analysis.
FLOW CYTOMETRY
A direct immunofluorescence assay was used to detect the surface markers of PLY. Monoclonal antibodies (OKT4a and OKT8) conjugated with fluorescein isothiocyanate (Ortho Diagnostics, Raritan, NJ, USA) were added to cell suspensions and the mixtures were incubated for 30 minutes at 4°C. The cells were then washed, resuspended in 0.1 ml phosphate buffered saline, and analysed with a FACScan flow cytometer.16 ,17 The monoclonal antibodies used were directed against lymphocyte antigens of CD4 and CD8. Before FACScan analysis, dead cells and non-lymphoid cells were excluded from analysis by light scatter gating.
STATISTICAL ANALYSIS
The statistical differences were examined by the Mann-Whitney U test. A p value of <0.05 was considered to be significant. Survival curves were calculated according to the method of Kaplan and Meier.19 The groups were compared by log rank test.20 Multivariate relationships were analysed according to Cox's proportional hazards linear model and the SAS program package.21
Results
The median %CD4+ PLY was 30.3% (5–95th percentile 9.5–60; range 6.4–82.7). Accordingly, the cutoff value for survival analysis in this study was assessed by 30% of CD4+ PLY. The 5 year survival rate of lung cancer patients with %CD4+ PLY ⩽30% was 84% while that of patients with %CD4+ PLY >30% was 26.9%. The median survival time of patients with %CD4+ PLY >30% was 24 months. The difference in survival between the %CD4+ PLY ⩽30% group and the %CD4+ PLY >30% group was significant (p<0.0001; fig 1A). The %CD4+ PLY in those who survived 5 years was significantly lower than that in the patients who died in less than 5 years (p<0.0001; fig 1B). The %CD4+ PLY in malignant effusions of lung cancer patients who were not candidates for surgery was significantly higher than in those who survived for 5 years (p<0.0001; fig 1B).
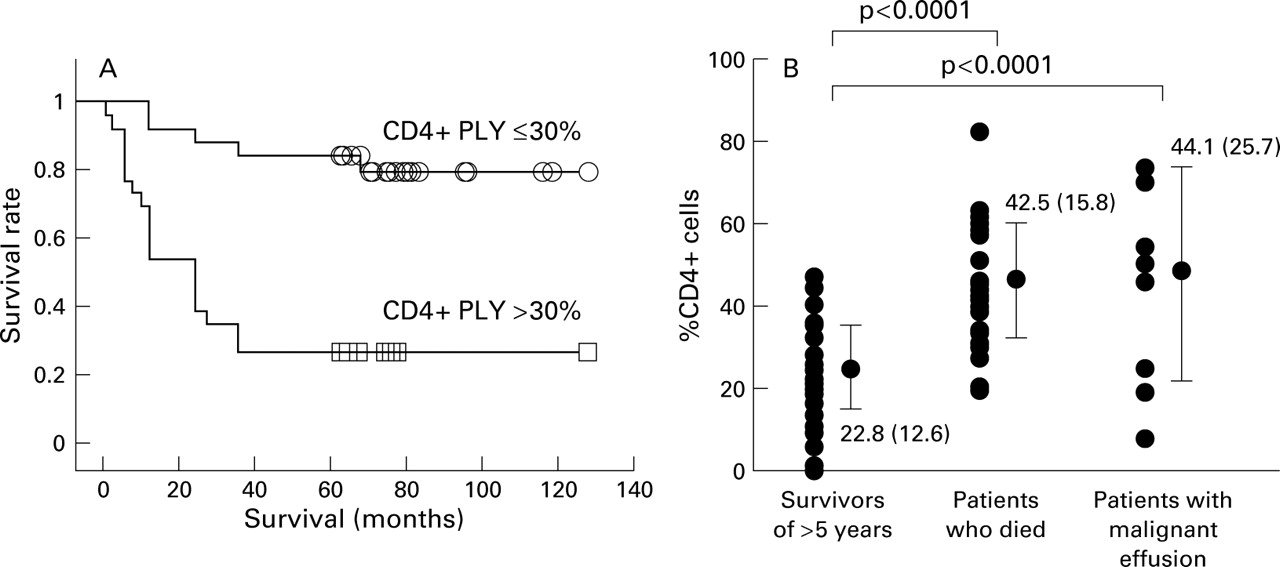
(A) Log rank survival of patients with %CD4+ PLY ⩽30% (n=24) or >30% (n=27). (B) There were eight patients with malignant pleural effusions who were not candidates for surgery.
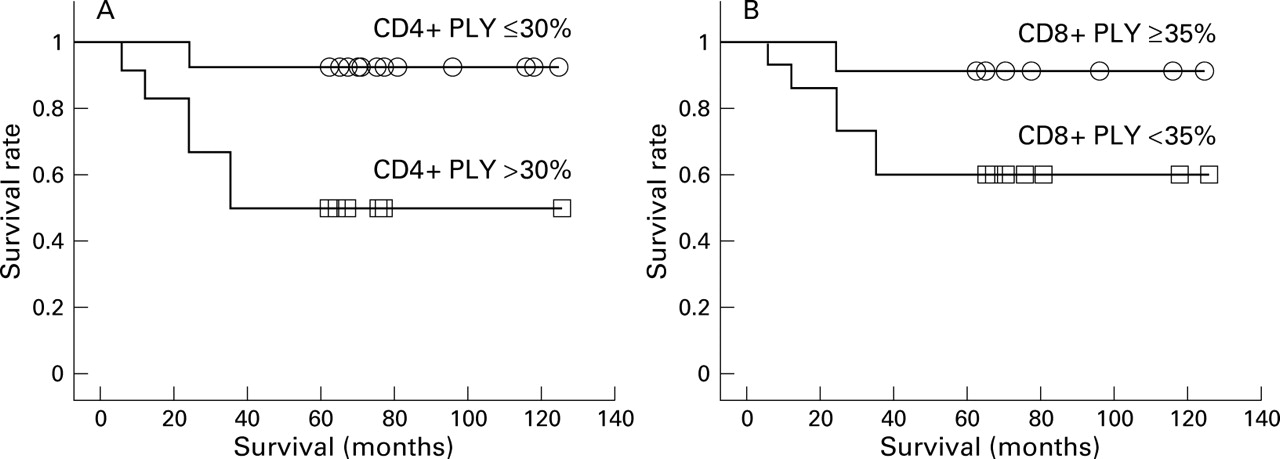
The median %CD8+ PLY was 33.2% (5–95th percentile 9.2–53.1; range 3.8–61.7). Accordingly, the cutoff value for survival analysis in this study was assessed by 35% of CD8+ PLY. The 5 year survival rate of lung cancer patients with %CD8+ PLY ⩾35% was 83.3% and that of patients with %CD8+ PLY <35% was 36.4%. The median survival time of patients whose %CD8+ PLY was <35% was 27 months. The difference in survival between the %CD8+ PLY ⩾35% group and the %CD8+ PLY <35% group was significant (p=0.0026; fig 2A). The %CD8+ PLY in those who survived 5 years was significantly higher than that in the patients who died within 5 years (p=0.0188; fig 2B). The %CD8+ PLY in malignant effusions of lung cancer patients was significantly lower than that in 5 year survivors (p=0.0159; fig 2B). The proportions of PLY expressing CD3, CD16, CD25, CD57, or HLA-DR were not associated with the prognosis of the patients with lung cancer (data not shown).

(A) Log rank survival of patients with %CD8+ PLY ⩾35% (n=18) or <35% (n=33). (B) There were eight patients with malignant pleural effusions who were not candidates for surgery.
The 5 year survival rate of patients with stage IA and IB lung cancer with %CD4+ PLY ⩽30% was 92.9% and that of patients with stage IA and IB disease with %CD4+ PLY >30% was 50%. The difference in survival between the %CD4+ PLY ⩽30% group and the %CD4+ PLY >30% group was significant (p=0.015; fig 3A). The 5 year survival rate of patients with stage IA and IB lung cancer with %CD8+ PLY ⩾35% was 90.9% and that of patients with stage IA and IB cancer with %CD8+ PLY <35% was 60%. The difference in survival between the %CD8+ PLY ⩾35% group and the %CD8+ PLY <35% group was not significant in these patients (fig 3B).

{kind=link}
{kind=link}
{kind=link}
Log rank survival of patients with (A) %CD4+ PLY ⩽30% (n=14) or >30% (n=12) and (B) %CD8+ PLY ⩾35% (n=11) or <35% (n=15) in 26 patients with stage IA and IB lung cancer.
An examination of other factors that correlated with prognosis is shown in table 2. In addition to proportions of CD4+ PLY and CD8+ PLY, p factor, nodal status, and clinical stage were significantly associated with the prognosis.
Univariate survival analysis of patients with lung cancer
Multivariate analysis (Cox proportional hazard models) clearly demonstrated that the proportion of CD4+ PLY and nodal status were the most important prognostic factors (table 3), and they were independently associated with the prognosis of the patients with lung cancer.
Multivariate survival analysis of patients with lung cancer based on Cox's hazard regression model
Discussion
Lung cancer patients with %CD4+ PLY ⩽30% are associated with a favourable prognosis. Multivariate analysis shows that the proportion of CD4+ PLY and nodal status are significant and independent prognostic factors for the survival of patients with lung cancer. Moreover, the proportion of CD4+ PLY can serve as a prognostic factor for patients with stage IA and IB non-small cell lung cancer.
The proportion of CD4+ cells in PBL in patients with malignancy decreases according to tumour progression and the decrease in the proportion of CD4+ PBL is associated with a poor prognosis.3-5 In this study, however, we found no significant change in the proportion of CD4+ PBL or CD8+ PBL in lung cancer patients according to tumour progression and the proportion of CD4+ PBL or CD8+ PBL was not associated with the prognosis of the patients with lung cancer (data not shown). Our subjects were patients with resectable non-small cell lung cancer. The proportion of CD4+ PBL or CD8+ PBL might be associated with the prognosis of the lung cancer patients with distant metastasis. Invasion of lung cancer cells into the pleural cavity may affect the nature of the PLY and distant metastasis of lung cancer cells may affect the nature of PBL.
The proportions of CD4+ and CD8+ tumour infiltrating lymphocytes (TIL) are similar to those in PBL of patients with malignancy.22-25 In lung cancer patients, however, the proportion of CD8+ TIL is significantly higher than that of CD8+ PBL.26 ,27 The proportion of CD4+ TIL increases and that of CD8+ TIL decreases according to tumour progression in patients with malignancy.22-27 The increase in the proportion of CD4+ TIL and the decrease in the proportion of CD8+ TIL are associated with a poor prognosis.22-27 In malignant peritoneal fluid the proportion of CD8+ lymphocytes decreases with progression of cancer cells.28 Following the changes in the population of lymphocytes in the peritoneal fluid of cancer patients may be useful for determining the prognosis.29
CD4+ lymphocytes can directly lyse tumour cells in an HLA class II restricted fashion.30 ,31 Most tumour specific CD4+ TIL and CD4+ lymphocytes in malignant peritoneal fluid may recognise tumour antigens presented on HLA class II molecules. CD4+ TIL and CD4+ lymphocytes in malignant peritoneal fluid of cancer patients may therefore play an important role in tumour regression mediated by the immune system. In malignant pleural effusions CD4+ PLY are dominant.12-15 By contrast, the proportion of CD4+ PLY in lung cancer patients without malignant pleural effusions is significantly lower than that of CD8+ PLY.16 ,17 In the pleural cavity changes in the population of lymphocytes may also occur according to tumour progression, as occurs in the tumour and the peritoneal cavity. The majority of tumour specific CD4+ PLY may also recognise tumour antigens presented on HLA class II molecules. These facts suggest that CD4+ PLY of lung cancer patients may play an important role in tumour regression, as do TIL and lymphocytes in malignant peritoneal fluid. The key to inducing the most potent killing response to a tumour is therefore the activation of CD4+ lymphocytes.
CD4+ PLY may be used diagnostically to select patients who are likely to have a poorer prognosis after surgery. How cancer cells invade the pleural cavity is still unknown. We believe that the most likely mechanism is by spread through lymphatic vessels. Cytological examination of pleural effusions or pleural lavage fluid would seem to be an important method for detecting invasion of lung cancer cells, but recognition of lung cancer cells by PLY might be more sensitive than cytological examination.
In conclusion, our retrospective study indicates that estimation of the proportion of CD4+ PLY is useful as a clinical biomarker which is related to the outcome of patients with resectable non-small cell lung cancer. If the current findings can be confirmed in large prospective studies, then measurement of the proportion of CD4+ PLY may become a useful clinical tool to select patients who are likely to have a poorer prognosis after surgery and who may be suitable for consideration of adjuvant treatments.